

Intra-articular hyaluronic acid for the treatment of osteoarthritis of the knee: systematic review and meta-analysis
- PMID: 15824412
- PMCID: PMC556045
- DOI: 10.1503/cmaj.1041203
Intra-articular hyaluronic acid for the treatment of osteoarthritis of the knee: systematic review and meta-analysis
Abstract
Background: Osteoarthritis of the knee affects up to 10% of the elderly population. The condition is frequently treated by intra-articular injection of hyaluronic acid. We performed a systematic review and meta-analysis of randomized controlled trials to assess the effectiveness of this treatment.
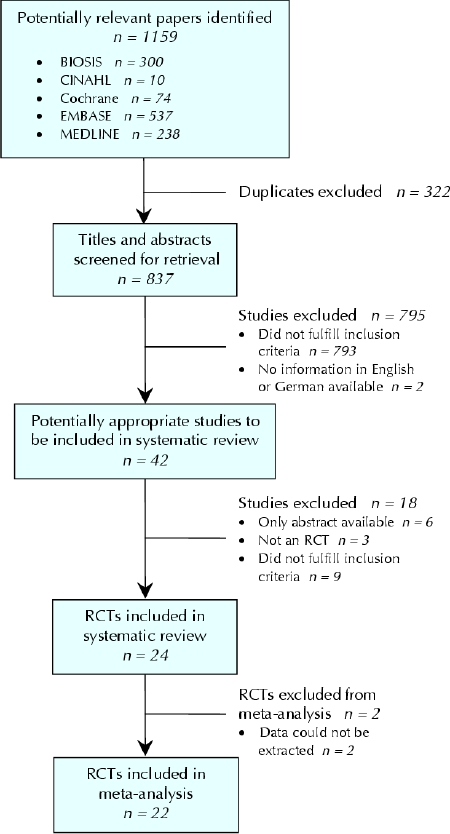
Methods: We searched MEDLINE, EMBASE, CINAHL, BIOSIS and the Cochrane Controlled Trial Register from inception until April 2004 using a combination of search terms for knee osteoarthritis and hyaluronic acid and a filter for randomized controlled trials. We extracted data on pain at rest, pain during or immediately after movement, joint function and adverse events.
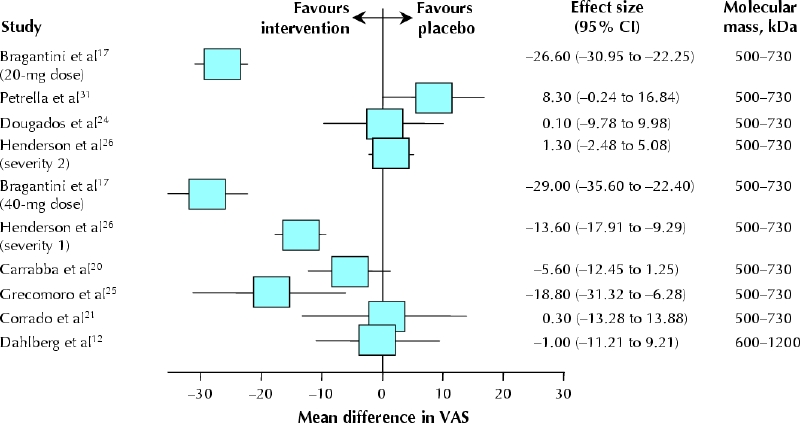
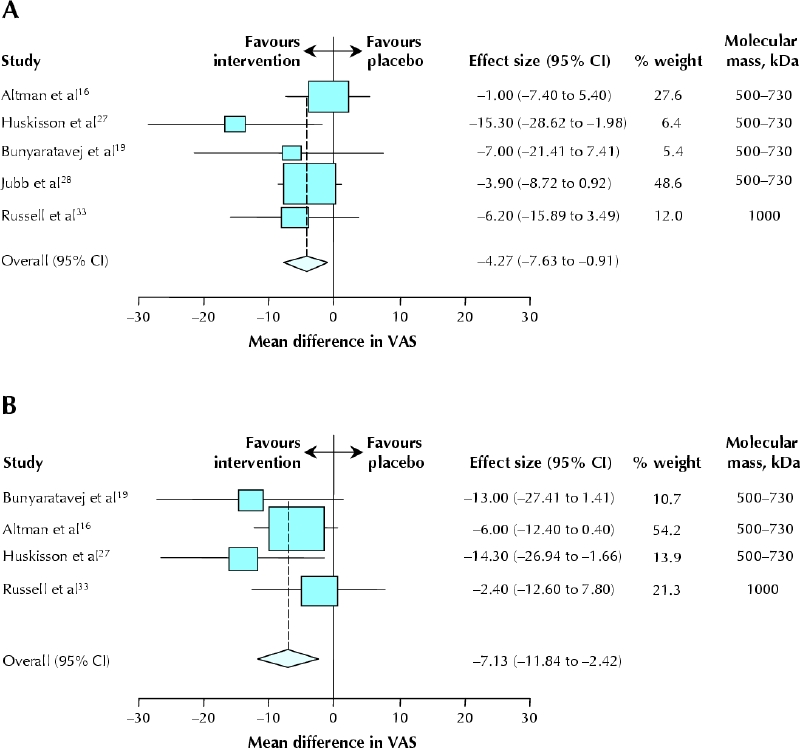
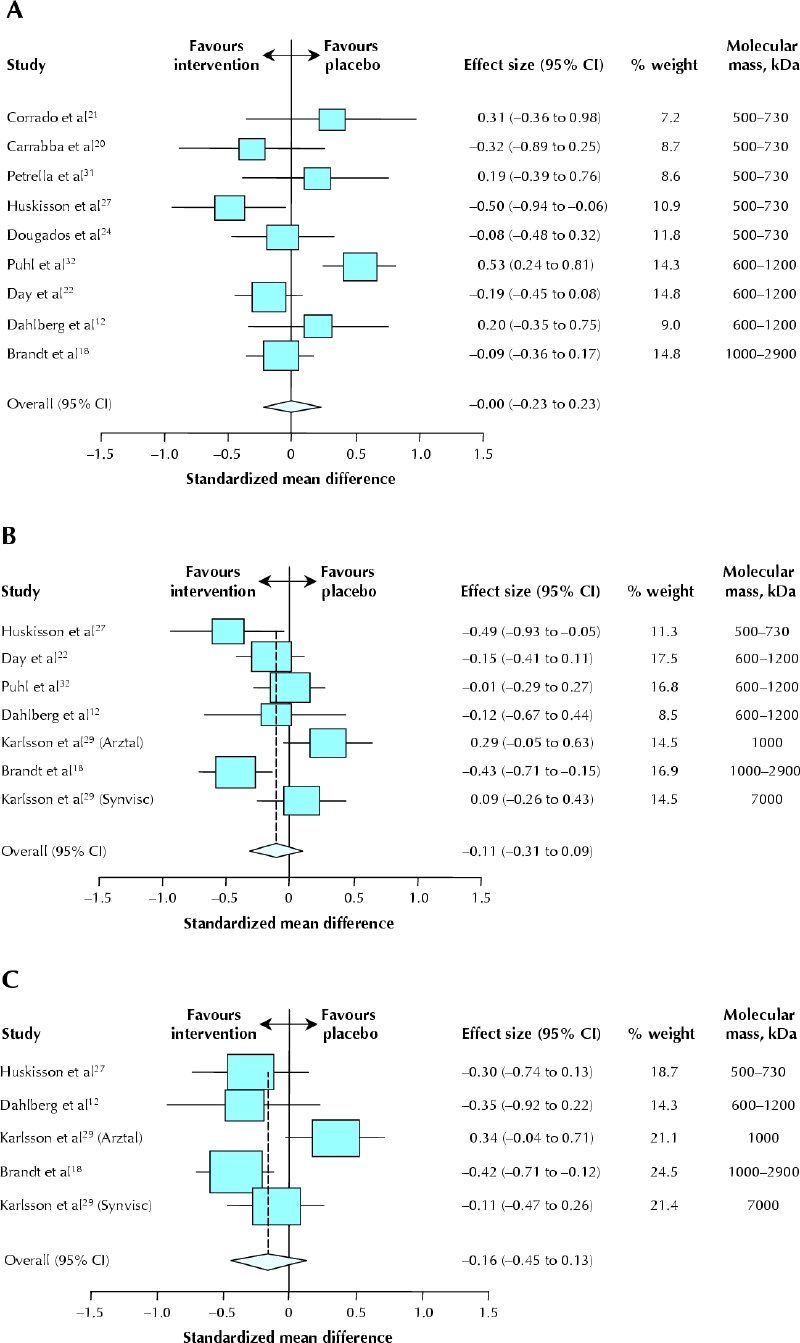
Results: Twenty-two trials that reported usable quantitative information on any of the predefined end points were identified and included in the systematic review. Even though pain at rest may be improved by hyaluronic acid, the data available from these studies did not allow an appropriate assessment of this end point. Patients who received the intervention experienced a reduction in pain during movement: the mean difference on a 100-mm visual analogue scale was -3.8 mm (95% confidence interval [CI] -9.1 to 1.4 mm) after 2-6 weeks, -4.3 mm (95% CI -7.6 to -0.9 mm) after 10-14 weeks and -7.1 mm (95% CI -11.8 to -2.4 mm) after 22-30 weeks. However, this effect was not compatible with a clinically meaningful difference (expected to be about 15 mm on the visual analogue scale). Furthermore, the effect was exaggerated by trials not reporting an intention-to-treat analysis. No improvement in knee function was observed at any time point. Even so, the effect of hyaluronic acid on knee function was more favourable when allocation was not concealed. Adverse events occurred slightly more often among patients who received the intervention (relative risk 1.08, 95% CI 1.01 to 1.15). Only 4 trials explicitly reported allocation concealment, had blinded outcome assessment and presented intention-to-treat data.
Interpretation: According to the currently available evidence, intra-articular hyaluronic acid has not been proven clinically effective and may be associated with a greater risk of adverse events. Large trials with clinically relevant and uniform end points are necessary to clarify the benefit-risk ratio.
Figures
Similar articles
-
Therapeutic effects of hyaluronic acid on osteoarthritis of the knee. A meta-analysis of randomized controlled trials.J Bone Joint Surg Am. 2004 Mar;86(3):538-45. doi: 10.2106/00004623-200403000-00012. J Bone Joint Surg Am. 2004. PMID: 14996880
-
Intra-articular hyaluronic acid in treatment of knee osteoarthritis: a meta-analysis.JAMA. 2003 Dec 17;290(23):3115-21. doi: 10.1001/jama.290.23.3115. JAMA. 2003. PMID: 14679274
-
Hylan versus hyaluronic acid for osteoarthritis of the knee: a systematic review and meta-analysis.Arthritis Rheum. 2007 Dec 15;57(8):1410-8. doi: 10.1002/art.23103. Arthritis Rheum. 2007. PMID: 18050181 Review.
-
Intra-Articular, Single-Shot Hylan G-F 20 Hyaluronic Acid Injection Compared with Corticosteroid in Knee Osteoarthritis: A Double-Blind, Randomized Controlled Trial.J Bone Joint Surg Am. 2016 Jun 1;98(11):885-92. doi: 10.2106/JBJS.15.00544. J Bone Joint Surg Am. 2016. PMID: 27252432 Clinical Trial.
-
Therapeutic trajectory of hyaluronic acid versus corticosteroids in the treatment of knee osteoarthritis: a systematic review and meta-analysis.Arthritis Rheum. 2009 Dec 15;61(12):1704-11. doi: 10.1002/art.24925. Arthritis Rheum. 2009. PMID: 19950318 Review.
Cited by
-
Intra-articular viscosupplementation with hylan g-f 20 to treat osteoarthritis of the knee: an evidence-based analysis.Ont Health Technol Assess Ser. 2005;5(10):1-66. Epub 2005 Jun 1. Ont Health Technol Assess Ser. 2005. PMID: 23074461 Free PMC article.
-
International differences in sport medicine access and clinical management.Muscles Ligaments Tendons J. 2013 Jan 21;2(4):248-52. Print 2012 Oct. Muscles Ligaments Tendons J. 2013. PMID: 23738305 Free PMC article.
-
Intra-articular hyaluronans: the treatment of knee pain in osteoarthritis.J Pain Res. 2010 May 10;3:51-6. doi: 10.2147/jpr.s4733. J Pain Res. 2010. PMID: 21197309 Free PMC article.
-
[Conservative local therapy of inflammation of joints: local invasive forms of therapy].Z Rheumatol. 2007 Sep;66(5):382-7. doi: 10.1007/s00393-007-0195-z. Z Rheumatol. 2007. PMID: 17721706 Review. German.
-
"Turn on" room-temperature phosphorescent biosensors for detection of hyaluronic acid based on manganese-doped ZnS quantum dots.RSC Adv. 2018 Jan 12;8(6):2873-2879. doi: 10.1039/c7ra11858a. eCollection 2018 Jan 12. RSC Adv. 2018. PMID: 35541178 Free PMC article.
References
-
- Lajeunesse D, Delalandre A, Martel-Pelletier J, Pelletier JP. Hyaluronic acid reverses the abnormal synthetic activity of human osteoarthritic subchondral bone osteoblasts. Bone 2003;33:703-10. - PubMed
-
- Jordan KM, Sawyer S, Coakley P, Smith HE, Cooper C, Arden NK. The use of conventional and complementary treatments for knee osteoarthritis in the community. Rheumatology (Oxford) 2004;43:381-4. - PubMed
-
- Pendleton A, Arden N, Dougados M, Doherty M, Bannwarth B, Bijlsma JW, et al. EULAR recommendations for the management of knee osteoarthritis: report of a task force of the Standing Committee for International Clinical Studies Including Therapeutic Trials (ESCISIT). Ann Rheum Dis 2000; 59: 936-44. - PMC - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Miscellaneous