

Molecular pathology in the lungs of severe acute respiratory syndrome patients
- PMID: 17255322
- PMCID: PMC1851867
- DOI: 10.2353/ajpath.2007.060469
Molecular pathology in the lungs of severe acute respiratory syndrome patients
Abstract
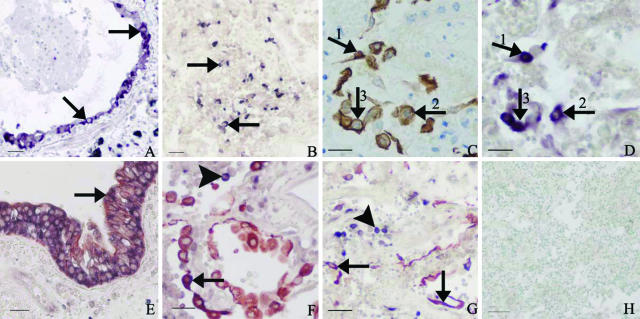
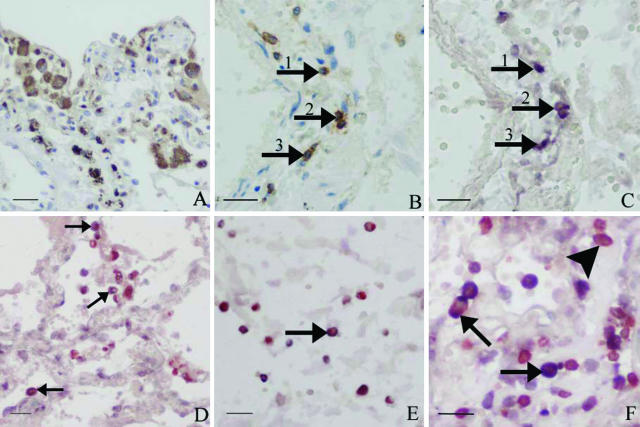
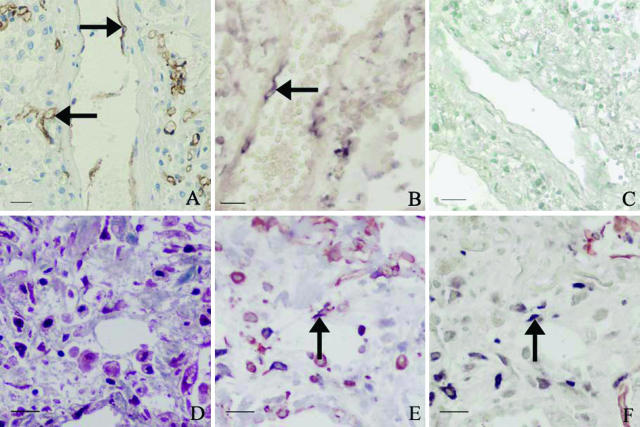
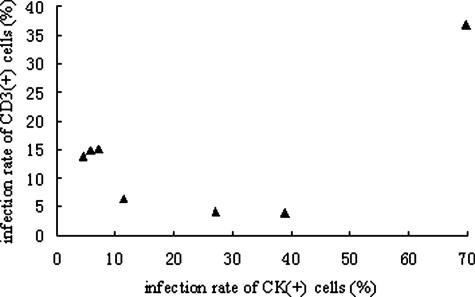
Severe acute respiratory syndrome (SARS) is a novel infectious disease with disastrous clinical consequences, in which the lungs are the major target organs. Previous studies have described the general pathology in the lungs of SARS patients and have identified some of the cell types infected by SARS coronavirus (SARS-CoV). However, at the time of this writing, there were no comprehensive reports of the cellular distribution of the virus in lung tissue. In this study, we have performed double labeling combining in situ hybridization with immunohistochemistry and alternating each of these techniques separately in consecutive sections to evaluate the viral distribution on various cell types in the lungs of seven patients affected with SARS. We found that SARS-CoV was present in bronchial epithelium, type I and II pneumocytes, T lymphocytes, and macrophages/monocytes. For pneumocytes, T lymphocytes, and macrophages, the infection rates were calculated. In addition, our present study is the first to demonstrate infection of endothelial cells and fibroblasts in SARS.
Figures
Similar articles
-
[Expression of SARS-CoV in various types of cells in lung tissues].Beijing Da Xue Xue Bao Yi Xue Ban. 2005 Oct 18;37(5):453-7. Beijing Da Xue Xue Bao Yi Xue Ban. 2005. PMID: 16224511 Chinese.
-
Immunohistochemical, in situ hybridization, and ultrastructural localization of SARS-associated coronavirus in lung of a fatal case of severe acute respiratory syndrome in Taiwan.Hum Pathol. 2005 Mar;36(3):303-9. doi: 10.1016/j.humpath.2004.11.006. Hum Pathol. 2005. PMID: 15791576 Free PMC article.
-
Detection of severe acute respiratory syndrome-associated coronavirus in pneumocytes of the lung.Am J Clin Pathol. 2004 Apr;121(4):574-80. doi: 10.1309/C0ED-U0RA-QBTX-BHCE. Am J Clin Pathol. 2004. PMID: 15080310 Free PMC article.
-
SARS-CoV replication and pathogenesis in an in vitro model of the human conducting airway epithelium.Virus Res. 2008 Apr;133(1):33-44. doi: 10.1016/j.virusres.2007.03.013. Epub 2007 Apr 23. Virus Res. 2008. PMID: 17451829 Free PMC article. Review.
-
Pathogenetic mechanisms of severe acute respiratory syndrome.Virus Res. 2008 Apr;133(1):4-12. doi: 10.1016/j.virusres.2007.01.022. Epub 2007 Sep 7. Virus Res. 2008. PMID: 17825937 Free PMC article. Review.
Cited by
-
Thrombosis in Coronavirus disease 2019 (COVID-19) through the prism of Virchow's triad.Clin Rheumatol. 2020 Sep;39(9):2529-2543. doi: 10.1007/s10067-020-05275-1. Epub 2020 Jul 11. Clin Rheumatol. 2020. PMID: 32654082 Free PMC article. Review.
-
COVID-19-driven endothelial damage: complement, HIF-1, and ABL2 are potential pathways of damage and targets for cure.Ann Hematol. 2020 Aug;99(8):1701-1707. doi: 10.1007/s00277-020-04138-8. Epub 2020 Jun 24. Ann Hematol. 2020. PMID: 32583086 Free PMC article. Review.
-
SARS-CoV replicates in primary human alveolar type II cell cultures but not in type I-like cells.Virology. 2008 Mar 1;372(1):127-35. doi: 10.1016/j.virol.2007.09.045. Epub 2007 Nov 26. Virology. 2008. PMID: 18022664 Free PMC article.
-
Autocrine interferon priming in macrophages but not dendritic cells results in enhanced cytokine and chemokine production after coronavirus infection.mBio. 2010 Oct 19;1(4):e00219-10. doi: 10.1128/mBio.00219-10. mBio. 2010. PMID: 20978536 Free PMC article.
-
Inhibition of severe acute respiratory syndrome coronavirus replication in a lethal SARS-CoV BALB/c mouse model by stinging nettle lectin, Urtica dioica agglutinin.Antiviral Res. 2011 Apr;90(1):22-32. doi: 10.1016/j.antiviral.2011.02.003. Epub 2011 Feb 19. Antiviral Res. 2011. PMID: 21338626 Free PMC article.
References
-
- Tsang KW, Ho PL, Ooi GC, Yee WK, Wang T, Chan-Yeung M, Lam WK, Seto WH, Yam LY, Cheung TM, Wong PC, Lam B, Ip MS, Chan J, Yuen KY, Lai KN. A cluster of cases of severe acute respiratory syndrome in Hong Kong. N Engl J Med. 2003;348:1977–1985. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Miscellaneous
