

Predicting outcome after traumatic brain injury: development and international validation of prognostic scores based on admission characteristics
- PMID: 18684008
- PMCID: PMC2494563
- DOI: 10.1371/journal.pmed.0050165
Predicting outcome after traumatic brain injury: development and international validation of prognostic scores based on admission characteristics
Abstract
Background: Traumatic brain injury (TBI) is a leading cause of death and disability. A reliable prediction of outcome on admission is of great clinical relevance. We aimed to develop prognostic models with readily available traditional and novel predictors.
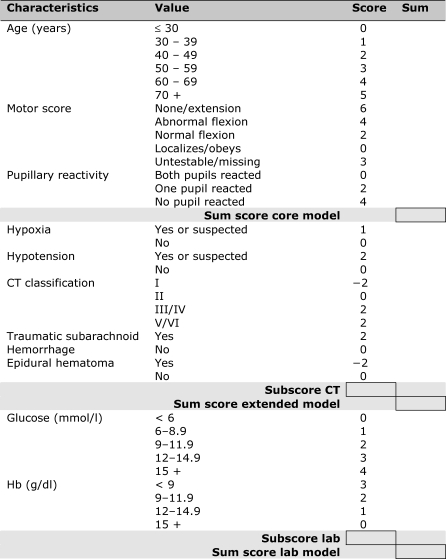
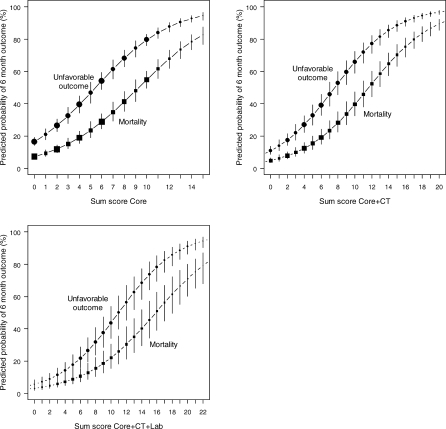
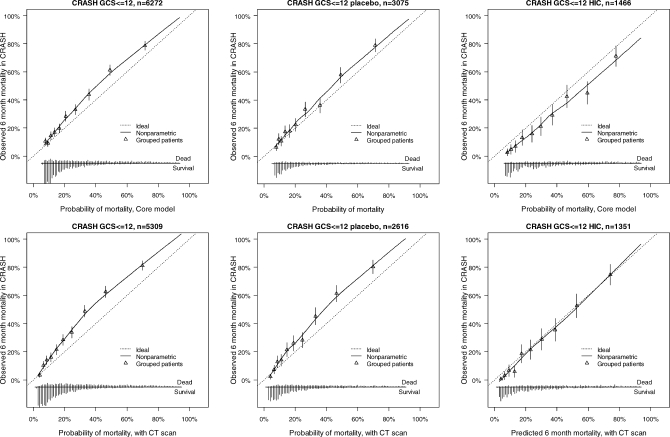
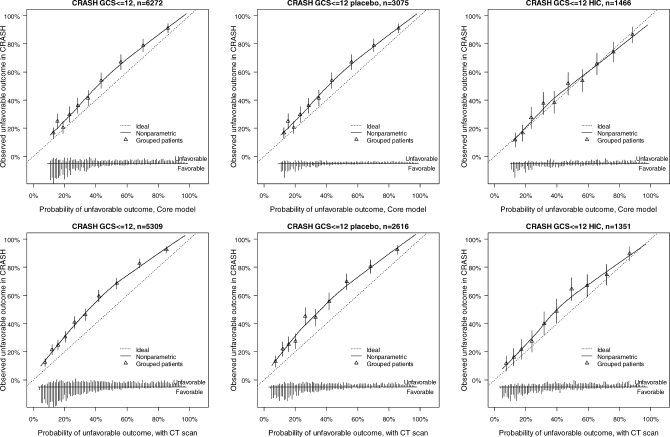
Methods and findings: Prospectively collected individual patient data were analyzed from 11 studies. We considered predictors available at admission in logistic regression models to predict mortality and unfavorable outcome according to the Glasgow Outcome Scale at 6 mo after injury. Prognostic models were developed in 8,509 patients with severe or moderate TBI, with cross-validation by omission of each of the 11 studies in turn. External validation was on 6,681 patients from the recent Medical Research Council Corticosteroid Randomisation after Significant Head Injury (MRC CRASH) trial. We found that the strongest predictors of outcome were age, motor score, pupillary reactivity, and CT characteristics, including the presence of traumatic subarachnoid hemorrhage. A prognostic model that combined age, motor score, and pupillary reactivity had an area under the receiver operating characteristic curve (AUC) between 0.66 and 0.84 at cross-validation. This performance could be improved (AUC increased by approximately 0.05) by considering CT characteristics, secondary insults (hypotension and hypoxia), and laboratory parameters (glucose and hemoglobin). External validation confirmed that the discriminative ability of the model was adequate (AUC 0.80). Outcomes were systematically worse than predicted, but less so in 1,588 patients who were from high-income countries in the CRASH trial.
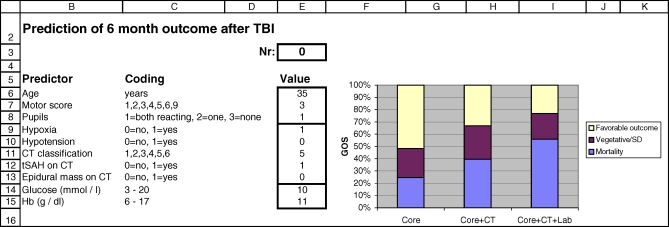
Conclusions: Prognostic models using baseline characteristics provide adequate discrimination between patients with good and poor 6 mo outcomes after TBI, especially if CT and laboratory findings are considered in addition to traditional predictors. The model predictions may support clinical practice and research, including the design and analysis of randomized controlled trials.
Conflict of interest statement
Figures
Comment in
-
Developing a prognostic model for traumatic brain injury--a missed opportunity?PLoS Med. 2008 Aug 5;5(8):e168. doi: 10.1371/journal.pmed.0050168. PLoS Med. 2008. PMID: 18684010 Free PMC article.
Similar articles
-
Validation of a prognostic score for early mortality in severe head injury cases.J Neurosurg. 2014 Dec;121(6):1314-22. doi: 10.3171/2014.7.JNS131874. Epub 2014 Sep 19. J Neurosurg. 2014. PMID: 25237737
-
Predicting outcome after traumatic brain injury: development and validation of a prognostic score based on admission characteristics.J Neurotrauma. 2005 Oct;22(10):1025-39. doi: 10.1089/neu.2005.22.1025. J Neurotrauma. 2005. PMID: 16238481
-
Prediction of outcome after moderate and severe traumatic brain injury: external validation of the International Mission on Prognosis and Analysis of Clinical Trials (IMPACT) and Corticoid Randomisation After Significant Head injury (CRASH) prognostic models.Crit Care Med. 2012 May;40(5):1609-17. doi: 10.1097/CCM.0b013e31824519ce. Crit Care Med. 2012. PMID: 22511138 Free PMC article.
-
Predicting outcome after traumatic brain injury.Handb Clin Neurol. 2015;128:455-74. doi: 10.1016/B978-0-444-63521-1.00029-7. Handb Clin Neurol. 2015. PMID: 25701901 Review.
-
A systematic review finds methodological improvements necessary for prognostic models in determining traumatic brain injury outcomes.J Clin Epidemiol. 2008 Apr;61(4):331-43. doi: 10.1016/j.jclinepi.2007.06.011. J Clin Epidemiol. 2008. PMID: 18313557 Review.
Cited by
-
Machine learning predicts improvement of functional outcomes in traumatic brain injury patients after inpatient rehabilitation.Front Rehabil Sci. 2022 Sep 22;3:1005168. doi: 10.3389/fresc.2022.1005168. eCollection 2022. Front Rehabil Sci. 2022. PMID: 36211830 Free PMC article.
-
The Relationship Between Trauma Scoring Systems and Outcomes in Patients With Severe Traumatic Brain Injury.Korean J Neurotrauma. 2022 Oct 13;18(2):169-177. doi: 10.13004/kjnt.2022.18.e54. eCollection 2022 Oct. Korean J Neurotrauma. 2022. PMID: 36381431 Free PMC article.
-
Early prediction of outcome after severe traumatic brain injury: a simple and practical model.BMC Emerg Med. 2016 Aug 24;16(1):32. doi: 10.1186/s12873-016-0098-x. BMC Emerg Med. 2016. PMID: 27553436 Free PMC article. Clinical Trial.
-
Traumatic Brain Injury as an Independent Predictor of Futility in the Early Resuscitation of Patients in Hemorrhagic Shock.J Clin Med. 2024 Jul 3;13(13):3915. doi: 10.3390/jcm13133915. J Clin Med. 2024. PMID: 38999481 Free PMC article. Review.
-
Early diagnosis of mortality using admission CT perfusion in severe traumatic brain injury patients (ACT-TBI): protocol for a prospective cohort study.BMJ Open. 2021 Jun 9;11(6):e047305. doi: 10.1136/bmjopen-2020-047305. BMJ Open. 2021. PMID: 34108167 Free PMC article.
References
-
- Teasdale G, Jennett B. Assessment of coma and impaired consciousness. A practical scale. Lancet. 1974;2:81–84. - PubMed
-
- Jennett B, Bond M. Assessment of outcome after severe brain damage. Lancet. 1975;1:480–484. - PubMed
-
- Jennett B, Teasdale G, Braakman R, Minderhoud J, Knill-Jones R. Predicting outcome in individual patients after severe head injury. Lancet. 1976;1:1031–1034. - PubMed
-
- Machado SG, Murray GD, Teasdale GM. Evaluation of designs for clinical trials of neuroprotective agents in head injury. European Brain Injury Consortium. J Neurotrauma. 1999;16:1131–1138. - PubMed
-
- Hernandez AV, Steyerberg EW, Taylor GS, Marmarou A, Habbema JD, et al. Subgroup analysis and covariate adjustment in randomized clinical trials of traumatic brain injury: a systematic review. Neurosurgery. 2005;57:1244–1253. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
