

Procalcitonin, lipopolysaccharide-binding protein, interleukin-6 and C-reactive protein in community-acquired infections and sepsis: a prospective study
- PMID: 16569262
- PMCID: PMC1550885
- DOI: 10.1186/cc4866
Procalcitonin, lipopolysaccharide-binding protein, interleukin-6 and C-reactive protein in community-acquired infections and sepsis: a prospective study
Abstract
Introduction: Clinicians are in need of better diagnostic markers in diagnosing infections and sepsis. We studied the ability of procalcitonin, lipopolysaccharide-binding protein, IL-6 and C-reactive protein to identify patients with infection and sepsis.
Methods: Plasma and serum samples were obtained on admission from patients with suspected community-acquired infections and sepsis. Procalcitonin was measured with a time-resolved amplified cryptate emission technology assay. Lipopolysaccharide-binding protein and IL-6 were measured with a chemiluminescent immunometric assay.
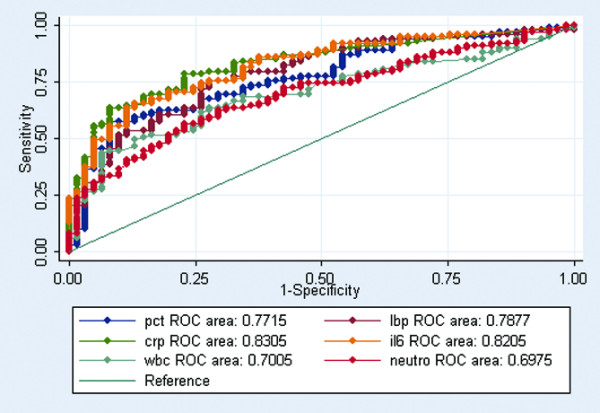
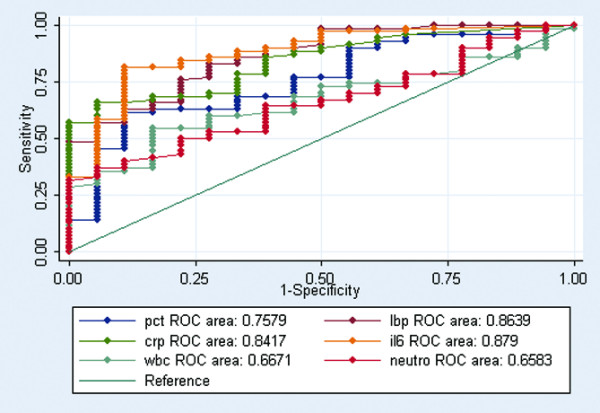
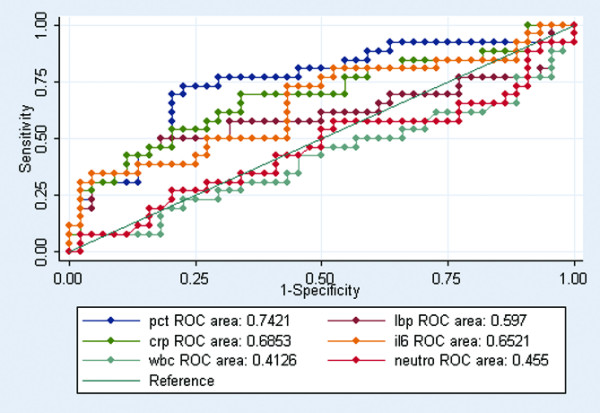
Results: Of 194 included patients, 106 had either infection without systemic inflammatory response syndrome or sepsis. Infected patients had significantly elevated levels of procalcitonin, lipopolysaccharide-binding protein, C-reactive protein and IL-6 compared with noninfected patients (P < 0.001). In a receiver-operating characteristic curve analysis, C-reactive protein and IL-6 performed best in distinguishing between noninfected and infected patients, with an area under the curve larger than 0.82 (P < 0.05). IL-6, lipopolysaccharide-binding protein and C-reactive protein performed best in distinguishing between systemic inflammatory response syndrome and sepsis, with an area under the curve larger than 0.84 (P < 0.01). Procalcitonin performed best in distinguishing between sepsis and severe sepsis, with an area under the curve of 0.74 (P < 0.01).
Conclusion: C-reactive protein, IL-6 and lipopolysaccharide-binding protein appear to be superior to procalcitonin as diagnostic markers for infection and sepsis in patients admitted to a Department of Internal Medicine. Procalcitonin appears to be superior as a severity marker.
Figures
Similar articles
-
A comparison of high-mobility group-box 1 protein, lipopolysaccharide-binding protein and procalcitonin in severe community-acquired infections and bacteraemia: a prospective study.Crit Care. 2007;11(4):R76. doi: 10.1186/cc5967. Crit Care. 2007. PMID: 17625012 Free PMC article.
-
Lipopolysaccharide-binding protein in critically ill neonates and children with suspected infection: comparison with procalcitonin, interleukin-6, and C-reactive protein.Intensive Care Med. 2004 Jul;30(7):1454-60. doi: 10.1007/s00134-004-2307-4. Epub 2004 May 4. Intensive Care Med. 2004. PMID: 15127192
-
Sepsis biomarkers in neutropaenic systemic inflammatory response syndrome patients on standard care wards.Eur J Clin Invest. 2015 Aug;45(8):815-23. doi: 10.1111/eci.12476. Eur J Clin Invest. 2015. PMID: 26046926
-
[Sepsismarker--what is useful?].Dtsch Med Wochenschr. 2008 Nov;133(48):2512-5. doi: 10.1055/s-0028-1100949. Epub 2008 Nov 19. Dtsch Med Wochenschr. 2008. PMID: 19021084 Review. German. No abstract available.
-
Procalcitonin as a diagnostic test for sepsis in critically ill adults and after surgery or trauma: a systematic review and meta-analysis.Crit Care Med. 2006 Jul;34(7):1996-2003. doi: 10.1097/01.CCM.0000226413.54364.36. Crit Care Med. 2006. PMID: 16715031 Review.
Cited by
-
Wave-shaped microfluidic chip assisted point-of-care testing for accurate and rapid diagnosis of infections.Mil Med Res. 2022 Feb 11;9(1):8. doi: 10.1186/s40779-022-00368-1. Mil Med Res. 2022. PMID: 35144683 Free PMC article.
-
Evaluation of urinary tissue inhibitor of metalloproteinase-2 in acute kidney injury: a prospective observational study.Crit Care. 2014 Dec 19;18(6):716. doi: 10.1186/s13054-014-0716-5. Crit Care. 2014. PMID: 25524453 Free PMC article.
-
Effect of Continuous Digital Hypothermia on Lamellar Inflammatory Signaling When Applied at a Clinically-Relevant Timepoint in the Oligofructose Laminitis Model.J Vet Intern Med. 2018 Jan;32(1):450-458. doi: 10.1111/jvim.15027. Epub 2017 Dec 27. J Vet Intern Med. 2018. PMID: 29282770 Free PMC article. Clinical Trial.
-
Clinical potential of C-reactive protein and procalcitonin serum concentrations to guide differential diagnosis and clinical management of pneumococcal and Legionella pneumonia.J Clin Microbiol. 2010 May;48(5):1915-7. doi: 10.1128/JCM.01348-09. Epub 2010 Mar 10. J Clin Microbiol. 2010. PMID: 20220163 Free PMC article.
-
Diagnostic effectiveness of soluble triggering receptor expressed on myeloid cells-1 in sepsis, severe sepsis and septic shock.Arch Med Sci. 2019 May;15(3):713-721. doi: 10.5114/aoms.2018.73090. Epub 2019 Feb 25. Arch Med Sci. 2019. PMID: 31110539 Free PMC article.
References
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
