

Neuroimmunophilin ligands protect cavernous nerves after crush injury in the rat: new experimental paradigms
- PMID: 17145129
- PMCID: PMC2682459
- DOI: 10.1016/j.eururo.2006.11.026
Neuroimmunophilin ligands protect cavernous nerves after crush injury in the rat: new experimental paradigms
Abstract
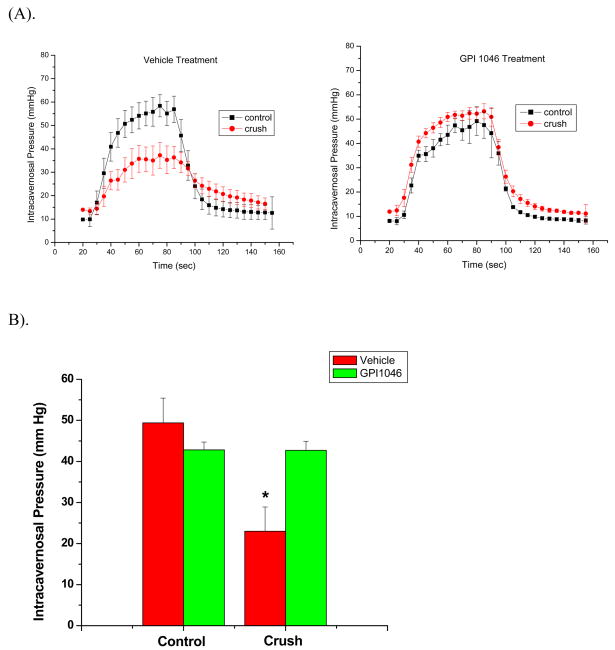
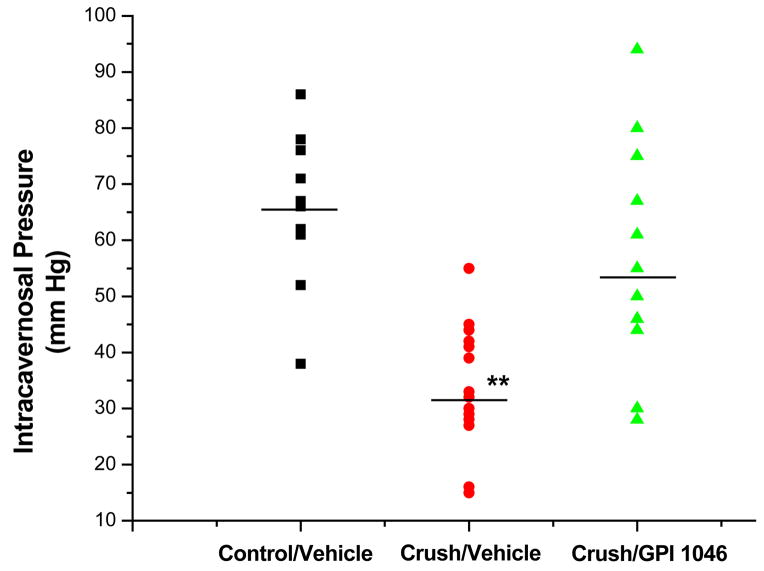
Objectives: We investigated the effects of the orally bioavailable non-immunosuppressive immunophilin ligand GPI 1046 (GPI) on erectile function and cavernous nerve (CN) histology following unilateral or bilateral crush injury (UCI, BCI, respectively) of the CNs.
Methods: Adult male Sprague-Dawley rats were administered GPI 15 mg/kg intraperitoneally (ip) or 30 mg/kg orally (po), FK506 1 mg/kg, ip, or vehicle controls for each route of administration just prior to UCI or BCI and daily up to 7 d following injury. At day 1 or 7 of treatment, erectile function induced by CN electrical stimulation was measured, and electron microscopic analysis of the injured CN was performed.
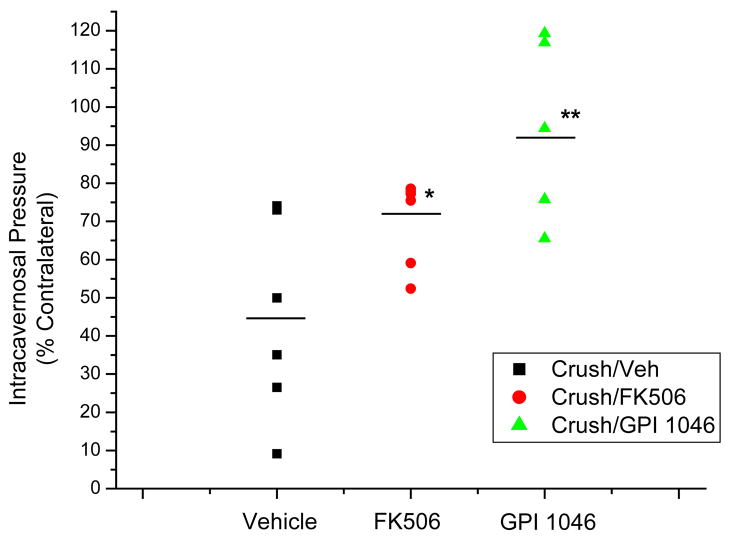
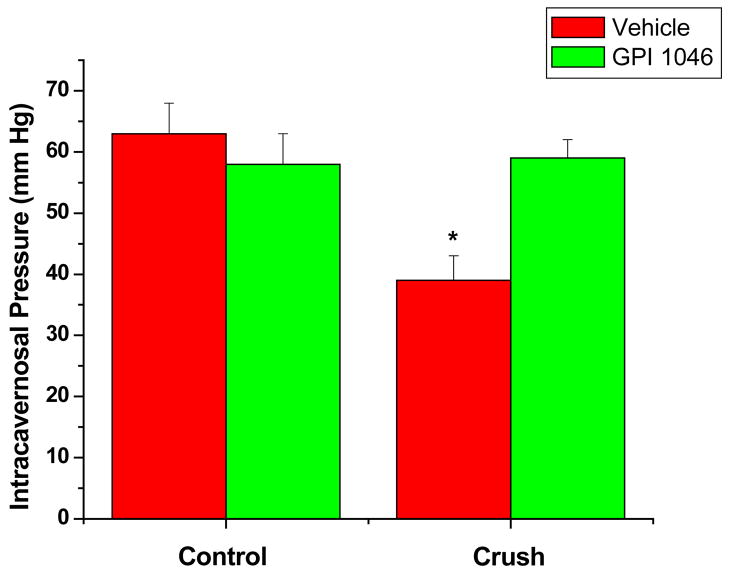
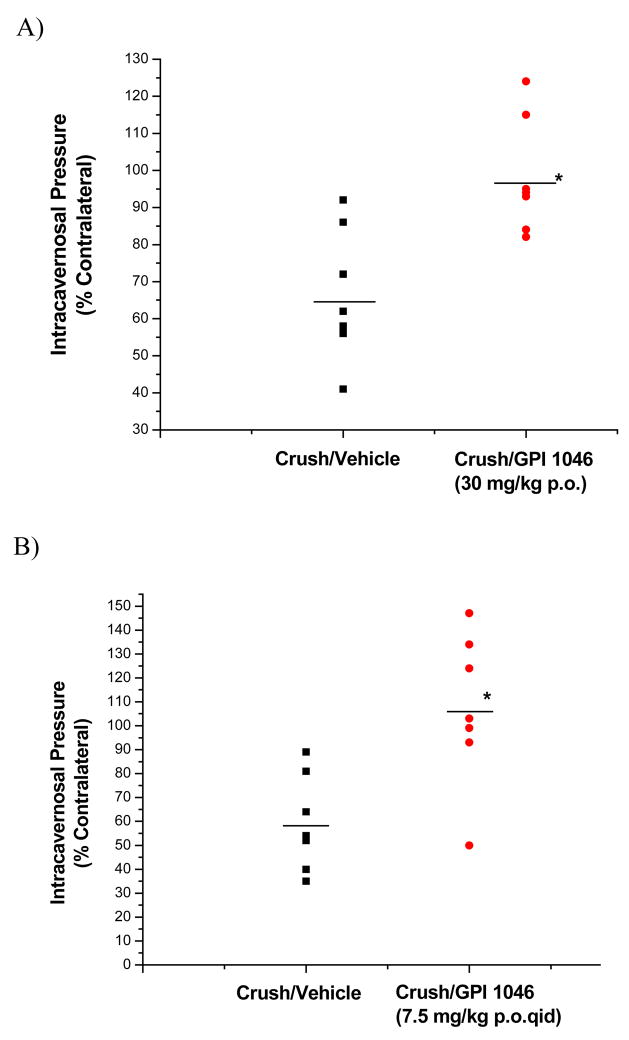
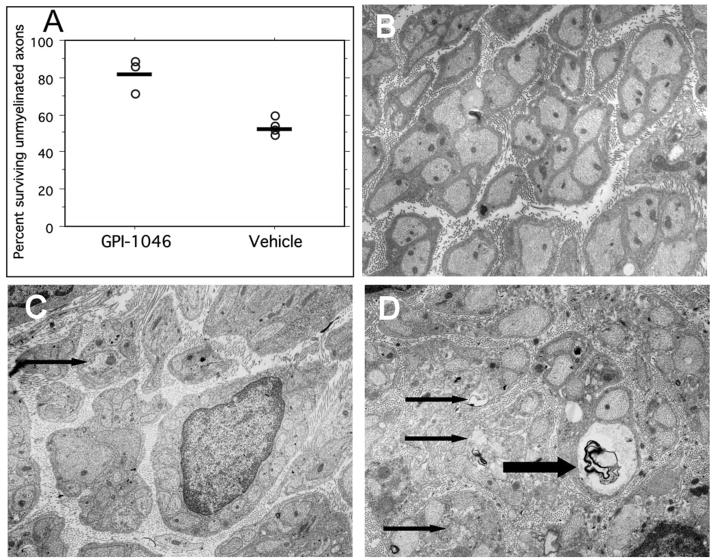
Results: Intraperitoneal administration of GPI to rats with injured CN protected erectile function, in a fashion similar to the prototypic immunophilin ligand FK506, compared with vehicle-treated animals (93%+/-9% vs. 70%+/-5% vs. 45%+/-1%, p<0.01, respectively). Oral administration of GPI elicited the same level of significant protection from CN injury. GPI administered po at 30 mg/kg/d, dosing either once daily or four times daily with 7.5 mg/kg, provided nearly complete protection of erectile function. In a more severe BCI model, po administration of GPI maintained erectile function at 24 h after CN injury. Ultrastructural analysis of injured CNs indicated that GPI administered at the time of CN injury prevents degeneration of about 83% of the unmyelinated axons at 7 d after CN injury.
Conclusions: The orally administered immunophilin ligand GPI neuroprotects CNs and maintains erectile function in rats under various conditions of CN crush injury.
Figures
Comment in
-
Neuroimmunophilin ligands protect cavernous nerves after crush injury in the rat: new experimental paradigms.Eur Urol. 2007 Jun;51(6):1488-9. doi: 10.1016/j.eururo.2007.01.043. Epub 2007 Jan 16. Eur Urol. 2007. PMID: 17275990 No abstract available.
Similar articles
-
Neuroimmunophilin ligands protect cavernous nerves after crush injury in the rat: new experimental paradigms.Eur Urol. 2007 Jun;51(6):1488-9. doi: 10.1016/j.eururo.2007.01.043. Epub 2007 Jan 16. Eur Urol. 2007. PMID: 17275990 No abstract available.
-
Immunophilin ligands promote penile neurogenesis and erection recovery after cavernous nerve injury.J Urol. 2004 Jan;171(1):495-500. doi: 10.1097/01.ju.0000089775.88825.ec. J Urol. 2004. PMID: 14665962
-
FK506 and sildenafil promote erectile function recovery after cavernous nerve injury through antioxidative mechanisms.J Sex Med. 2007 Jul;4(4 Pt 1):908-16. doi: 10.1111/j.1743-6109.2007.00519.x. J Sex Med. 2007. PMID: 17627738
-
Role of immunophilins in recovery of erectile function after cavernous nerve injury.J Sex Med. 2009 Mar;6 Suppl 3(Suppl 3):340-6. doi: 10.1111/j.1743-6109.2008.01193.x. J Sex Med. 2009. PMID: 19267858 Free PMC article. Review.
-
Bilateral Cavernous Nerve Crush Injury in the Rat Model: A Comparative Review of Pharmacologic Interventions.Sex Med Rev. 2018 Apr;6(2):234-241. doi: 10.1016/j.sxmr.2017.07.007. Epub 2017 Aug 18. Sex Med Rev. 2018. PMID: 28827037 Review.
Cited by
-
A review of regenerative therapies as penile rehabilitation in men following primary prostate cancer treatment: Evidence for erectile restoration and cavernous nerve regeneration.Asian J Urol. 2022 Jul;9(3):287-293. doi: 10.1016/j.ajur.2021.11.005. Epub 2021 Nov 20. Asian J Urol. 2022. PMID: 36035357 Free PMC article. Review.
-
Penile Rehabilitation and Treatment Options for Erectile Dysfunction Following Radical Prostatectomy and Radiotherapy: A Systematic Review.Front Surg. 2021 Mar 2;8:636974. doi: 10.3389/fsurg.2021.636974. eCollection 2021. Front Surg. 2021. PMID: 33738297 Free PMC article.
-
GPI-1046 protects dorsal root ganglia from gp120-induced axonal injury by modulating store-operated calcium entry.J Peripher Nerv Syst. 2009 Mar;14(1):27-35. doi: 10.1111/j.1529-8027.2009.00203.x. J Peripher Nerv Syst. 2009. PMID: 19335537 Free PMC article.
-
Combined effects of brain-derived neurotrophic factor immobilized poly-lactic-co-glycolic acid membrane with human adipose-derived stem cells and basic fibroblast growth factor hydrogel on recovery of erectile dysfunction.Tissue Eng Part A. 2014 Sep;20(17-18):2446-54. doi: 10.1089/ten.tea.2013.0495. Epub 2014 May 20. Tissue Eng Part A. 2014. PMID: 24673637 Free PMC article.
-
Dipyridamole reduces penile apoptosis in a rat model of post-prostatectomy erectile dysfunction.Int Braz J Urol. 2017 Sep-Oct;43(5):966-973. doi: 10.1590/S1677-5538.IBJU.2017.0023. Int Braz J Urol. 2017. PMID: 28727374 Free PMC article.
References
-
- Burnett AL. Erectile dysfunction following radical prostatectomy. JAMA. 2005;293:2648–53. - PubMed
-
- Montorsi F, McCullough A. Efficacy of sildenafil citrate in men with erectile dysfunction following radical prostatectomy: a systematic review of clinical data. J Sex Med. 2005;2:658–67. - PubMed
-
- Carrier S, Zvara P, Nunes L, et al. Regeneration of nitric oxide synthase-containing nerves after cavernous nerve neurotomy in the rat. J Urol. 1995;153:1722–7. - PubMed
-
- Bochinski D, Lin GT, Nunes L, et al. The effect of neural embryonic stem cell therapy in a rat model of cavernosal nerve injury. BJU Int. 2004;94:904–9. - PubMed
-
- Chen KC, Minor TX, Rahman NU, et al. The additive erectile recovery effect of brain-derived neurotrophic factor combined with vascular endothelial growth factor in a rat model of neurogenic impotence. BJU Int. 2005;95:1077–80. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
