

A monoclonal antibody recognizing human cancers with amplification/overexpression of the human epidermal growth factor receptor
- PMID: 12515857
- PMCID: PMC141049
- DOI: 10.1073/pnas.232686499
A monoclonal antibody recognizing human cancers with amplification/overexpression of the human epidermal growth factor receptor
Erratum in
- Proc Natl Acad Sci U S A. 2003 Feb 18;100(4):2163. Cavanee, Webster K [corrected to Cavenee, Webster K]
Abstract
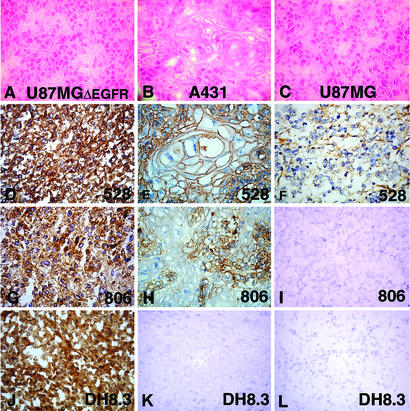
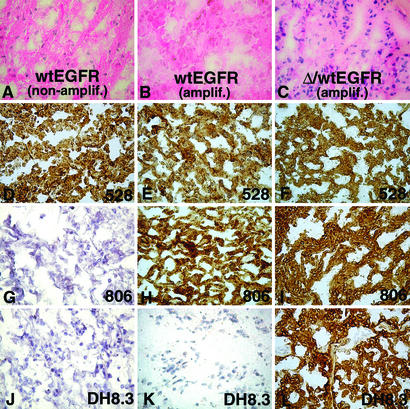
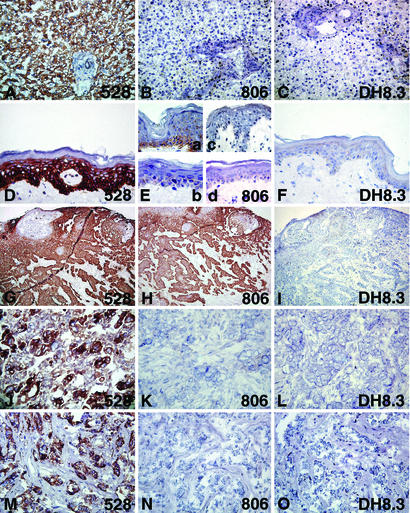
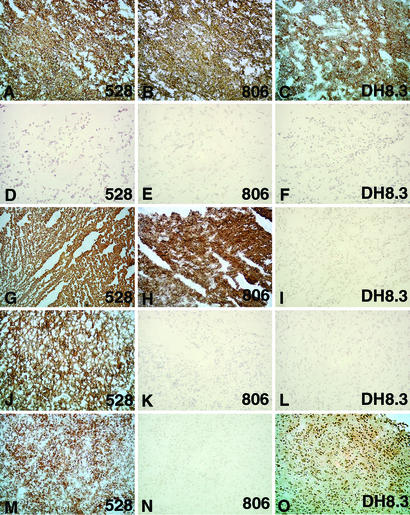
Epidermal growth factor receptor (EGFR) has attracted considerable attention as a target for cancer therapy. Wild-type (wt)EGFR is amplified/overexpressed in a number of tumor types, and several mutant forms of the coding gene have been found, with DeltaEGFR, a deletion mutation lacking exons 2-7 of the external domain, being the most common and particularly associated with glioblastoma. We generated monoclonal antibodies (mAbs) against NR6(DeltaEGFR) (mouse fibroblast line NR6 transfected with DeltaEGFR). mAb 806 with selective reactivity for NR6(DeltaEGFR) in mixed hemadsorption assays, fluorescence-activated cell sorting, Western blot, and immunohistochemistry was analyzed in detail and compared with mAbs 528 (anti-wtEGFR) and DH8.3 (anti-DeltaEGFR). In xenograft tumors and molecularly pretyped glioblastomas, the reactivity pattern was as follows: 528 reactive with amplified and nonamplified wtEGFR; DH8.3 reactive with DeltaEGFR; and 806 reactive with amplified/overexpressed wtEGFR (with or without DeltaEGFR). In normal tissues, 528 but not DH8.3 or 806 was widely reactive with many organs, e.g., liver expressing high EGFR levels. In glioblastoma and non-CNS tumor panels, 806 was reactive with a high proportion of glioblastomas and a substantial number of epithelial cancers of lung and of head and neck. DH8.3 reactivity was restricted to DeltaEGFR-positive glioblastoma. Thus, 806 represents a category of mAbs that recognizes tumors with EGFR amplification/overexpression but not normal tissues or tumors with normal EGFR levels. Our study also indicates that DeltaEGFR is restricted to glioblastoma, in contrast to other reports that this mutation is found in tumors outside the brain.
Figures
Similar articles
-
Growth suppression of intracranial xenografted glioblastomas overexpressing mutant epidermal growth factor receptors by systemic administration of monoclonal antibody (mAb) 806, a novel monoclonal antibody directed to the receptor.Cancer Res. 2001 Jul 15;61(14):5349-54. Cancer Res. 2001. PMID: 11454673
-
Monoclonal antibody 806 inhibits the growth of tumor xenografts expressing either the de2-7 or amplified epidermal growth factor receptor (EGFR) but not wild-type EGFR.Cancer Res. 2001 Jul 15;61(14):5355-61. Cancer Res. 2001. PMID: 11454674
-
A common mutant epidermal growth factor receptor confers enhanced tumorigenicity on human glioblastoma cells by increasing proliferation and reducing apoptosis.Cancer Res. 1996 Nov 1;56(21):5079-86. Cancer Res. 1996. PMID: 8895767
-
Mutant epidermal growth factor receptor signaling down-regulates p27 through activation of the phosphatidylinositol 3-kinase/Akt pathway in glioblastomas.Cancer Res. 2002 Nov 15;62(22):6764-9. Cancer Res. 2002. PMID: 12438278
-
Monoclonal antibodies against EGFRvIII are tumor specific and react with breast and lung carcinomas and malignant gliomas.Cancer Res. 1995 Jul 15;55(14):3140-8. Cancer Res. 1995. PMID: 7606735
Cited by
-
An efficient strategy for cell-based antibody library selection using an integrated vector system.BMC Biotechnol. 2012 Sep 18;12:62. doi: 10.1186/1472-6750-12-62. BMC Biotechnol. 2012. PMID: 22989299 Free PMC article.
-
Advances in immunotherapeutic targets for childhood cancers: A focus on glypican-2 and B7-H3.Pharmacol Ther. 2021 Jul;223:107892. doi: 10.1016/j.pharmthera.2021.107892. Epub 2021 May 14. Pharmacol Ther. 2021. PMID: 33992682 Free PMC article. Review.
-
Emerging drugs to treat squamous cell carcinomas of the head and neck.Expert Opin Emerg Drugs. 2010 Sep;15(3):355-73. doi: 10.1517/14728214.2010.497754. Expert Opin Emerg Drugs. 2010. PMID: 20557270 Free PMC article. Review.
-
Therapeutic anti-EGFR antibody 806 generates responses in murine de novo EGFR mutant-dependent lung carcinomas.J Clin Invest. 2007 Feb;117(2):346-52. doi: 10.1172/JCI30446. Epub 2007 Jan 25. J Clin Invest. 2007. PMID: 17256054 Free PMC article.
-
A phase I clinical trial with monoclonal antibody ch806 targeting transitional state and mutant epidermal growth factor receptors.Proc Natl Acad Sci U S A. 2007 Mar 6;104(10):4071-6. doi: 10.1073/pnas.0611693104. Epub 2007 Feb 28. Proc Natl Acad Sci U S A. 2007. PMID: 17360479 Free PMC article. Clinical Trial.
References
-
- Mach J P. In: Oxford Textbook of Oncology. Peckham M, Pinedo H M, Veronesi U, editors. Vol. 1. Oxford: Oxford Univ. Press; 1995. pp. 81–103.
-
- Prenzel N, Fischer O M, Streit S, Hart S, Ullrich A. Endocr Relat Cancer. 2001;8:11–31. - PubMed
-
- Nicholson R I, Gee J M, Harper M E. Eur J Cancer. 2001;37, Suppl. 4:S9–S15. - PubMed
-
- Libermann T A, Nusbaum H R, Razon N, Kris R, Lax I, Soreq H, Whittle N, Waterfield M D, Ullrich A, Schlessinger J. Nature. 1985;313:144–147. - PubMed
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Research Materials
Miscellaneous
