

RNAi for treating hepatitis B viral infection
- PMID: 18074201
- PMCID: PMC2217617
- DOI: 10.1007/s11095-007-9504-0
RNAi for treating hepatitis B viral infection
Abstract
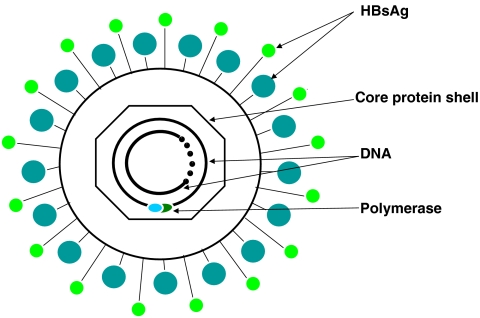
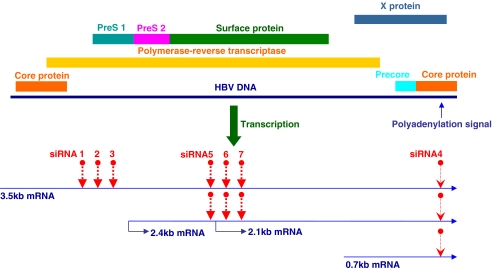
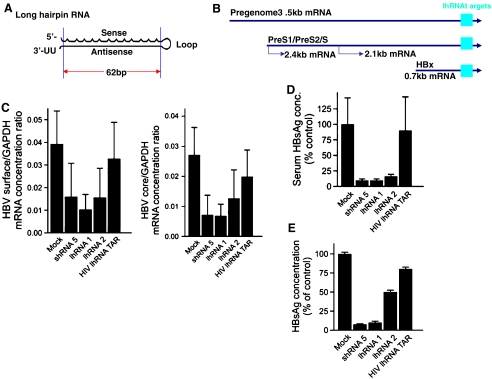
Chronic hepatitis B virus (HBV) infection is one of the leading causes of liver cirrhosis and hepatocellular carcinoma (HCC). Current treatment strategies of HBV infection including the use of interferon (IFN)-alpha and nucleotide analogues such as lamivudine and adefovir have met with only partial success. Therefore, it is necessary to develop more effective antiviral therapies that can clear HBV infection with fewer side effects. RNA interference (RNAi), by which a small interfering RNA (siRNA) induces the gene silence at a post-transcriptional level, has the potential of treating HBV infection. The successful use of chemically synthesized siRNA, endogenous expression of small hairpin RNA (shRNA) or microRNA (miRNA) to silence the target gene make this technology towards a potentially rational therapeutics for HBV infection. However, several challenges including poor siRNA stability, inefficient cellular uptake, widespread biodistribution and non-specific effects need to be overcome. In this review, we discuss several strategies for improving the anti-HBV therapeutic efficacy of siRNAs, while avoiding their off-target effects and immunostimulation. There is an in-depth discussion on the (1) mechanisms of RNAi, (2) methods for siRNA/shRNA production, (3) barriers to RNAi-based therapies, and (4) delivery strategies of siRNA for treating HBV infection.
Figures




Similar articles
-
Countering hepatitis B virus infection using RNAi: how far are we from the clinic?Rev Med Virol. 2011 Nov;21(6):383-96. doi: 10.1002/rmv.705. Epub 2011 Sep 13. Rev Med Virol. 2011. PMID: 21913277 Review.
-
Clearance of hepatitis B virus from the liver of transgenic mice by short hairpin RNAs.Proc Natl Acad Sci U S A. 2005 Jan 18;102(3):773-8. doi: 10.1073/pnas.0409028102. Epub 2005 Jan 7. Proc Natl Acad Sci U S A. 2005. PMID: 15640346 Free PMC article.
-
The short hairpin RNA driven by polymerase II suppresses both wild-type and lamivudine-resistant hepatitis B virus strains.Antivir Ther. 2007;12(6):865-76. Antivir Ther. 2007. PMID: 17926641
-
5'-triphosphate-siRNA activates RIG-I-dependent type I interferon production and enhances inhibition of hepatitis B virus replication in HepG2.2.15 cells.Eur J Pharmacol. 2013 Dec 5;721(1-3):86-95. doi: 10.1016/j.ejphar.2013.09.050. Epub 2013 Oct 5. Eur J Pharmacol. 2013. PMID: 24099962
-
siRNA drug development against hepatitis B virus infection.Expert Opin Biol Ther. 2018 Jun;18(6):609-617. doi: 10.1080/14712598.2018.1472231. Epub 2018 May 8. Expert Opin Biol Ther. 2018. PMID: 29718723 Review.
Cited by
-
Strategies to eliminate HBV infection.Future Virol. 2014;9(6):565-585. doi: 10.2217/fvl.14.36. Future Virol. 2014. PMID: 25309617 Free PMC article.
-
Antiviral treatment of chronic hepatitis B virus (HBV) infections.Viruses. 2010 Jun;2(6):1279-1305. doi: 10.3390/v2061279. Epub 2010 May 31. Viruses. 2010. PMID: 21994680 Free PMC article.
-
Host Transcription Factors in Hepatitis B Virus RNA Synthesis.Viruses. 2020 Jan 30;12(2):160. doi: 10.3390/v12020160. Viruses. 2020. PMID: 32019103 Free PMC article. Review.
-
Drug Delivery Strategies for Antivirals against Hepatitis B Virus.Viruses. 2018 May 17;10(5):267. doi: 10.3390/v10050267. Viruses. 2018. PMID: 29772748 Free PMC article. Review.
-
Eradication Strategies for Chronic Hepatitis B Infection.Clin Infect Dis. 2016 Jun 1;62 Suppl 4(Suppl 4):S318-25. doi: 10.1093/cid/ciw044. Clin Infect Dis. 2016. PMID: 27190322 Free PMC article. Review.
References
-
- {'text': '', 'ref_index': 1, 'ids': [{'type': 'PubMed', 'value': '9392700', 'is_inner': True, 'url': 'https://pubmed.ncbi.nlm.nih.gov/9392700/'}]}
- W. M. Lee. Hepatitis B virus infection. N. Engl. J. Med.337(24):1733–1745 (1997). - PubMed
-
- {'text': '', 'ref_index': 1, 'ids': [{'type': 'PubMed', 'value': '7901639', 'is_inner': True, 'url': 'https://pubmed.ncbi.nlm.nih.gov/7901639/'}]}
- J. Y. Lau and T. L. Wright. Molecular virology and pathogenesis of hepatitis B. Lancet342(8883):1335–1340 (1993). - PubMed
-
- {'text': '', 'ref_index': 1, 'ids': [{'type': 'PubMed', 'value': '1651454', 'is_inner': True, 'url': 'https://pubmed.ncbi.nlm.nih.gov/1651454/'}]}
- J. R. Wands and H. E. Blum. Primary hepatocellular carcinoma. N. Engl. J. Med.325(10):729–731 (1991). - PubMed
-
- {'text': '', 'ref_index': 1, 'ids': [{'type': 'PubMed', 'value': '9352870', 'is_inner': True, 'url': 'https://pubmed.ncbi.nlm.nih.gov/9352870/'}]}
- D. T. Lau, et al. Long-term follow-up of patients with chronic hepatitis B treated with interferon alpha. Gastroenterology113(5):1660–1667 (1997). - PubMed
-
- {'text': '', 'ref_index': 1, 'ids': [{'type': 'PubMed', 'value': '9011789', 'is_inner': True, 'url': 'https://pubmed.ncbi.nlm.nih.gov/9011789/'}]}
- J. H. Hoofnagle and A. M. di Bisceglie. The treatment of chronic viral hepatitis. N. Engl. J. Med.336(5):347–356 (1997). - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
