

Determinants of the accuracy of rapid diagnostic tests in malaria case management: evidence from low and moderate transmission settings in the East African highlands
- PMID: 18834523
- PMCID: PMC2571107
- DOI: 10.1186/1475-2875-7-202
Determinants of the accuracy of rapid diagnostic tests in malaria case management: evidence from low and moderate transmission settings in the East African highlands
Abstract
Background: The accuracy of malaria diagnosis has received renewed interest in recent years due to changes in treatment policies in favour of relatively high-cost artemisinin-based combination therapies. The use of rapid diagnostic tests (RDTs) based on histidine-rich protein 2 (HRP2) synthesized by Plasmodium falciparum has been widely advocated to save costs and to minimize inappropriate treatment of non-malarial febrile illnesses. HRP2-based RDTs are highly sensitive and stable; however, their specificity is a cause for concern, particularly in areas of intense malaria transmission due to persistence of HRP2 antigens from previous infections.
Methods: In this study, 78,454 clinically diagnosed malaria patients were tested using HRP2-based RDTs over a period of approximately four years in four highland sites in Kenya and Uganda representing hypoendemic to mesoendemic settings. In addition, the utility of the tests was evaluated in comparison with expert microscopy for disease management in 2,241 subjects in two sites with different endemicity levels over four months.
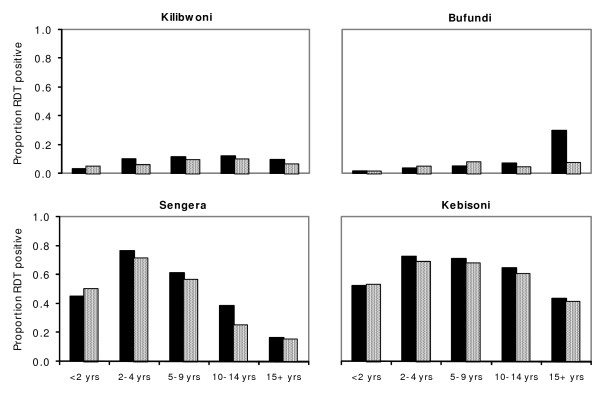
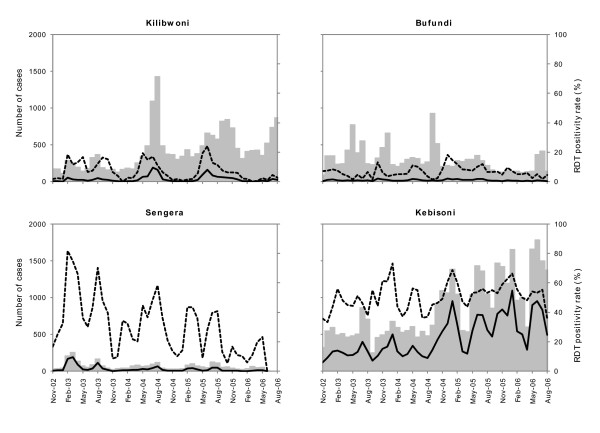
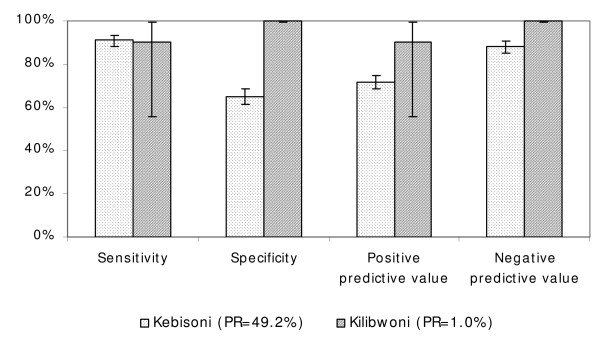
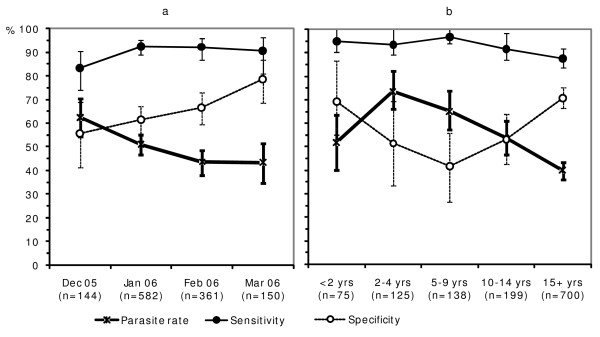
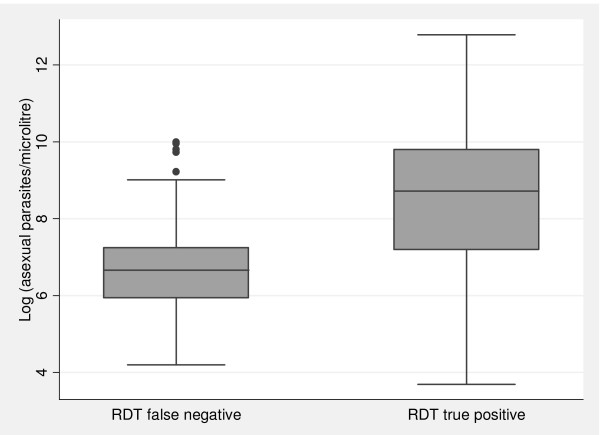
Results: RDT positivity rates varied by season and year, indicating temporal changes in accuracy of clinical diagnosis. Compared to expert microscopy, the sensitivity, specificity, positive predictive value and negative predictive value of the RDTs in a hypoendemic site were 90.0%, 99.9%, 90.0% and 99.9%, respectively. Corresponding measures at a mesoendemic site were 91.0%, 65.0%, 71.6% and 88.1%. Although sensitivities at the two sites were broadly comparable, levels of specificity varied considerably between the sites as well as according to month of test, age of patient, and presence or absence of fever during consultation. Specificity was relatively high in older age groups and increased towards the end of the transmission season, indicating the role played by anti-HRP2 antibodies. Patients with high parasite densities were more likely to test positive with RDTs than those with low density infections.
Conclusion: RDTs may be effective when used in low endemicity situations, but high false positive error rates may occur in areas with moderately high transmission. Reports on specificity of RDTs and cost-effectiveness analyses on their use should be interpreted with caution as there may be wide variations in these measurements depending upon endemicity, season and the age group of patients studied.
Figures
Similar articles
-
Rapid diagnostic tests for malaria at sites of varying transmission intensity in Uganda.J Infect Dis. 2008 Feb 15;197(4):510-8. doi: 10.1086/526502. J Infect Dis. 2008. PMID: 18240951
-
Comparison of HRP2- and pLDH-based rapid diagnostic tests for malaria with longitudinal follow-up in Kampala, Uganda.Am J Trop Med Hyg. 2007 Jun;76(6):1092-7. Am J Trop Med Hyg. 2007. PMID: 17556616
-
Operational accuracy and comparative persistent antigenicity of HRP2 rapid diagnostic tests for Plasmodium falciparum malaria in a hyperendemic region of Uganda.Malar J. 2008 Oct 29;7:221. doi: 10.1186/1475-2875-7-221. Malar J. 2008. PMID: 18959777 Free PMC article.
-
Malaria rapid diagnostic tests in endemic settings.Clin Microbiol Infect. 2013 May;19(5):399-407. doi: 10.1111/1469-0691.12151. Epub 2013 Feb 25. Clin Microbiol Infect. 2013. PMID: 23438048 Review.
-
Malaria rapid diagnostic tests in travel medicine.Clin Microbiol Infect. 2013 May;19(5):408-15. doi: 10.1111/1469-0691.12152. Epub 2013 Feb 1. Clin Microbiol Infect. 2013. PMID: 23373854 Review.
Cited by
-
Standardizing Plasmodium falciparum infection prevalence measured via microscopy versus rapid diagnostic test.Malar J. 2015 Nov 17;14:460. doi: 10.1186/s12936-015-0984-9. Malar J. 2015. PMID: 26577805 Free PMC article.
-
Diagnostic performance of an ultrasensitive HRP2-based malaria rapid diagnostic test kit used in surveys of afebrile people living in Southern Ghana.Malar J. 2021 Mar 2;20(1):125. doi: 10.1186/s12936-021-03665-7. Malar J. 2021. PMID: 33653356 Free PMC article.
-
Evaluation of Paracheck-Pf(TM) rapid malaria diagnostic test for the diagnosis of malaria among HIV-positive patients in Ibadan, south-western Nigeria.Pathog Glob Health. 2013 Mar;107(2):69-77. doi: 10.1179/2047773213Y.0000000077. Pathog Glob Health. 2013. PMID: 23683333 Free PMC article.
-
Overdiagnosis of Malaria Illness in an Endemic Setting: A Facility-Based Surveillance Study in Malawi.Am J Trop Med Hyg. 2021 May 3;104(6):2123-2130. doi: 10.4269/ajtmh.20-1209. Am J Trop Med Hyg. 2021. PMID: 33939628 Free PMC article.
-
Implementation of the integrated management of childhood illness with parasitological diagnosis of malaria in rural Ghana: health worker perceptions.Malar J. 2015 Apr 23;14:174. doi: 10.1186/s12936-015-0699-y. Malar J. 2015. PMID: 25899509 Free PMC article.
References
-
- Wongsrichanalai C, Barcus MJ, Muth S, Sutamihardja A, Wernsdorfer WH. A review of malaria diagnostic tools: microscopy and rapid diagnostic test (RDT) Am J Trop Med Hyg. 2007;77:119–127. - PubMed
-
- WHO . The Role of Laboratory Diagnosis to Support Malaria Disease Management: Report of a WHO Technical Consultation, 25–26 October Report No WHO/HTM/MAL/20061111. Geneva: World Health Organization; 2004.
-
- Hopkins H, Kambale W, Kamya MR, Staedke SG, Dorsey G, Rosenthal PJ. Comparison of HRP2- and pLDH-based rapid diagnostic tests for malaria with longitudinal follow-up in Kampala, Uganda. Am J Trop Med Hyg. 2007;76:1092–1097. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
