

Antiretroviral drug exposure in the female genital tract: implications for oral pre- and post-exposure prophylaxis
- PMID: 17721097
- PMCID: PMC2862268
- DOI: 10.1097/QAD.0b013e328270385a
Antiretroviral drug exposure in the female genital tract: implications for oral pre- and post-exposure prophylaxis
Abstract
Objectives: To describe first dose and steady state antiretroviral drug exposure in the female genital tract.
Design: Non-blinded, single center, open-label pharmacokinetic study in HIV-infected women.
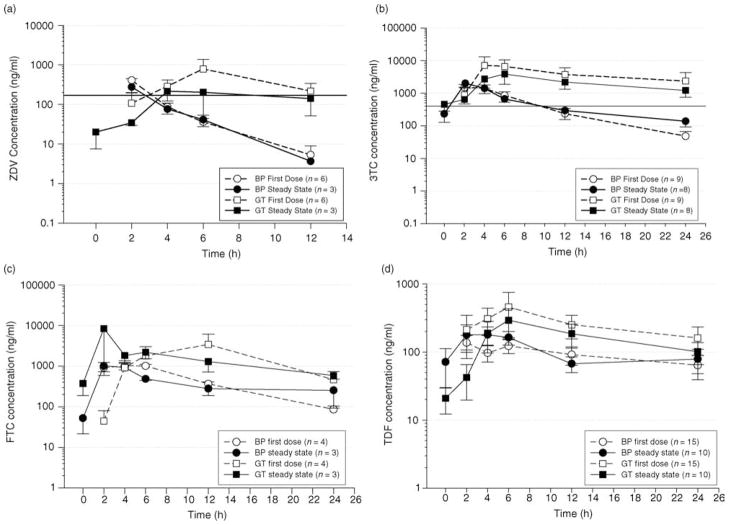
Method: Twenty-seven women initiating combination antiretroviral therapy underwent comprehensive blood plasma and cervicovaginal fluid sampling for drug concentrations during the first dose of antiretroviral therapy and at steady-state. Drug concentrations were measured by validated HPLC/UV or HPLC-MS/MS methods. Pharmacokinetic parameters were estimated for 11 drugs by non-compartmental analysis. Descriptive statistics and 95% confidence intervals were generated using Intercooled STATA Release 8.0 (Stata Corporation, College Station, Texas, USA).
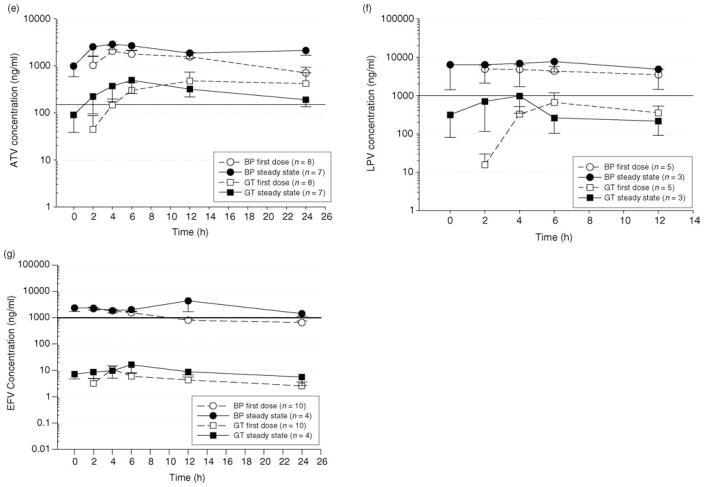
Results: For all antiretroviral drugs, genital tract concentrations were detected rapidly after the first dose. Drugs were stratified according to the genital tract concentrations achieved relative to blood plasma. Median rank order of highest to lowest genital tract concentrations relative to blood plasma at steady state were: lamivudine (concentrations achieved were 411% greater than blood plasma), emtricitabine (395%), zidovudine (235%) tenofovir (75%), ritonavir (26%), didanosine (21%), atazanavir (18%), lopinavir (8%), abacavir (8%), stavudine (5%), and efavirenz (0.4%).
Conclusions: This is the first study to comprehensively evaluate antiretroviral drug exposure in the female genital tract. These findings support the use of lamivudine, zidovudine, tenofovir and emtricitabine as excellent pre-exposure/post-exposure prophylaxis (PrEP/PEP) candidates. Atazanavir and lopinavir might be useful agents for these applications due to favorable therapeutic indices, despite lower genital tract concentrations. Agents such as stavudine, abacavir, and efavirenz that achieve genital tract exposures less than 10% of blood plasma are less attractive PrEP/PEP candidates.
Figures
Similar articles
-
Pharmacokinetic modelling of efavirenz, atazanavir, lamivudine and tenofovir in the female genital tract of HIV-infected pre-menopausal women.Clin Pharmacokinet. 2012 Dec;51(12):809-22. doi: 10.1007/s40262-012-0012-y. Clin Pharmacokinet. 2012. PMID: 23044523 Free PMC article. Clinical Trial.
-
Abacavir plasma pharmacokinetics in the absence and presence of atazanavir/ritonavir or lopinavir/ritonavir and vice versa in HIV-infected patients.Antivir Ther. 2007;12(5):825-30. Antivir Ther. 2007. PMID: 17713166 Clinical Trial.
-
Duration of first-line antiretroviral therapy with tenofovir and emtricitabine combined with atazanavir/ritonavir, efavirenz or lopinavir/ritonavir in the Italian ARCA cohort.J Antimicrob Chemother. 2013 Jan;68(1):200-5. doi: 10.1093/jac/dks339. Epub 2012 Aug 21. J Antimicrob Chemother. 2013. PMID: 22915463
-
Pharmacokinetics of antiretroviral drugs in anatomical sanctuary sites: the male and female genital tract.Antivir Ther. 2011;16(8):1149-67. doi: 10.3851/IMP1919. Antivir Ther. 2011. PMID: 22155899 Review.
-
Clinical pharmacokinetics and summary of efficacy and tolerability of atazanavir.Clin Pharmacokinet. 2005;44(10):1035-50. doi: 10.2165/00003088-200544100-00003. Clin Pharmacokinet. 2005. PMID: 16176117 Review.
Cited by
-
Antiretrovirals and HIV prevention: new insights, challenges, and new directions.Curr Opin HIV AIDS. 2012 Nov;7(6):495-7. doi: 10.1097/COH.0b013e328358e4d9. Curr Opin HIV AIDS. 2012. PMID: 23032735 Free PMC article. No abstract available.
-
What primary care providers need to know about preexposure prophylaxis for HIV prevention: a narrative review.Ann Intern Med. 2012 Oct 2;157(7):490-7. doi: 10.7326/0003-4819-157-7-201210020-00510. Ann Intern Med. 2012. PMID: 22821365 Free PMC article. Review.
-
Drug transporters in tissues and cells relevant to sexual transmission of HIV: Implications for drug delivery.J Control Release. 2015 Dec 10;219:681-696. doi: 10.1016/j.jconrel.2015.08.018. Epub 2015 Aug 13. J Control Release. 2015. PMID: 26278511 Free PMC article. Review.
-
Highly diverse anaerobe-predominant vaginal microbiota among HIV-infected pregnant women in Zambia.PLoS One. 2019 Oct 2;14(10):e0223128. doi: 10.1371/journal.pone.0223128. eCollection 2019. PLoS One. 2019. PMID: 31577818 Free PMC article.
-
Lopinavir/Ritonavir: a review of its use in the management of HIV-1 infection.Drugs. 2010 Oct 1;70(14):1885-915. doi: 10.2165/11204950-000000000-00000. Drugs. 2010. PMID: 20836579 Review.
References
-
- UNAIDS. UNAIDS Global Fact Sheet. 24–27/07/2005. THird IAS Conference on HIV Pathogenesis and Treatment; Rio de Janeiro.
-
- UNAIDS. UNAIDS women and AIDS fact sheet. 23/11/2004. UNAIDS Epidemic Update. Geneva: UNAIDS; 2004.
-
- Hosseinipour M, Cohen MS, Vernazza PL, Kashuba AD. Can antiretroviral therapy be used to prevent sexual transmission of human immunodeficiency virus type 1? Clin Infect Disease. 2002;34:1391–1395. - PubMed
-
- . Recommendations from the US Department of Health and Human Services (DHHS) Management of possible sexual, infection-drug-use, or other nonoccupational exposure to hiv, including considerations related to antiretroviral therapy. Jan 212005. [Accessed: 27 June 2007]. www.AIDSinfo.nih.gov.
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
