

Bilateral cochlear implants in children: localization acuity measured with minimum audible angle
- PMID: 16446564
- PMCID: PMC2651156
- DOI: 10.1097/01.aud.0000194515.28023.4b
Bilateral cochlear implants in children: localization acuity measured with minimum audible angle
Abstract
Objective: To evaluate sound localization acuity in a group of children who received bilateral (BI) cochlear implants in sequential procedures and to determine the extent to which BI auditory experience affects sound localization acuity. In addition, to investigate the extent to which a hearing aid in the nonimplanted ear can also provide benefits on this task.
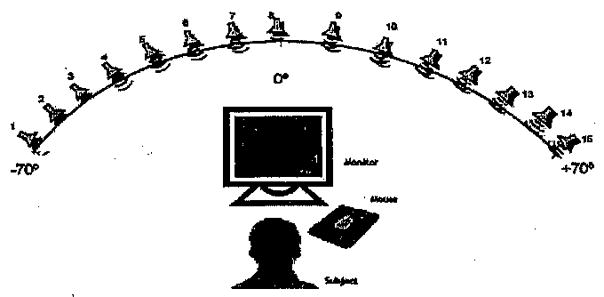
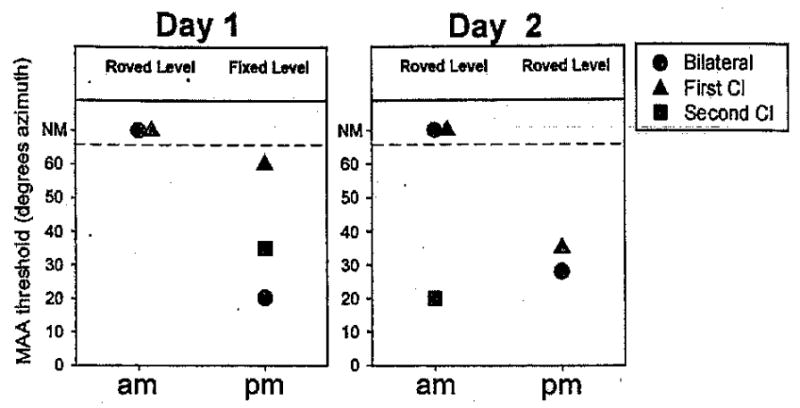
Design: Two groups of children participated, 13 with BI cochlear implants (cochlear implant + cochlear implant), ranging in age from 3 to 16 yrs, and six with a hearing aid in the nonimplanted ear (cochlear implant + hearing aid), ages 4 to 14 yrs. Testing was conducted in large sound-treated booths with loudspeakers positioned on a horizontal arc with a radius of 1.5 m. Stimuli were spondaic words recorded with a male voice. Stimulus levels typically averaged 60 dB SPL and were randomly roved between 56 and 64 dB SPL (+/-4 dB rove); in a few instances, levels were held fixed (60 dB SPL). Testing was conducted by using a "listening game" platform via computerized interactive software, and the ability of each child to discriminate sounds presented to the right or left was measured for loudspeakers subtending various angular separations. Minimum audible angle thresholds were measured in the BI (cochlear implant + cochlear implant or cochlear implant + hearing aid) listening mode and under monaural conditions.
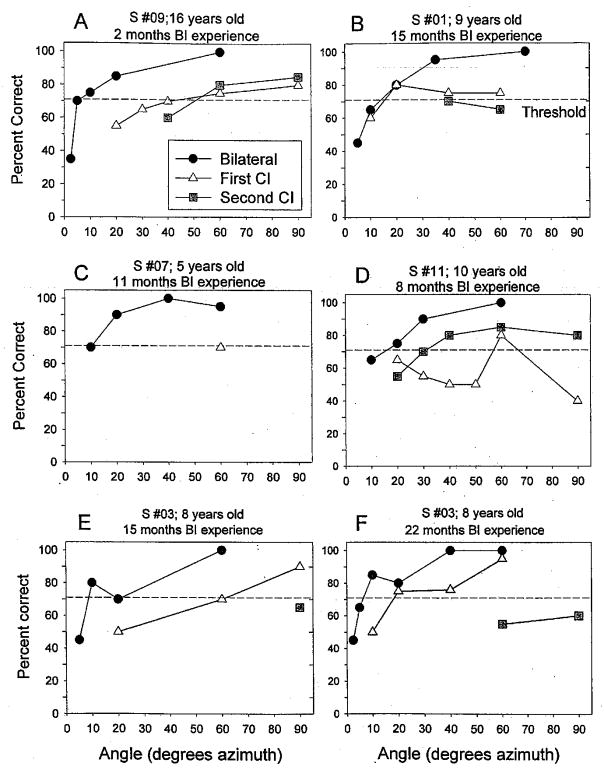
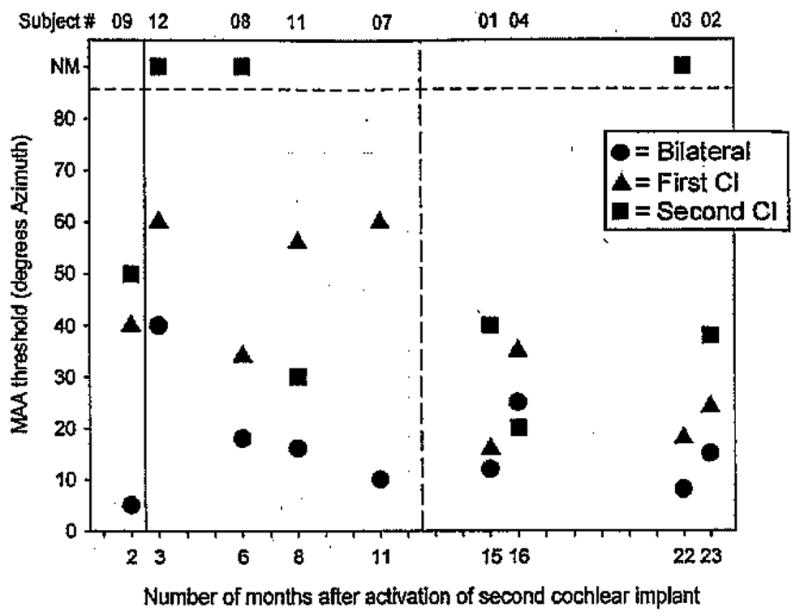
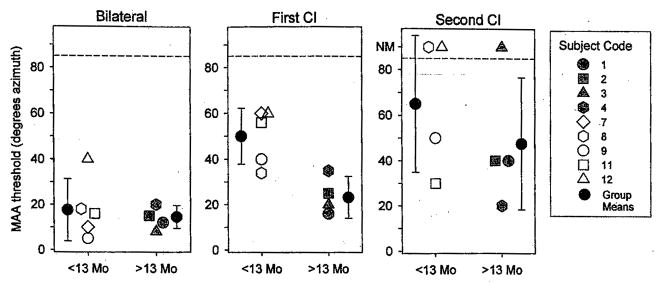
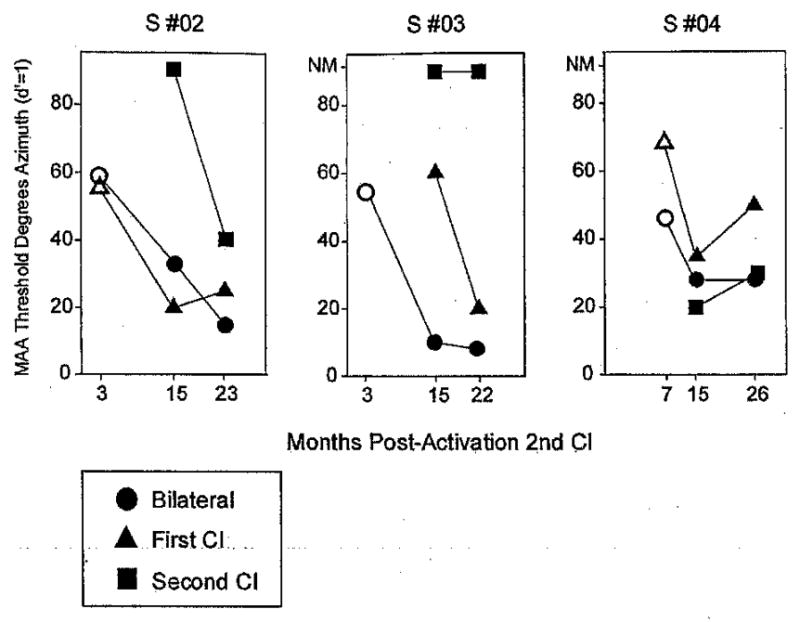
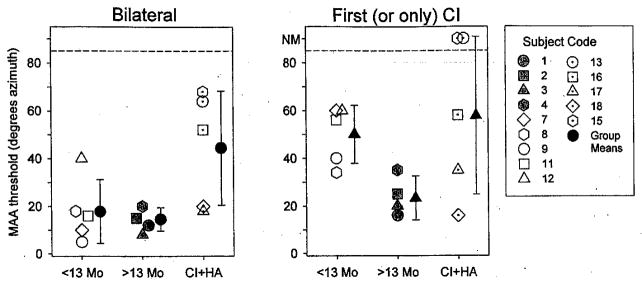
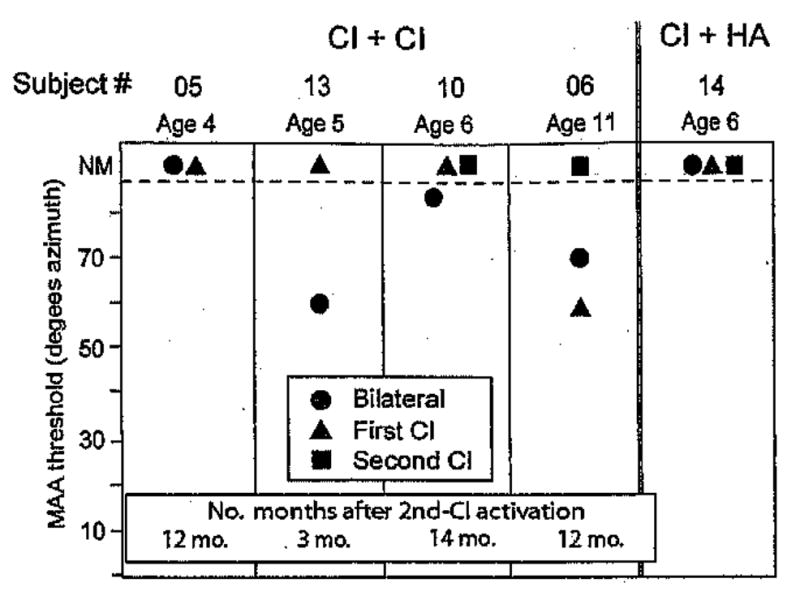
Results: Approximately 70% (9/13) of children in the cochlear implant + cochlear implant group discriminated left/right for source separations of <or=20 degrees , and, of those, 77% (7/9) performed better when listening bilaterally than with either cochlear implant alone. Several children were also able to perform the task when using a single cochlear implant, under some conditions. Minimum audible angle thresholds were better in the first cochlear implant than the second cochlear implant listening mode for nearly all (8/9) subjects. Repeated testing of a few individual subjects over a 2-yr period suggests that robust improvements in performance occurred with increased auditory experience. Children who wore hearing aids in the nonimplanted ear were at times also able to perform the task. Average group performance was worse than that of the children with BI cochlear implants when both ears were activated (cochlear implant + hearing aid versus cochlear implant + cochlear implant) but not significantly different when listening with a single cochlear implant.
Conclusions: Children with sequential BI cochlear implants represent a unique population of individuals who have undergone variable amounts of auditory deprivation in each ear. Our findings suggest that many but not all of these children perform better on measures of localization acuity with two cochlear implants compared with one and are better at the task than children using the cochlear implant + hearing aid. These results must be interpreted with caution, because benefits on other tasks as well as the long-term benefits of BI cochlear implants are yet to be fully understood. The factors that might contribute to such benefits must be carefully evaluated in large populations of children using a variety of measures.
Figures
Similar articles
-
Spatial acuity in 2-to-3-year-old children with normal acoustic hearing, unilateral cochlear implants, and bilateral cochlear implants.Ear Hear. 2012 Sep-Oct;33(5):561-72. doi: 10.1097/AUD.0b013e31824c7801. Ear Hear. 2012. PMID: 22517185 Free PMC article.
-
Sound localization skills in children who use bilateral cochlear implants and in children with normal acoustic hearing.Ear Hear. 2010 Oct;31(5):645-56. doi: 10.1097/AUD.0b013e3181e50a1d. Ear Hear. 2010. PMID: 20592615 Free PMC article.
-
Recognition and localization of speech by adult cochlear implant recipients wearing a digital hearing aid in the nonimplanted ear (bimodal hearing).J Am Acad Audiol. 2009 Jun;20(6):353-73. doi: 10.3766/jaaa.20.6.4. J Am Acad Audiol. 2009. PMID: 19594084 Free PMC article.
-
[Cochlear implant in children: rational, indications and cost/efficacy].Minerva Pediatr. 2013 Jun;65(3):325-39. Minerva Pediatr. 2013. PMID: 23685383 Review. Italian.
-
Restoring hearing symmetry with two cochlear implants or one cochlear implant and a contralateral hearing aid.J Rehabil Res Dev. 2008;45(5):749-67. doi: 10.1682/jrrd.2007.08.0120. J Rehabil Res Dev. 2008. PMID: 18816424 Review.
Cited by
-
Reaching for sound measures: an ecologically valid estimate of spatial hearing in 2- to 3-year-old children with bilateral cochlear implants.Otol Neurotol. 2013 Apr;34(3):429-35. doi: 10.1097/MAO.0b013e31827de2b3. Otol Neurotol. 2013. PMID: 23370551 Free PMC article.
-
Current and planned cochlear implant research at New York University Laboratory for Translational Auditory Research.J Am Acad Audiol. 2012 Jun;23(6):422-37. doi: 10.3766/jaaa.23.6.5. J Am Acad Audiol. 2012. PMID: 22668763 Free PMC article.
-
Neural Coding of Interaural Time Differences with Bilateral Cochlear Implants in Unanesthetized Rabbits.J Neurosci. 2016 May 18;36(20):5520-31. doi: 10.1523/JNEUROSCI.3795-15.2016. J Neurosci. 2016. PMID: 27194332 Free PMC article.
-
The development of the Nucleus Freedom Cochlear implant system.Trends Amplif. 2006 Dec;10(4):175-200. doi: 10.1177/1084713806296386. Trends Amplif. 2006. PMID: 17172547 Free PMC article. Review.
-
Binaural-bimodal fitting or bilateral implantation for managing severe to profound deafness: a review.Trends Amplif. 2007 Sep;11(3):161-92. doi: 10.1177/1084713807304357. Trends Amplif. 2007. PMID: 17709573 Free PMC article. Review.
References
-
- Armstrong M, Pegg P, James C, Blarney P. Speech perception in noise with implant and hearing aid. American Journal of Otolaryngology. 1997;18(Suppl 6):S140–S141. - PubMed
-
- Ashmead DH, Clifton RK, Ferris EE. Precision of auditory localization in human infants. Developmental Psychology. 1987;23:641–647.
-
- Blauert J. Spatial Hearing: The Psychophysics of Human Sound Localization. 2. Cambridge, MA: The MIT Press; 1997.
-
- Boothroyd A, Boothroyd-Turner D. Postimplantation audition and educational attainment in children with prelingually acquired profound deafness. Annals of Otology, Rkinology, and Laryngology Supplement. 2002;189:79–84. - PubMed
-
- Breebaart J, Kohlrausch A. The influence of interaural stimulus uncertainty on binaural signal detection. Journal of the Acoustical Society of America. 2001;109:331–345. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
