

Histologic tumor type is an independent prognostic parameter in esophageal cancer: lessons from more than 1,000 consecutive resections at a single center in the Western world
- PMID: 11524589
- PMCID: PMC1422027
- DOI: 10.1097/00000658-200109000-00010
Histologic tumor type is an independent prognostic parameter in esophageal cancer: lessons from more than 1,000 consecutive resections at a single center in the Western world
Abstract
Objective: To analyze the changing pattern in tumor type and postoperative deaths at a national referral center for esophageal cancer in the Western world and to assess prognostic factors for long-term survival after resection.
Summary background data: During the past two decades, the epidemiology and treatment strategies of esophageal cancer have changed markedly in the Western world. The influence of these factors on postoperative deaths and long-term prognosis has not been adequately evaluated.
Methods: Between 1982 and 2000, 1,059 patients with primary esophageal squamous cell cancer or adenocarcinoma had resection with curative intention at a single center. Patient and tumor characteristics and details of the surgical procedure and outcome were documented during this period. Follow-up was available for 95.8% of the patients. Changing patterns in tumor type and postoperative deaths were analyzed. Prognostic factors for long-term survival were assessed by multivariate analysis.
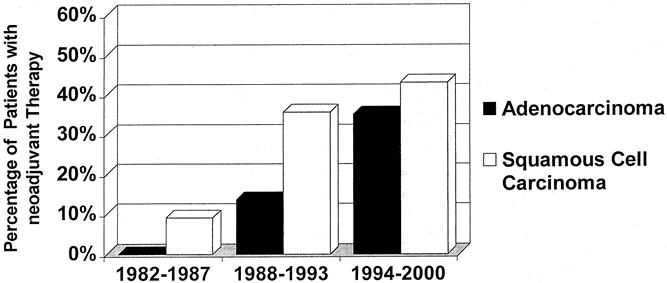
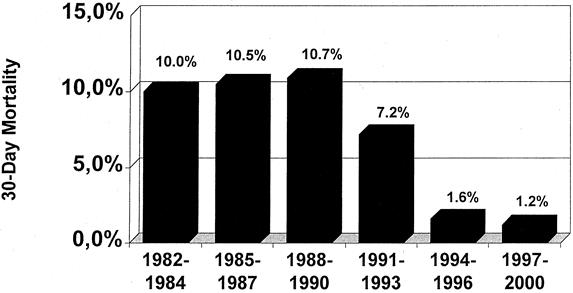
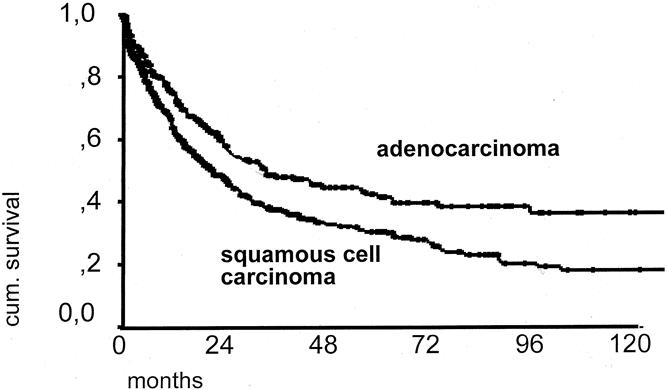
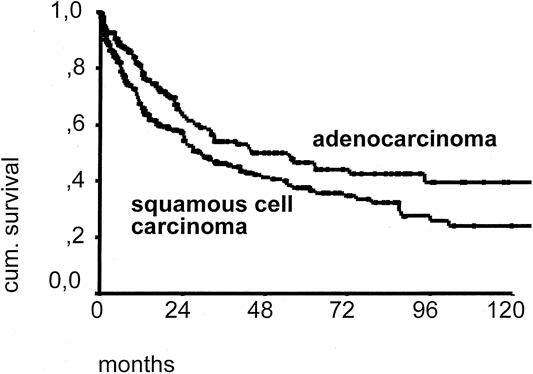
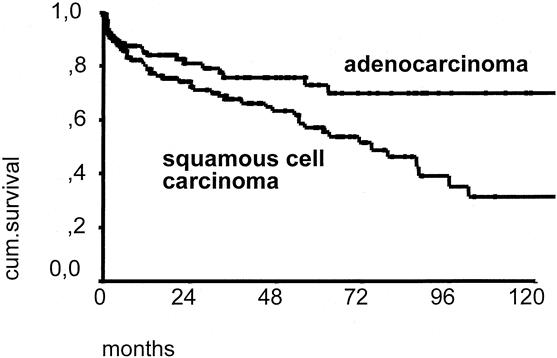
Results: The prevalence of adenocarcinoma in patients with resected esophageal cancer increased markedly during the study period. The postoperative death rate decreased from about 10% before 1990 to less than 2% since 1994, coinciding with the introduction of a procedure-specific composite risk score and exclusion of high-risk patients from surgical resection. In addition to the well-established prognostic parameters, tumor cell type "adenocarcinoma" was identified as a favorable independent predictor of long-term survival after resection. The independent prognostic effect of tumor cell type persisted in the subgroups of patients with primary resection and patients with primary resection and R0 category.
Conclusion: Esophagectomy for esophageal cancer has become a safe procedure in experienced hands. Esophageal adenocarcinoma has a better long-term prognosis after resection than squamous cell carcinoma.
Figures

Similar articles
-
Early esophageal cancer: pattern of lymphatic spread and prognostic factors for long-term survival after surgical resection.Ann Surg. 2005 Oct;242(4):566-73; discussion 573-5. doi: 10.1097/01.sla.0000184211.75970.85. Ann Surg. 2005. PMID: 16192817 Free PMC article.
-
Treatment outcomes of resected esophageal cancer.Ann Surg. 2002 Sep;236(3):376-84; discussion 384-5. doi: 10.1097/00000658-200209000-00014. Ann Surg. 2002. PMID: 12192324 Free PMC article.
-
Survival after esophageal resection for carcinoma: the importance of the histologic cell type.Ann Thorac Surg. 2006 Sep;82(3):1073-7. doi: 10.1016/j.athoracsur.2006.03.012. Ann Thorac Surg. 2006. PMID: 16928541
-
Factors affecting postoperative course and survival after en bloc resection for esophageal carcinoma.Ann Thorac Surg. 2004 Oct;78(4):1177-83. doi: 10.1016/j.athoracsur.2004.02.068. Ann Thorac Surg. 2004. PMID: 15464466 Review.
-
Esophageal cancer: patient evaluation and pre-treatment staging.Surg Oncol. 2001 Nov;10(3):103-11. doi: 10.1016/s0960-7404(01)00023-8. Surg Oncol. 2001. PMID: 11750229 Review.
Cited by
-
Comparative evaluation of serum C-reactive protein (CRP) levels in the different histological subtypes of esophageal cancer (squamous cell carcinoma and adenocarcinoma of esophagus).J Clin Lab Anal. 2012 Feb;26(2):73-81. doi: 10.1002/jcla.21486. J Clin Lab Anal. 2012. PMID: 22467322 Free PMC article.
-
Docetaxel and cisplatin concurrent with radiotherapy versus 5-fluorouracil and cisplatin concurrent with radiotherapy in treatment for locally advanced oesophageal squamous cell carcinoma: a randomized clinical study.Med Oncol. 2012 Dec;29(5):3017-23. doi: 10.1007/s12032-012-0228-6. Epub 2012 Apr 5. Med Oncol. 2012. PMID: 22476809 Clinical Trial.
-
Recurrent laryngeal nerve monitoring during totally robot-assisted Ivor Lewis esophagectomy.Langenbecks Arch Surg. 2020 Dec;405(8):1091-1099. doi: 10.1007/s00423-020-01990-0. Epub 2020 Sep 24. Langenbecks Arch Surg. 2020. PMID: 32970189 Free PMC article.
-
Identification of Adenosquamous Carcinoma as a Rare Aggressive HER2-negative Subgroup of Esophageal/Gastroesophageal Junction Adenocarcinoma.Am J Clin Oncol. 2019 Feb;42(2):190-195. doi: 10.1097/COC.0000000000000495. Am J Clin Oncol. 2019. PMID: 30516569 Free PMC article.
-
Prognostic significance of circumferential resection margin involvement following oesophagectomy for cancer.Br J Cancer. 2003 May 19;88(10):1549-52. doi: 10.1038/sj.bjc.6600931. Br J Cancer. 2003. PMID: 12771920 Free PMC article.
References
-
- Swisher SG, Deford L, Merriman KW, et al. Effect of operative volume on morbidity, mortality, and hospital use after esophagectomy for cancer. J Thorac Cardiovasc Surg 2000; 119: 1126–1132. - PubMed
-
- Devesa SS, Blot WJ, Fraumeni JF Jr. Changing patterns in the incidence of esophageal and gastric carcinoma in the United States. Cancer 1998; 83: 2049–2053. - PubMed
-
- Daly JD, Fry WA, Little AG, et al. Esophageal cancer: results of an American College of Surgeons Patient Care Evaluation Study. J Am Coll Surg 2000; 190: 562–573. - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
