

Clinical Trial
doi: 10.1182/blood-2006-11-058933.
Epub 2007 Mar 16.
Gene therapy improves immune function in preadolescents with X-linked severe combined immunodeficiency
Affiliations
- PMID: 17369490
- PMCID: PMC1896128
- DOI: 10.1182/blood-2006-11-058933
Item in Clipboard
Clinical Trial
Gene therapy improves immune function in preadolescents with X-linked severe combined immunodeficiency
Blood.
.
Abstract
Retroviral gene therapy can restore immunity to infants with X-linked severe combined immunodeficiency (XSCID) caused by mutations in the IL2RG gene encoding the common gamma chain (gammac) of receptors for interleukins 2 (IL-2), -4, -7, -9, -15, and -21. We investigated the safety and efficacy of gene therapy as salvage treatment for older XSCID children with inadequate immune reconstitution despite prior bone marrow transplant from a parent. Subjects received retrovirus-transduced autologous peripherally mobilized CD34(+) hematopoietic cells. T-cell function significantly improved in the youngest subject (age 10 years), and multilineage retroviral marking occurred in all 3 children.
Figures
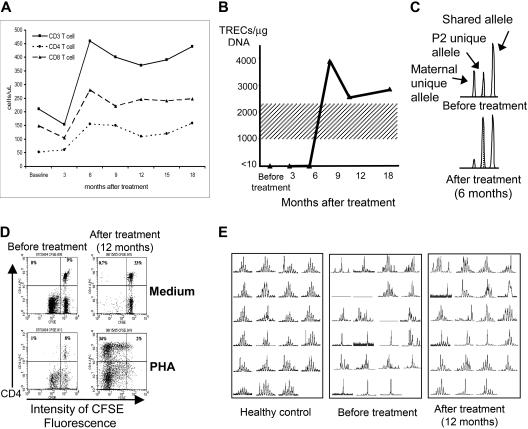
Improvements in immune function of patient P2 following gene therapy. (A) Increases in peripheral-blood CD4+, CD8+, and total CD3+ T-cell counts at 6 months after gene therapy. (B) TRECs, initially absent from peripheral-blood T cells, appearing at 9 months after gene therapy (normal adult range 1000-2200 TRECs/μg DNA, shading). (C) Shift in T-cell chimerism after gene therapy (area under PCR-amplified polymorphic allele peaks; Cofiler; Applied Biosystems, Foster City, CA), from before gene therapy (top set of peaks) where there is 51% maternal bone marrow donor (left peak) and 49% P2 host (stippled middle peak) to 6 months after gene therapy (bottom set of peaks) where the ratio is 13% donor versus 87% host. (D) CD4+ T-cell proliferation measured by decrease in fluorescence in response to PHA mitogen stimulation, absent before gene therapy (empty top left quadrant of the bottom left panel) but normal at 12 months after gene therapy (top left quadrant of the bottom right panel). P2 blood mononuclear leukocytes were labeled with the permanent cell-membrane–binding dye CFSE and cultured for 5 days in medium alone (control; top panels) or PHA (stimulus; bottom panels), then labeled with phycoerythrin-labeled anti-CD4 antibody. CD4+ T cells appear in the top half of each panel, and proliferation of the CD4+ T cells (dilution of CSFE fluorescence) is seen to occur only after gene therapy and only in response to PHA stimulation (bottom right panel). Not shown is that CD8+ T-cell response to PHA and both CD4+ and CD8+ responses to ConA, PWM, and Candida antigen increased similarly as measured by the CSFE assay. (E) Spectratyping of the Vβ TCR repertoire of CD3+ T cells from P2, demonstrating very restricted diversity before gene therapy (middle panel; total absence of representation of 3 Vβ families and almost monoclonal single-peak representation within 6 or 7 families) but increased diversity at 12 months after gene therapy (right panel; some representation in all the Vβ families, almost monoclonal single-peak representation only within 3 or 4 families, and clear improvement in multipeak polyclonality within 12 of the 23 families represented). A typical healthy control is shown in the left panel.
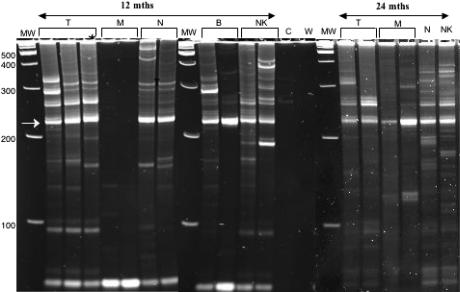
Polyclonality of vector inserts in blood leukocyte lineages of P2 at 12 and 24 months after gene therapy. Retroviral vector insertions are assessed by the LAM-PCR DNA amplification method; amplified bands of multiple sizes are then separated by gel electrophoresis, where the various bands correspond to different retroviral-genomic DNA junctions. Shown in this figure are 3 electrophoresis gels cropped to show the relevant adjacent lanes. The different gels are separated by a vertical white line. Gels A and B were run at the same time and amplifications of DNA from the various blood-cell lineages separated from a single blood sample from subject P2 were obtained at 12 months after gene therapy. Shown for each lineage are 2 to 3 independent amplifications for DNA from T (CD3+ lymphocytes), M (CD14+ monocytes), N (CD15+ neutrophils), B (CD19+ lymphocytes), and NK (CD56+CD3−) cells. Note that the unlabeled lane at the far right of gel B contained a sample of the same amplification of T as run in the left-most T lane in gel A to assure that gels A and B had run similarly. Also included in gel B are lanes containing the amplification of control (before gene therapy) blood cell DNA from P2 (C) and a water control (W). All gels contain a lan with molecular weight markers (MW), with the molecular weight indicated in base pairs (bp) at the left margin of gel A. The recurrent bright band at 227 bp (arrow at left) is derived from internal retroviral sequence. Polyclonality is demonstrated by bands of many sizes in T, B, and NK cells and neutrophils at 12 months after gene therapy. Gel C was run at a later time than gels A and B and contains amplifications of DNA from the various blood-cell lineages separated from a single blood sample from subject P2 obtained at 24 months after gene therapy. Shown in gel C are 2 independent LAM-PCR amplifications for the T and M lineages but only 1 amplification for N and NK lineages. Polyclonality of vector inserts is still observed at the 24-month time point.
Similar articles
-
Retroviral transduction of IL2RG into CD34(+) cells from X-linked severe combined immunodeficiency patients permits human T- and B-cell development in sheep chimeras.Blood. 2002 Jul 1;100(1):72-9. doi: 10.1182/blood.v100.1.72. Blood. 2002. PMID: 12070011
-
Comparison of five retrovirus vectors containing the human IL-2 receptor gamma chain gene for their ability to restore T and B lymphocytes in the X-linked severe combined immunodeficiency mouse model.Mol Ther. 2001 Apr;3(4):565-73. doi: 10.1006/mthe.2001.0292. Mol Ther. 2001. PMID: 11319919
-
Lentiviral Gene Therapy Combined with Low-Dose Busulfan in Infants with SCID-X1.N Engl J Med. 2019 Apr 18;380(16):1525-1534. doi: 10.1056/NEJMoa1815408. N Engl J Med. 2019. PMID: 30995372 Free PMC article. Clinical Trial.
-
Gene therapy studies in a canine model of X-linked severe combined immunodeficiency.Hum Gene Ther Clin Dev. 2015 Mar;26(1):50-6. doi: 10.1089/humc.2015.004. Epub 2015 Feb 24. Hum Gene Ther Clin Dev. 2015. PMID: 25603151 Free PMC article. Review.
-
Gene Therapy for X-Linked Severe Combined Immunodeficiency: Where Do We Stand?Hum Gene Ther. 2016 Feb;27(2):108-16. doi: 10.1089/hum.2015.137. Hum Gene Ther. 2016. PMID: 26790362 Free PMC article. Review.
Cited by
-
Gene therapy for PIDs: progress, pitfalls and prospects.Gene. 2013 Aug 10;525(2):174-81. doi: 10.1016/j.gene.2013.03.098. Epub 2013 Apr 6. Gene. 2013. PMID: 23566838 Free PMC article. Review.
-
Long-term clinical outcome of patients with severe combined immunodeficiency who received related donor bone marrow transplants without pretransplant chemotherapy or post-transplant GVHD prophylaxis.J Pediatr. 2009 Dec;155(6):834-840.e1. doi: 10.1016/j.jpeds.2009.07.049. Epub 2009 Oct 9. J Pediatr. 2009. PMID: 19818451 Free PMC article.
-
Creating higher titer lentivirus with caffeine.Hum Gene Ther. 2011 Jan;22(1):93-100. doi: 10.1089/hum.2010.068. Epub 2010 Dec 12. Hum Gene Ther. 2011. PMID: 20626321 Free PMC article.
-
Insulators to Improve the Safety of Retroviral Vectors for HIV Gene Therapy.Biomedicines. 2016 Mar;4(1):4. doi: 10.3390/biomedicines4010004. Epub 2016 Feb 2. Biomedicines. 2016. PMID: 28424756 Free PMC article.
-
Long-term outcome of non-ablative booster BMT in patients with SCID.Bone Marrow Transplant. 2013 Aug;48(8):1050-5. doi: 10.1038/bmt.2013.6. Epub 2013 Feb 11. Bone Marrow Transplant. 2013. PMID: 23396406 Free PMC article.
References
-
- Cavazzana-Calvo M, Hacein-Bey S, de Saint Basile G, et al. Gene therapy of human severe combined immunodeficiency (SCID)-X1 disease. Science. 2000;288:669–672. - PubMed
-
- Hacein-Bey-Abina S, Von Kalle C, Schmidt M, et al. LMO2-associated clonal T cell proliferation in two patients after gene therapy for SCID-X1. Science. 2003;302:415–419. - PubMed
-
- Gaspar HB, Parsley KL, Howe S, et al. Gene therapy of X-linked severe combined immunodeficiency by use of a pseudotyped gammaretroviral vector. Lancet. 2004;364:2181–2187. - PubMed
-
- Puck JM. X-linked severe combined immunodeficiency. In: Ochs H, Smith CIE, Puck JM, editors. Primary Immunodeficiency Diseases, a Molecular and Genetic Approach. 2nd ed. New York, NY: Oxford University Press; 2007. pp. 123–136.
-
- Buckley RH, Schiff SE, Schiff RI, et al. Hematopoietic stem cell transplantation for the treatment of severe combined immunodeficiency. New Engl J Med. 1999;340:508–516. - PubMed
