

Efavirenz versus nevirapine-based initial treatment of HIV infection: clinical and virological outcomes in Southern African adults
- PMID: 18832875
- PMCID: PMC2659649
- DOI: 10.1097/QAD.0b013e328310407e
Efavirenz versus nevirapine-based initial treatment of HIV infection: clinical and virological outcomes in Southern African adults
Abstract
Objective: To determine the effectiveness of efavirenz versus nevirapine in initial antiretroviral therapy regimens for adults in sub-Saharan Africa.
Design: Observational cohort study.
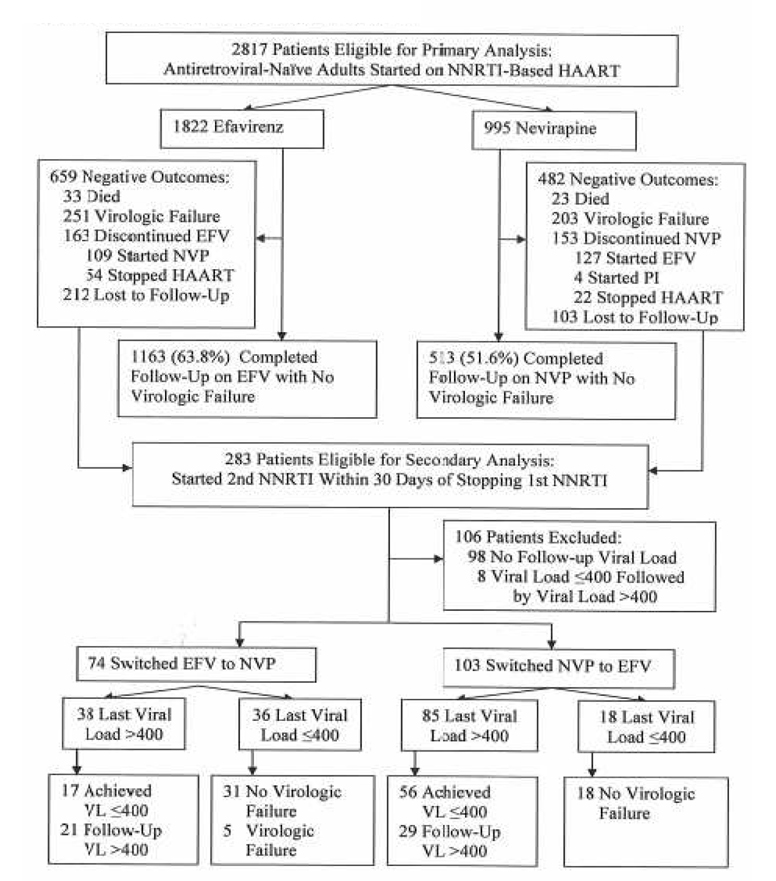
Methods: Study participants were 2817 HIV-infected, highly active antiretroviral therapy-naive adults who began nevirapine-based or efavirenz-based highly active antiretroviral therapy between January 1998 and September 2004 via a private-sector HIV/AIDS program in nine countries of southern Africa. The primary outcome was time to virologic failure (two measurements of viral loads >or=400 copies/ml). Secondary outcomes included all-cause mortality, time to viral load less than 400 copies/ml, pharmacy-claim adherence, and discontinuation of nevirapine or efavirenz without virologic failure.
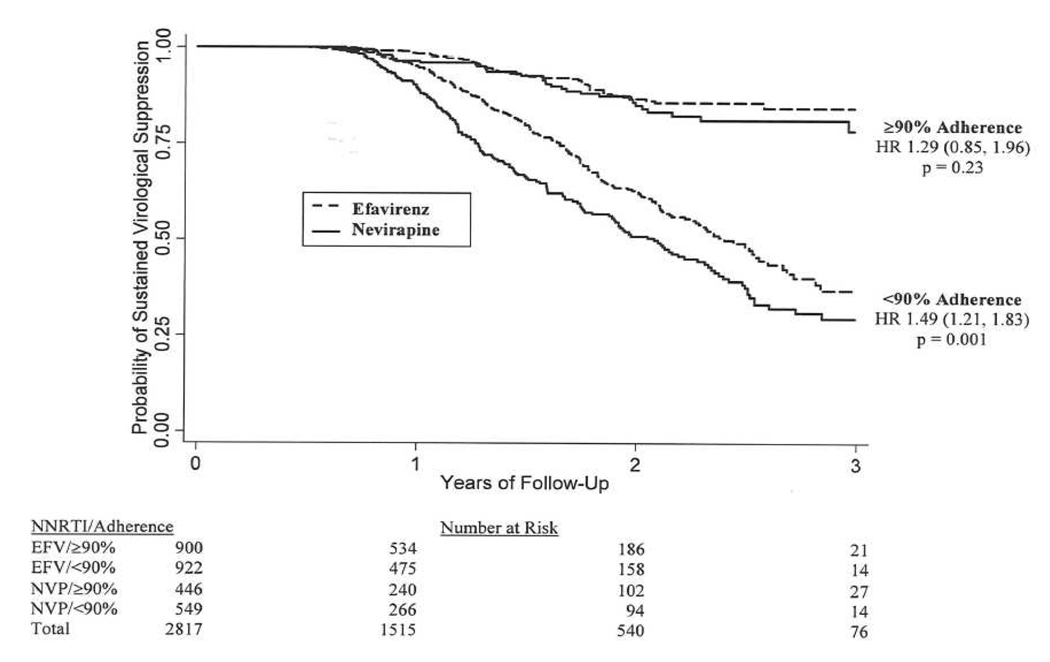
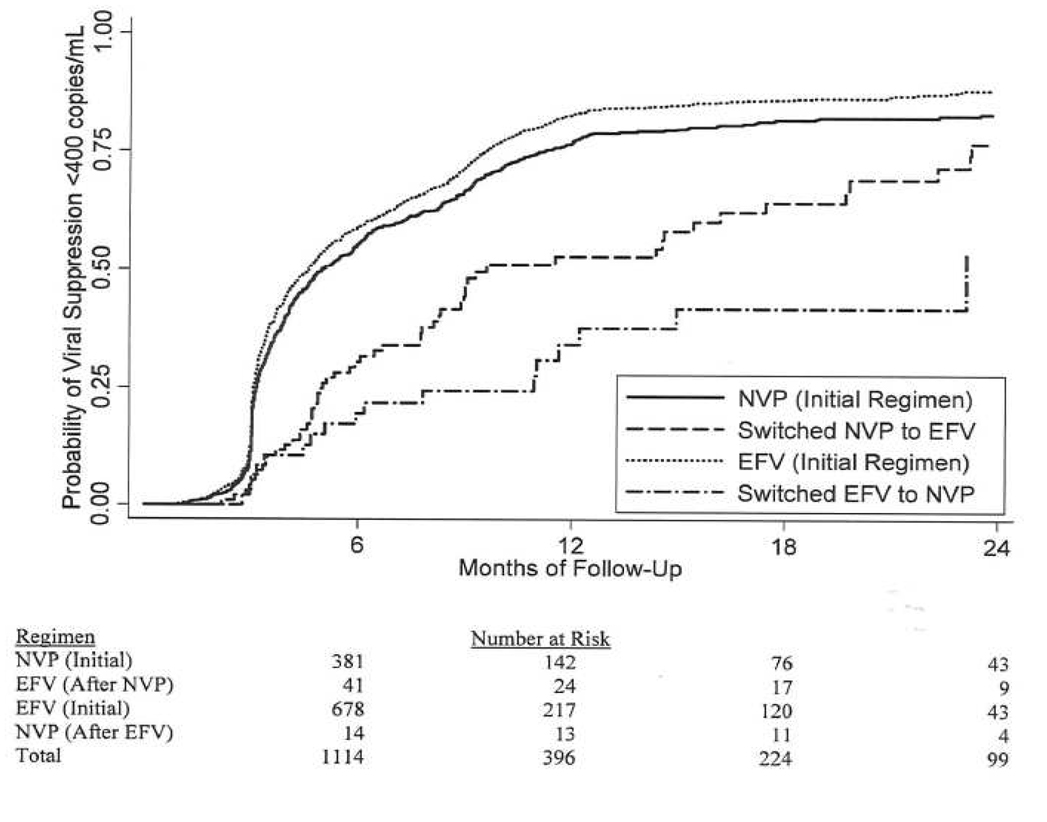
Results: The median follow-up period was 2.0 years (interquartile range 1.2-2.6). Patients started on nevirapine were significantly less likely than those started on efavirenz to achieve high adherence, whether defined as 100% (30.2 versus 38.1%, P < 0.002) or more than 90% (44.8 versus 49.4%, P < 0.02) pharmacy-claim adherence. In a multivariate analysis, patients on nevirapine had greater risk of virologic failure [hazard ratio (HR 1.52; 95% confidence interval (CI) 1.24-1.86)], death (2.17; 1.31-3.60), and regimen discontinuation (1.67; 1.32-2.11). Switching from nevirapine to efavirenz had no significant virologic effect, whereas switching from efavirenz to nevirapine resulted in significantly slower time to suppression (hazard ratio 0.58, 95% confidence interval 0.35-0.93) and faster time to failure (hazard ratio 3.92; 95% confidence interval 1.61-9.55) than remaining on efavirenz.
Conclusion: In initial highly active antiretroviral therapy regimens, efavirenz was associated with superior virologic and clinical outcomes than nevirapine, suggesting that efavirenz might be the preferred nonnucleoside reverse transcriptase inhibitor in resource-limited settings. However, its higher cost and potential teratogenicity are important barriers to implementation.
Conflict of interest statement
Conflict of interest
Consultant: R.E. Chaisson (Bristol-Myers Squibb). Consultant and/or honorarium: J.B. Nachega (GlaxoSmithKline, Merck-Sharp-Dohme) and G. Maartens (Merck-Sharp-Dohme). Grants received: G. Maartens (Merck-Sharp-Dohme). Other: J.B. Nachega (Aspen Pharmaceuticals); J.E. Gallant: Grants/Research Support (Gilead Sciences, GlaxoSmithKline, Merck, Pfizer, Roche, Tibotec), consultant and/or honorarium (Bristol Myers Squibb, Gilead Sciences, Roche, Abbott Laboratories, GlaxoSmithKline, Merck, Schering Plough, Pfizer, Tibotec).
Figures
Similar articles
-
Outcomes of nevirapine- and efavirenz-based antiretroviral therapy when coadministered with rifampicin-based antitubercular therapy.JAMA. 2008 Aug 6;300(5):530-9. doi: 10.1001/jama.300.5.530. JAMA. 2008. PMID: 18677025
-
Adherence to nonnucleoside reverse transcriptase inhibitor-based HIV therapy and virologic outcomes.Ann Intern Med. 2007 Apr 17;146(8):564-73. doi: 10.7326/0003-4819-146-8-200704170-00007. Ann Intern Med. 2007. PMID: 17438315
-
A randomized trial comparing plasma drug concentrations and efficacies between 2 nonnucleoside reverse-transcriptase inhibitor-based regimens in HIV-infected patients receiving rifampicin: the N2R Study.Clin Infect Dis. 2009 Jun 15;48(12):1752-9. doi: 10.1086/599114. Clin Infect Dis. 2009. PMID: 19438397 Clinical Trial.
-
Nevirapine versus efavirenz for patients co-infected with HIV and tuberculosis: a systematic review and meta-analysis.Int J Infect Dis. 2014 Aug;25:130-5. doi: 10.1016/j.ijid.2014.04.020. Epub 2014 Jun 6. Int J Infect Dis. 2014. PMID: 24911886 Review.
-
Efavirenz or nevirapine in three-drug combination therapy with two nucleoside or nucleotide-reverse transcriptase inhibitors for initial treatment of HIV infection in antiretroviral-naïve individuals.Cochrane Database Syst Rev. 2016 Dec 10;12(12):CD004246. doi: 10.1002/14651858.CD004246.pub4. Cochrane Database Syst Rev. 2016. PMID: 27943261 Free PMC article. Review.
Cited by
-
Projecting the clinical benefits and risks of using efavirenz-containing antiretroviral therapy regimens in women of childbearing age.AIDS. 2012 Mar 13;26(5):625-34. doi: 10.1097/QAD.0b013e328350fbfb. AIDS. 2012. PMID: 22398569 Free PMC article.
-
Comparative durability of nevirapine versus efavirenz in first-line regimens during the first year of initiating antiretroviral therapy among Swaziland HIV-infected adults.Pan Afr Med J. 2013 May 3;15:5. doi: 10.11604/pamj.2013.15.5.1889. Print 2013. Pan Afr Med J. 2013. PMID: 23847702 Free PMC article.
-
Effectiveness of efavirenz-based regimens in young HIV-infected children treated for tuberculosis: a treatment option for resource-limited settings.PLoS One. 2013;8(1):e55111. doi: 10.1371/journal.pone.0055111. Epub 2013 Jan 25. PLoS One. 2013. PMID: 23372824 Free PMC article.
-
Combination of metformin/efavirenz/fluoxetine exhibits profound anticancer activity via a cancer cell-specific ROS amplification.Cancer Biol Ther. 2023 Dec 31;24(1):20-32. doi: 10.1080/15384047.2022.2161803. Cancer Biol Ther. 2023. PMID: 36588385 Free PMC article.
-
Antiretroviral therapy for treatment-naïve patients: a review of recent literature and the updated guidelines.Curr Infect Dis Rep. 2009 Jul;11(4):311-8. doi: 10.1007/s11908-009-0046-y. Curr Infect Dis Rep. 2009. PMID: 19545501
References
-
- World Health Organization (WHO) Scaling up antiretroviral therapy in resource-limited settings: treatment guidelines for a public health approach. 2006 Revision. Geneva: WHO; 2006.
-
- Gilks CF, Crowley S, Ekpini R, Gove S, Perriens J, Souteyrand Y, et al. The WHO public-health approach to antiretroviral treatment against HIV in resource-limited settings. Lancet. 2006;368:505–510. - PubMed
-
- Van Leth P, Phanuphak P, Ruxrungtham K, Baraldi E, Miller S, Gazzard B, et al. for the 2NN Study Team. Comparison of first-line antiretroviral therapy with regimens including nevirapine, efavirenz, or both drugs, plus stavudine and lamivudine: A randomised open-label trial, the 2NN Study. Lancet. 2004;363:1253–1263. - PubMed
-
- The Antiretroviral Therapy Cohort Collaboration (ART-CC) Rates of disease progression according to initial highly active antiretroviral therapy regimen: A collaborative analysis of 12 prospective cohort studies. J Infect Dis. 2006;194:612–622. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
