

Medical treatment of viral pneumonia including SARS in immunocompetent adult
- PMID: 15474623
- PMCID: PMC7112637
- DOI: 10.1016/j.jinf.2004.07.010
Medical treatment of viral pneumonia including SARS in immunocompetent adult
Abstract
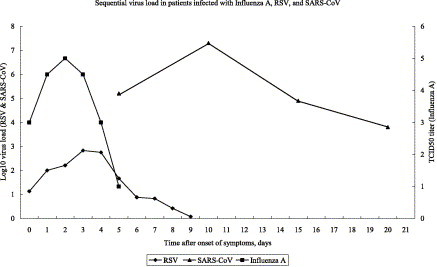
Since no randomized controlled trials have been conducted on the treatment of viral pneumonia by antivirals or immunomodulators in immunocompetent adults, a review of such anecdotal experience are needed for the more rational use of such agents. Case reports (single or case series) with details on their treatment and outcome in the English literature can be reviewed for pneumonia caused by human or avian influenza A virus (50 patients), varicella zoster virus (120), adenovirus (29), hantavirus (100) and SARS coronavirus (SARS-CoV) (841). Even with steroid therapy alone, the mortality rate appeared to be lower when compared with conservative treatment for pneumonia caused by human influenza virus (12.5% vs. 42.1%) and hantavirus (13.3% vs. 63.4%). Combination of an effective antiviral, acyclovir, with steroid in the treatment of varicella zoster virus may be associated with a lower mortality than acyclovir alone (0% vs. 10.3%). Combination of interferon alfacon-1 plus steroid, or lopinavir/ritonavir, ribavirin plus steroid were associated with a better outcome than ribavirin plus steroid (0% vs. 2.3% vs. 7.7%, respectively). Combination of lopinavir/ritonavir plus ribavirin significantly reduced the virus load of SARS-CoV in nasopharyngeal, serum, stool and urine specimens taken between day 10 and 15 after symptom onset when compared with the historical control group treated with ribavirin. It appears that the combination of an effective antiviral and steroid was associated with a better outcome. Randomized therapeutic trial should be conducted to ascertain the relative usefulness of antiviral alone or in combination with steroid.
Figures
Similar articles
-
Role of lopinavir/ritonavir in the treatment of SARS: initial virological and clinical findings.Thorax. 2004 Mar;59(3):252-6. doi: 10.1136/thorax.2003.012658. Thorax. 2004. PMID: 14985565 Free PMC article. Clinical Trial.
-
Pro/con clinical debate: steroids are a key component in the treatment of SARS. Con: No, steroids are not a key component of the treatment regimen for SARS.Crit Care. 2004 Apr;8(2):105-7. Crit Care. 2004. PMID: 15515216 No abstract available.
-
SARS: pharmacotherapy.Respirology. 2003 Nov;8 Suppl:S25-30. doi: 10.1046/j.1440-1843.2003.00525.x. Respirology. 2003. PMID: 15018130 Review.
-
Interferon alfacon-1 plus corticosteroids in severe acute respiratory syndrome: a preliminary study.JAMA. 2003 Dec 24;290(24):3222-8. doi: 10.1001/jama.290.24.3222. JAMA. 2003. PMID: 14693875
-
The management of coronavirus infections with particular reference to SARS.J Antimicrob Chemother. 2008 Sep;62(3):437-41. doi: 10.1093/jac/dkn243. Epub 2008 Jun 18. J Antimicrob Chemother. 2008. PMID: 18565970 Free PMC article. Review.
Cited by
-
Avian influenza virus infections in humans.Chest. 2006 Jan;129(1):156-68. doi: 10.1378/chest.129.1.156. Chest. 2006. PMID: 16424427 Free PMC article. Review.
-
Clinical review: update of avian influenza A infections in humans.Crit Care. 2007;11(2):209. doi: 10.1186/cc5675. Crit Care. 2007. PMID: 17419881 Free PMC article. Review.
-
Successful treatment of parainfluenza virus 3 pneumonia with oral ribavirin and methylprednisolone in a bone marrow transplant recipient.Int J Hematol. 2008 Oct;88(3):336-340. doi: 10.1007/s12185-008-0148-6. Epub 2008 Aug 19. Int J Hematol. 2008. PMID: 18712461
-
A 72-Year-Old Woman With Respiratory Failure and Bilateral Ground-Glass Opacities.Chest. 2020 Jul;158(1):e41-e45. doi: 10.1016/j.chest.2019.11.054. Epub 2020 Jul 2. Chest. 2020. PMID: 32654738 Free PMC article.
-
COVID-19: Progress in diagnostics, therapy and vaccination.Theranostics. 2020 Jun 19;10(17):7821-7835. doi: 10.7150/thno.47987. eCollection 2020. Theranostics. 2020. PMID: 32685022 Free PMC article. Review.
References
-
- Guan Y., Zheng B.J., He Y.Q. Isolation and characterization of viruses related to the SARS coronavirus from animals in southern China. Science. 2003;302:276–278. - PubMed
-
- Poutanen S.M., Low D.E., Henry B. Identification of severe acute respiratory syndrome in Canada. N Engl J Med. 2003;348:1995–2005. - PubMed
-
- Tsang K.W., Ho P.L., Ooi G.C. A cluster of cases of severe acute respiratory syndrome in Hong Kong. N Engl J Med. 2003;348:1977–1985. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Miscellaneous
