

Prevention and treatment of pediatric obesity: an endocrine society clinical practice guideline based on expert opinion
- PMID: 18782869
- PMCID: PMC6048599
- DOI: 10.1210/jc.2007-2458
Prevention and treatment of pediatric obesity: an endocrine society clinical practice guideline based on expert opinion
Erratum in
-
Corrigendum to: "Prevention and Treatment of Pediatric Obesity: An Endocrine Society Clinical Practice Guideline Based on Expert Opinion".J Clin Endocrinol Metab. 2021 Jun 16;106(7):e2846. doi: 10.1210/clinem/dgab309. J Clin Endocrinol Metab. 2021. PMID: 33999174 Free PMC article. No abstract available.
Abstract
Objective: Our objective was to formulate practice guidelines for the treatment and prevention of pediatric obesity.
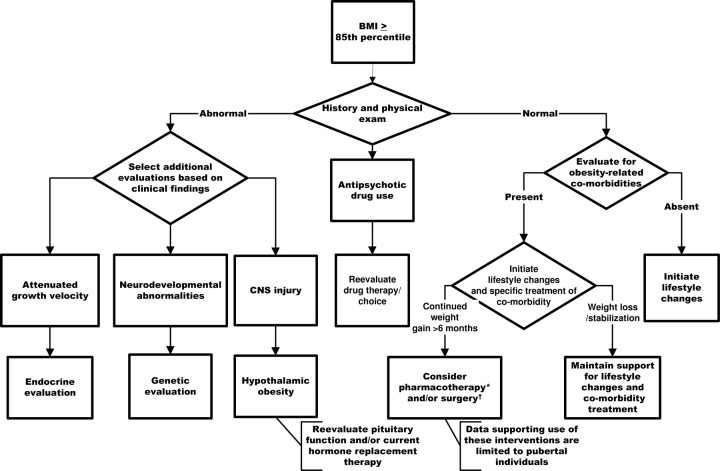
Conclusions: We recommend defining overweight as body mass index (BMI) in at least the 85th percentile but < the 95th percentile and obesity as BMI in at least the 95th percentile against routine endocrine studies unless the height velocity is attenuated or inappropriate for the family background or stage of puberty; referring patients to a geneticist if there is evidence of a genetic syndrome; evaluating for obesity-associated comorbidities in children with BMI in at least the 85th percentile; and prescribing and supporting intensive lifestyle (dietary, physical activity, and behavioral) modification as the prerequisite for any treatment. We suggest that pharmacotherapy (in combination with lifestyle modification) be considered in: 1) obese children only after failure of a formal program of intensive lifestyle modification; and 2) overweight children only if severe comorbidities persist despite intensive lifestyle modification, particularly in children with a strong family history of type 2 diabetes or premature cardiovascular disease. Pharmacotherapy should be provided only by clinicians who are experienced in the use of antiobesity agents and aware of the potential for adverse reactions. We suggest bariatric surgery for adolescents with BMI above 50 kg/m(2), or BMI above 40 kg/m(2) with severe comorbidities in whom lifestyle modifications and/or pharmacotherapy have failed. Candidates for surgery and their families must be psychologically stable and capable of adhering to lifestyle modifications. Access to experienced surgeons and sophisticated multidisciplinary teams who assess the benefits and risks of surgery is obligatory. We emphasize the prevention of obesity by recommending breast-feeding of infants for at least 6 months and advocating that schools provide for 60 min of moderate to vigorous daily exercise in all grades. We suggest that clinicians educate children and parents through anticipatory guidance about healthy dietary and activity habits, and we advocate for restricting the availability of unhealthy food choices in schools, policies to ban advertising unhealthy food choices to children, and community redesign to maximize opportunities for safe walking and bike riding to school, athletic activities, and neighborhood shopping.
Figures
Similar articles
-
Pediatric Obesity-Assessment, Treatment, and Prevention: An Endocrine Society Clinical Practice Guideline.J Clin Endocrinol Metab. 2017 Mar 1;102(3):709-757. doi: 10.1210/jc.2016-2573. J Clin Endocrinol Metab. 2017. PMID: 28359099 Free PMC article.
-
The effectiveness of web-based programs on the reduction of childhood obesity in school-aged children: A systematic review.JBI Libr Syst Rev. 2012;10(42 Suppl):1-14. doi: 10.11124/jbisrir-2012-248. JBI Libr Syst Rev. 2012. PMID: 27820152
-
Obesity in Adolescents: A Review.JAMA. 2024 Sep 3;332(9):738-748. doi: 10.1001/jama.2024.11809. JAMA. 2024. PMID: 39102244 Review.
-
Family Based Prevention of Cardiovascular Disease Risk Factors in Children by Lifestyle Change: The PEP Family Heart Study.Adv Exp Med Biol. 2019;1121:41-55. doi: 10.1007/978-3-030-10616-4_5. Adv Exp Med Biol. 2019. PMID: 31392651
-
The effect of weight management interventions that include a diet component on weight-related outcomes in pregnant and postpartum women: a systematic review protocol.JBI Database System Rev Implement Rep. 2015 Jan;13(1):88-98. doi: 10.11124/jbisrir-2015-1812. JBI Database System Rev Implement Rep. 2015. PMID: 26447010
Cited by
-
Endocrine check-up in adolescents and indications for referral: A guide for health care providers.Indian J Endocrinol Metab. 2014 Nov;18(Suppl 1):S26-38. doi: 10.4103/2230-8210.145055. Indian J Endocrinol Metab. 2014. PMID: 25538875 Free PMC article. Review.
-
Lifestyle intervention in childhood obesity: changes and challenges.Nat Rev Endocrinol. 2013 Oct;9(10):607-14. doi: 10.1038/nrendo.2013.149. Epub 2013 Jul 30. Nat Rev Endocrinol. 2013. PMID: 23897171 Review.
-
Waist circumference measurement site does not affect relationships with visceral adiposity and cardiometabolic risk factors in children.Pediatr Obes. 2013 Jun;8(3):199-206. doi: 10.1111/j.2047-6310.2012.00106.x. Epub 2012 Nov 21. Pediatr Obes. 2013. PMID: 23172858 Free PMC article.
-
A clinic-based lifestyle intervention for pediatric obesity: efficacy and behavioral and biochemical predictors of response.J Pediatr Endocrinol Metab. 2009 Sep;22(9):805-14. doi: 10.1515/jpem.2009.22.9.805. J Pediatr Endocrinol Metab. 2009. PMID: 19960890 Free PMC article.
-
Exercise in the treatment of childhood obesity.Turk Pediatri Ars. 2020 Mar 9;55(1):2-10. doi: 10.14744/TurkPediatriArs.2019.60430. eCollection 2020. Turk Pediatri Ars. 2020. PMID: 32231444 Free PMC article. Review.
References
-
- Atkins D, Best D, Briss PA, Eccles M, Falck-Ytter Y, Flottorp S, Guyatt GH, Harbour RT, Haugh MC, Henry D, Hill S, Jaeschke R, Leng G, Liberati A, Magrini N, Mason J, Middleton P, Mrukowicz J, O'Connell D, Oxman AD, Phillips B, Schunemann HJ, Edejer TT, Varonen H, Vist GE, Williams Jr JW, Zaza S. 2004. Grading quality of evidence and strength of recommendations. BMJ 328:1490. - PMC - PubMed
-
- Swiglo BA, Murad MH, Schunemann HJ, Kunz R, Vigersky RA, Guyatt GH, Montori VM. 2008. A case for clarity, consistency, and helpfulness: state-of-the-art clinical practice guidelines in endocrinology using the grading of recommendations, assessment, development, and evaluation system. J Clin Endocrinol Metab 93:666–673 - PubMed
-
- Guyatt G, Gutterman D, Baumann MH, Addrizzo-Harris D, Hylek EM, Phillips B, Raskob G, Lewis SZ, Schunemann H. 2006. Grading strength of recommendations and quality of evidence in clinical guidelines: report from an American College of Chest Physicians task force. Chest 129:174–181 - PubMed
-
- Snow V, Barry P, Fitterman N, Qaseem A, Weiss K. 2005. Pharmacologic and surgical management of obesity in primary care: a clinical practice guideline from the American College of Physicians. Ann Intern Med 142:525–531 - PubMed
-
- NCHS 2005. Prevalence of overweight among children and adolescents: United States, 1999–2002. National Center for Health Statistics; Available at: http://www.cdc.gov/nchs/products/pubs/pubd/hestats/overwght99.htm
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
