

Morphological characteristics of coronary atherosclerosis in diabetes mellitus
- PMID: 16498517
- PMCID: PMC2780829
- DOI: 10.1016/s0828-282x(06)70991-6
Morphological characteristics of coronary atherosclerosis in diabetes mellitus
Abstract
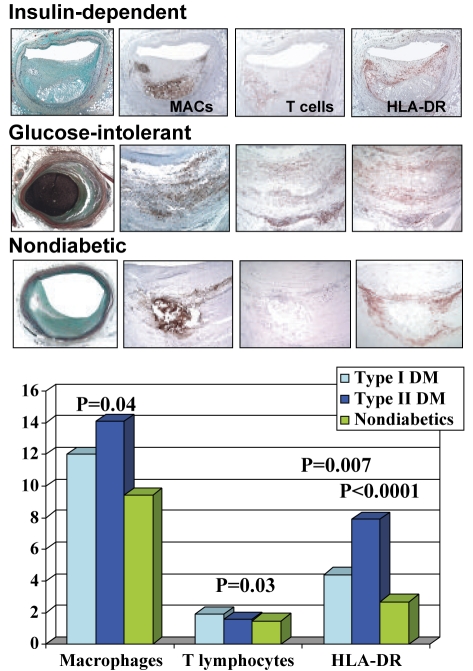
The incidence of diabetes is increasing in the general population because of increasing obesity, and is likely to result in a higher incidence of coronary artery disease. It was recently reported that diabetics (types I and II) dying suddenly from coronary artery disease have greater macrophage and T lymphocyte infiltration in atherosclerotic plaques, as well as larger necrotic cores compared with nondiabetics. The inflammatory cell infiltrates showed human leukocyte antigen-DR expression, which was greater in diabetics. The receptors for advanced glycosylation end-products expression, demonstrated by immunohistochemistry, was greater in diabetics than in nondiabetics in macrophages, smooth muscle cells and endothelial cells, and was associated with apoptosis of macrophages and smooth muscle cells, but not of endothelial cells. There is also a higher incidence of healed plaque ruptures and healed myocardial infarct in type II diabetics. Plaque burden is higher in diabetics than in nondiabetics; however, distal plaque burden was only significantly different in type II diabetics compared with nondiabetics. There was greater positive remodelling in diabetic coronary arteries than in nondiabetic ones, which correlated with the per cent necrotic core. Further studies are needed to better understand the mechanisms that govern greater inflammation and plaque burden in diabetics.
L’incidence du diabète est en hausse dans la population générale à cause de l’augmentation des cas d’obésité, et elle risque fort d’entraîner à sa suite une forte incidence de la maladie coronarienne. On a récemment signalé que comparativement aux non-diabétiques, les diabétiques (de type I et de type II) décédés subitement de coronaropathie présentaient une infiltration plus importante des macrophages et des lymphocytes T dans leurs plaques d’athérome et des noyaux nécrotiques plus volumineux. Les infiltrats cellulaires inflammatoires ont révélé une expression plus marquée de l’antigène HLA-DR chez les diabétiques que chez les non-diabétiques. Les récepteurs de l’expression des produits terminaux de la glycosylation avancée observés en immunohistochimie étaient plus présents dans les macrophages, les cellules des muscles lisses et les cellules endothéliales des diabétiques que des non-diabétiques et étaient associés à l’apoptose des macrophages et des cellules des muscles lisses, mais non des cellules endothéliales. On note en outre une incidence plus forte de plaques rompues cicatrisées et d’infarctus du myocarde cicatrisés chez les diabétiques de type II. Le rôle de la plaque est plus important chez les diabétiques que chez les non-diabétiques. Par contre, la différence ne s’est révélée significative qu’entre les diabétiques de type II et les non-diabétiques. On a noté un remodelage positif plus marqué au niveau des coronaires des diabétiques, phénomène qui était en corrélation avec le pourcentage de noyaux nécrotiques. Il faudra poursuivre la recherche pour mieux comprendre les mécanismes qui sont à l’origine de l’inflammation plus marquée et du rôle plus prépondérant de la plaque chez les diabétiques.
Figures
Similar articles
-
Morphologic findings of coronary atherosclerotic plaques in diabetics: a postmortem study.Arterioscler Thromb Vasc Biol. 2004 Jul;24(7):1266-71. doi: 10.1161/01.ATV.0000131783.74034.97. Epub 2004 May 13. Arterioscler Thromb Vasc Biol. 2004. PMID: 15142859
-
Pathology of Human Coronary and Carotid Artery Atherosclerosis and Vascular Calcification in Diabetes Mellitus.Arterioscler Thromb Vasc Biol. 2017 Feb;37(2):191-204. doi: 10.1161/ATVBAHA.116.306256. Epub 2016 Dec 1. Arterioscler Thromb Vasc Biol. 2017. PMID: 27908890 Free PMC article. Review.
-
Healed plaque ruptures and sudden coronary death: evidence that subclinical rupture has a role in plaque progression.Circulation. 2001 Feb 20;103(7):934-40. doi: 10.1161/01.cir.103.7.934. Circulation. 2001. PMID: 11181466
-
Sudden coronary death caused by pathologic intimal thickening without atheromatous plaque formation.Cardiovasc Pathol. 2011 Jan-Feb;20(1):51-7. doi: 10.1016/j.carpath.2009.08.004. Epub 2009 Nov 12. Cardiovasc Pathol. 2011. PMID: 19913444
-
Update on acute coronary syndromes: the pathologists' view.Eur Heart J. 2013 Mar;34(10):719-28. doi: 10.1093/eurheartj/ehs411. Epub 2012 Dec 13. Eur Heart J. 2013. PMID: 23242196 Review.
Cited by
-
Role of NFAT in the Progression of Diabetic Atherosclerosis.Front Cardiovasc Med. 2021 Mar 11;8:635172. doi: 10.3389/fcvm.2021.635172. eCollection 2021. Front Cardiovasc Med. 2021. PMID: 33791348 Free PMC article. Review.
-
Recent novel approaches to limit oxidative stress and inflammation in diabetic complications.Clin Transl Immunology. 2018 Apr 18;7(4):e1016. doi: 10.1002/cti2.1016. eCollection 2018. Clin Transl Immunology. 2018. PMID: 29713471 Free PMC article. Review.
-
Metformin improved oxidized low-density lipoprotein-impaired mitochondrial function and increased glucose uptake involving Akt-AS160 pathway in raw264.7 macrophages.Chin Med J (Engl). 2019 Jul 20;132(14):1713-1722. doi: 10.1097/CM9.0000000000000333. Chin Med J (Engl). 2019. PMID: 31268904 Free PMC article.
-
Disruption of COMMD1 accelerates diabetic atherosclerosis by promoting glycolysis.Diab Vasc Dis Res. 2023 Jan-Feb;20(1):14791641231159009. doi: 10.1177/14791641231159009. Diab Vasc Dis Res. 2023. PMID: 36803109 Free PMC article.
-
Transcriptional profiles associated with coronary artery disease in type 2 diabetes mellitus.Front Endocrinol (Lausanne). 2024 Apr 19;15:1323168. doi: 10.3389/fendo.2024.1323168. eCollection 2024. Front Endocrinol (Lausanne). 2024. PMID: 38706700 Free PMC article.
References
-
- Amos AF, McCarty DJ, Zimmet P. The rising global burden of diabetes and its complications: Estimates and projections to the year 2010. Diabet Med. 1997;14(Suppl 5):S1–85. - PubMed
-
- Mokdad AH, Bowman BA, Ford ES, Vinicor F, Marks JS, Koplan JP. The continuing epidemics of obesity and diabetes in the United States. JAMA. 2001;286:1195–200. - PubMed
-
- Silva JA, Escobar A, Collins TJ, Ramee SR, White CJ. Unstable angina. A comparison of angioscopic findings between diabetic and nondiabetic patients. Circulation. 1995;92:1731–6. - PubMed
-
- Schurgin S, Rich S, Mazzone T. Increased prevalence of significant coronary artery calcification in patients with diabetes. Diabetes Care. 2001;24:335–8. - PubMed
-
- Kornowski R, Mintz GS, Lansky AJ, et al. Paradoxic decreases in atherosclerotic plaque mass in insulin-treated diabetic patients. Am J Cardiol. 1998;81:1298–304. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
