

MET increased gene copy number and primary resistance to gefitinib therapy in non-small-cell lung cancer patients
- PMID: 18836087
- PMCID: PMC2733067
- DOI: 10.1093/annonc/mdn635
MET increased gene copy number and primary resistance to gefitinib therapy in non-small-cell lung cancer patients
Abstract
Background: MET amplification has been detected in approximately 20% of non-small-cell lung cancer patients (NSCLC) with epidermal growth factor receptor (EGFR) mutations progressing after an initial response to tyrosine kinase inhibitor (TKI) therapy.
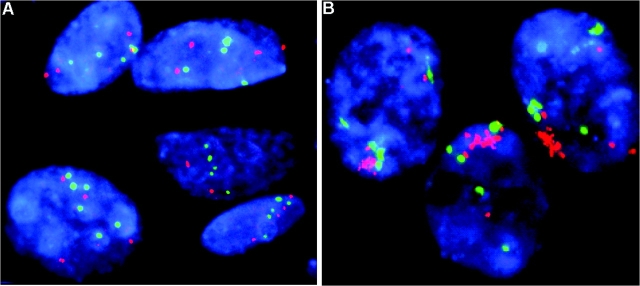
Patients and methods: We analyzed MET gene copy number using FISH in two related NSCLC cell lines, one sensitive (HCC827) and one resistant (HCC827 GR6) to gefitinib therapy and in two different NSCLC patient populations: 24 never smokers or EGFR FISH-positive patients treated with gefitinib (ONCOBELL cohort) and 182 surgically resected NSCLC not exposed to anti-EGFR agents.
Results: HCC827 GR6-resistant cell line displayed MET amplification, with a mean MET copy number >12, while sensitive HCC827 cell line had a mean MET copy number of 4. In the ONCOBELL cohort, no patient had gene amplification and MET gene copy number was not associated with outcome to gefitinib therapy. Among the surgically resected patients, MET was amplified in 12 cases (7.3%) and only four (2.4%) had a higher MET copy number than the resistant HCC827 GR6 cell line.
Conclusions: MET gene amplification is a rare event in patients with advanced NSCLC. The development of anti-MET therapeutic strategies should be focused on patients with acquired EGFR-TKI resistance.
Figures

Similar articles
-
MET gene copy number in non-small cell lung cancer: molecular analysis in a targeted tyrosine kinase inhibitor naïve cohort.J Thorac Oncol. 2008 Apr;3(4):331-9. doi: 10.1097/JTO.0b013e318168d9d4. J Thorac Oncol. 2008. PMID: 18379349
-
Effects of Src inhibitors on cell growth and epidermal growth factor receptor and MET signaling in gefitinib-resistant non-small cell lung cancer cells with acquired MET amplification.Cancer Sci. 2010 Jan;101(1):167-72. doi: 10.1111/j.1349-7006.2009.01368.x. Epub 2009 Sep 14. Cancer Sci. 2010. PMID: 19804422 Free PMC article.
-
Clinical implications of high MET gene dosage in non-small cell lung cancer patients without previous tyrosine kinase inhibitor treatment.J Thorac Oncol. 2011 Dec;6(12):2027-35. doi: 10.1097/JTO.0b013e3182307e92. J Thorac Oncol. 2011. PMID: 22052229
-
Erlotinib or gefitinib for the treatment of relapsed platinum pretreated non-small cell lung cancer and ovarian cancer: a systematic review.Drug Resist Updat. 2011 Jun;14(3):177-90. doi: 10.1016/j.drup.2011.02.004. Epub 2011 Mar 24. Drug Resist Updat. 2011. PMID: 21435938 Review.
-
Activating and resistance mutations of EGFR in non-small-cell lung cancer: role in clinical response to EGFR tyrosine kinase inhibitors.Oncogene. 2009 Aug;28 Suppl 1(Suppl 1):S24-31. doi: 10.1038/onc.2009.198. Oncogene. 2009. PMID: 19680293 Free PMC article. Review.
Cited by
-
MET nucleotide variations and amplification in advanced ovarian cancer: characteristics and outcomes with c-Met inhibitors.Oncoscience. 2013 Dec 11;1(1):5-13. doi: 10.18632/oncoscience.3. eCollection 2014. Oncoscience. 2013. PMID: 25593979 Free PMC article.
-
Molecular mechanisms contributing to resistance to tyrosine kinase-targeted therapy for non-small cell lung cancer.Cancer Biol Med. 2012 Mar;9(1):18-22. doi: 10.3969/j.issn.2095-3941.2012.01.003. Cancer Biol Med. 2012. PMID: 23691449 Free PMC article.
-
Targeted sequencing identifies genetic alterations that confer primary resistance to EGFR tyrosine kinase inhibitor (Korean Lung Cancer Consortium).Oncotarget. 2016 Jun 14;7(24):36311-36320. doi: 10.18632/oncotarget.8904. Oncotarget. 2016. PMID: 27121209 Free PMC article.
-
Successful Treatment with Crizotinib to Overcome Drug Resistance Possibly Due to Mesenchymal-epithelial Transition Amplification in a Lung Cancer Patient with the Echinoderm Microtubule-associated Protein-like 4-anaplastic Lymphoma Kinase Fusion Gene.Intern Med. 2023 Nov 1;62(21):3215-3221. doi: 10.2169/internalmedicine.1164-22. Epub 2023 Mar 15. Intern Med. 2023. PMID: 36927974 Free PMC article.
-
Comparison of in situ and extraction-based methods for the detection of MET amplifications in solid tumors.Comput Struct Biotechnol J. 2019 Sep 11;17:1339-1347. doi: 10.1016/j.csbj.2019.09.003. eCollection 2019. Comput Struct Biotechnol J. 2019. PMID: 31762957 Free PMC article.
References
-
- Paez JG, Janne PA, Lee JC, et al. EGFR mutations in lung cancer: correlation with clinical response to gefitinib therapy. Science. 2004;304:1497–1500. - PubMed
-
- Tsao MS, Sakurada A, Cutz JC, et al. Erlotinib in lung cancer molecular and clinical predictors of outcome. N Engl J Med. 2005;353:133–144. - PubMed
-
- Hirsch FR, Varella-Garcia M, Bunn PA, Jr, et al. Molecular predictors of outcome with gefitinib in a phase III placebo-controlled study in advanced non-small-cell lung cancer. J Clin Oncol. 2006;24:5034–5042. - PubMed
-
- Cappuzzo F, Hirsch FR, Rossi E, et al. Epidermal growth factor receptor gene and protein and gefitinib sensitivity in non-small cell lung cancer. J Natl Cancer Inst. 2005;97:643–655. - PubMed
-
- Cappuzzo F, Ligorio C, Janne PA, et al. Prospective study of gefitinib in EGFR FISH positive/P-Akt positive or never smoker patients with advanced non-small cell lung cancer (NSCLC): the ONCOBELL trial. J Clin Oncol. 2007;25:2248–2255. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous
