

Enhanced cytomegalovirus infection in atherosclerotic human blood vessels
- PMID: 14742264
- PMCID: PMC1602282
- DOI: 10.1016/S0002-9440(10)63148-3
Enhanced cytomegalovirus infection in atherosclerotic human blood vessels
Abstract
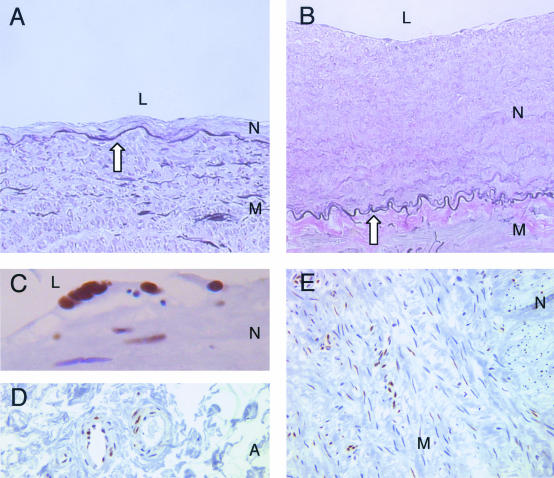
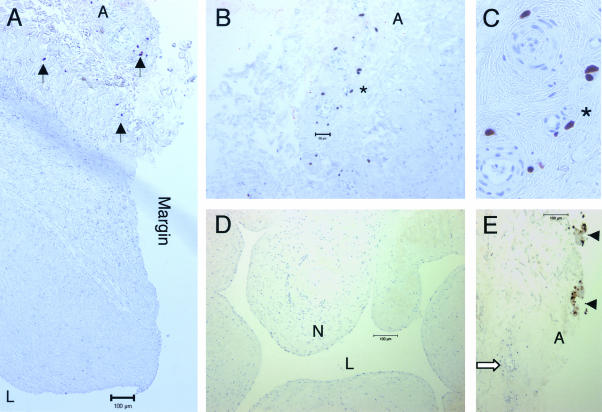
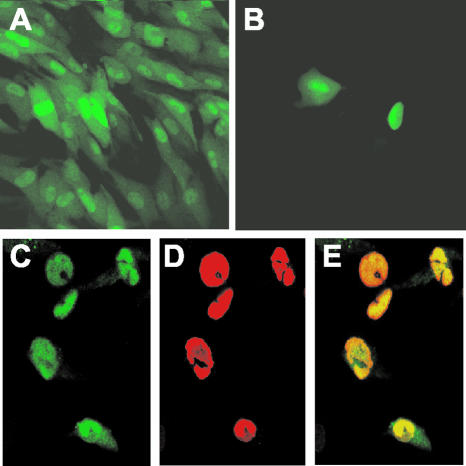
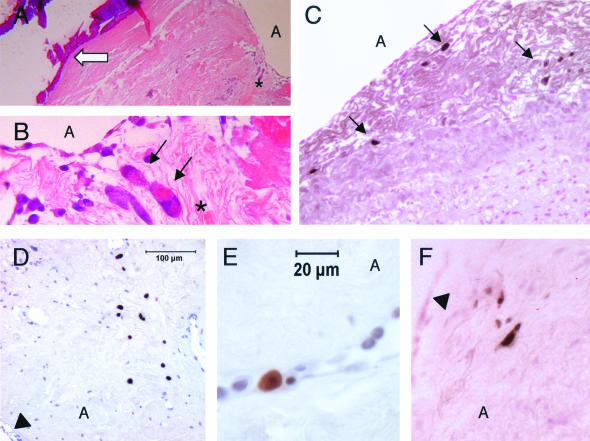
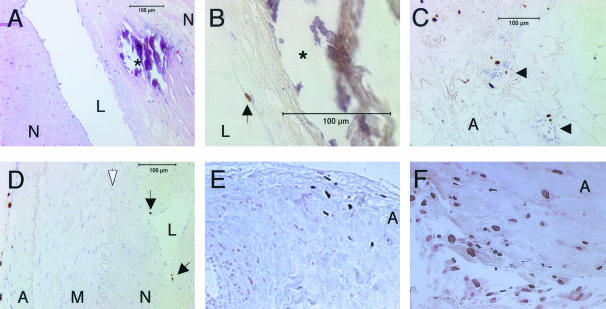
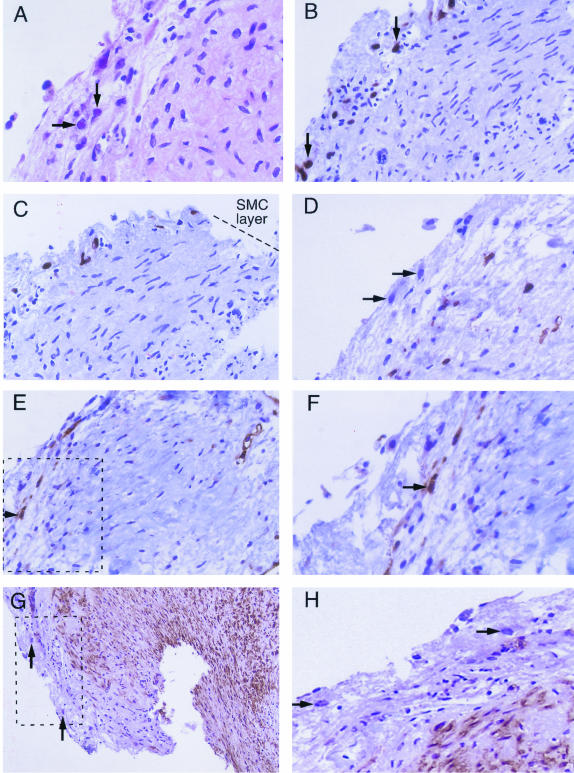
Human cytomegalovirus (CMV) is a possible co-factor in atherogenesis and vascular occlusion, but its ability to actively infect medium and large blood vessels is unclear. A vascular explant model was adapted to investigate CMV infection in human coronary artery, internal mammary artery (IMA), and saphenous vein (SV). Vascular explants were inoculated with CMV Towne or low-passage clinical isolate and examined in situ for CMV cytopathic effect and immediate-early and early antigens, as indicators of active infection. At 5 to 7 days after inoculation, we found that CMV Towne actively infected eight of eight different atherosclerotic blood vessel explants (coronary artery, n = 4; SV and IMA grafts, n = 4), whereas it only infected 2 of 14 nonatherosclerotic blood vessel explants (SV, n = 10; IMA, n = 4) (P = 0.001). The CMV clinical isolate actively infected none of six sets of nonatherosclerotic SV explants at 5 to 7 days after inoculation. The active CMV infections involved adventitial and, less frequently, intimal cells. A small subset of infected cells in atherosclerotic tissue expresses the endothelial cell marker CD31. Smooth muscle cells residing in both atherosclerotic and nonatherosclerotic blood vessels were free of active CMV infections even after all vascular tissue layers were exposed to the virus. In contrast, active CMV Towne infection was evident at 2 days after inoculation in smooth muscle cells and endothelial cells previously isolated from the SV tissues. We conclude that active CMV infection is enhanced in atherosclerotic blood vessels compared to atherosclerosis-free vascular equivalents, and this viral activity is restricted to subpopulations of intimal and adventitial cells.
Figures
Similar articles
-
Cytomegalovirus aggravates intimal hyperplasia in rats by stimulating smooth muscle cell proliferation.Microbes Infect. 2005 Feb;7(2):164-70. doi: 10.1016/j.micinf.2004.10.008. Epub 2005 Jan 27. Microbes Infect. 2005. PMID: 15716015
-
Cytomegalovirus genome and the immediate-early antigen in cells of different layers of human aorta.Virchows Arch. 2000 Jun;436(6):539-52. doi: 10.1007/s004289900173. Virchows Arch. 2000. PMID: 10917167
-
Cytomegalovirus antigen expression, endothelial cell proliferation, and intimal thickening in rat cardiac allografts after cytomegalovirus infection.Circulation. 1995 Nov 1;92(9):2594-604. doi: 10.1161/01.cir.92.9.2594. Circulation. 1995. PMID: 7586362
-
Cytomegalovirus infection and cardiac allograft vasculopathy.Transpl Infect Dis. 1999 Jun;1(2):115-26. doi: 10.1034/j.1399-3062.1999.010205.x. Transpl Infect Dis. 1999. PMID: 11428979 Review.
-
Cytomegalovirus and atherosclerosis.Arch Immunol Ther Exp (Warsz). 1996;44(5-6):297-302. Arch Immunol Ther Exp (Warsz). 1996. PMID: 9017143 Review.
Cited by
-
Cytomegalovirus infection causes an increase of arterial blood pressure.PLoS Pathog. 2009 May;5(5):e1000427. doi: 10.1371/journal.ppat.1000427. Epub 2009 May 15. PLoS Pathog. 2009. PMID: 19436702 Free PMC article.
-
Human cytomegalovirus modulates mTORC1 to redirect mRNA translation within quiescently infected monocytes.J Virol. 2024 Feb 20;98(2):e0188823. doi: 10.1128/jvi.01888-23. Epub 2024 Jan 30. J Virol. 2024. PMID: 38289104 Free PMC article.
-
Infectious serologies and autoantibodies in hepatitis C and autoimmune disease-associated mixed cryoglobulinemia.Clin Rev Allergy Immunol. 2012 Apr;42(2):238-46. doi: 10.1007/s12016-011-8275-x. Clin Rev Allergy Immunol. 2012. PMID: 21633930 Review.
-
Infectious myocarditis: the role of the cardiac vasculature.Heart Fail Rev. 2018 Jul;23(4):583-595. doi: 10.1007/s10741-018-9688-x. Heart Fail Rev. 2018. PMID: 29536322 Free PMC article. Review.
-
Significant increase in 1-year posttransplant renal arterial index predicts graft loss.Clin J Am Soc Nephrol. 2010 Oct;5(10):1867-72. doi: 10.2215/CJN.01210210. Epub 2010 Jul 8. Clin J Am Soc Nephrol. 2010. PMID: 20616164 Free PMC article.
References
-
- Levi M. CMV endothelitis as a factor in the pathogenesis of atherosclerosis. Cardiovasc Res. 2001;50:432–433. - PubMed
-
- Bruggeman CA, Marjorie HJ, Nelissen-Vrancken G. Cytomegalovirus and atherosclerosis. Antiviral Res. 1999;43:191–200. - PubMed
-
- Epstein SE, Speir E, Zhou YF, Guetta E, Leon M, Finkel T. The role of infection in restenosis and atherosclerosis: focus on cytomegalovirus. Lancet. 1996;348:13–17. - PubMed
-
- Nieto FJ, Adam E, Farzadegan H, Melnick JL, Comstock GW, Szklo M. Cohort study of cytomegalovirus infection as a risk factor for carotid intimal-medial thickening, a measure of subclinical atherosclerosis. Circulation. 1996;94:922–927. - PubMed
-
- Zhou YF, Leon MB, Waclawiw MA, Popma JJ, Yu ZX, Finkel T, Epstein SE. Association between prior cytomegalovirus infection and the risk of restenosis after coronary atherectomy. N Engl J Med. 1996;335:624–630. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
