

Analysis of reduced death and complication rates after esophageal resection
- PMID: 11224620
- PMCID: PMC1421248
- DOI: 10.1097/00000658-200103000-00006
Analysis of reduced death and complication rates after esophageal resection
Abstract
Objective: To identify factors that have contributed to reduced rates of death and complications after esophageal resection in a 17-year period at a tertiary referral center.
Summary background data: There has been an evolving refinement in surgical technique and perioperative management of patients undergoing esophageal resection at Queen Mary Hospital during the past two decades. As of the end of 1998, there had been no hospital deaths among the last 105 consecutive resections performed for esophageal squamous cancer.
Methods: The results of esophageal resection for squamous cell carcinoma were analyzed using a prospective esophageal database. A longitudinal study was performed to compare and analyze rates of death and complications for three consecutive time periods.
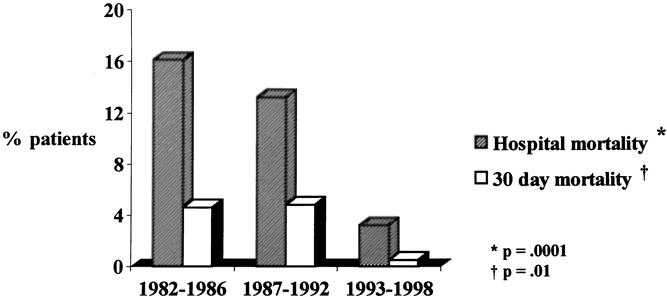
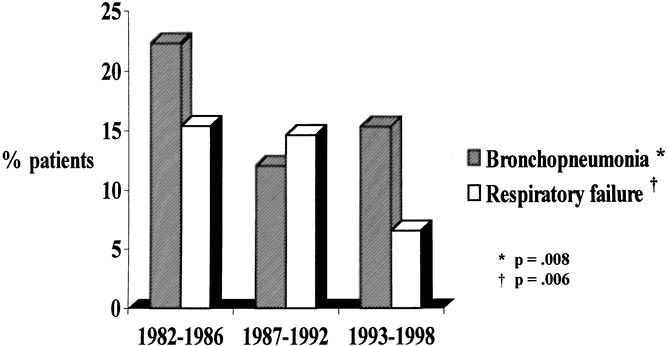
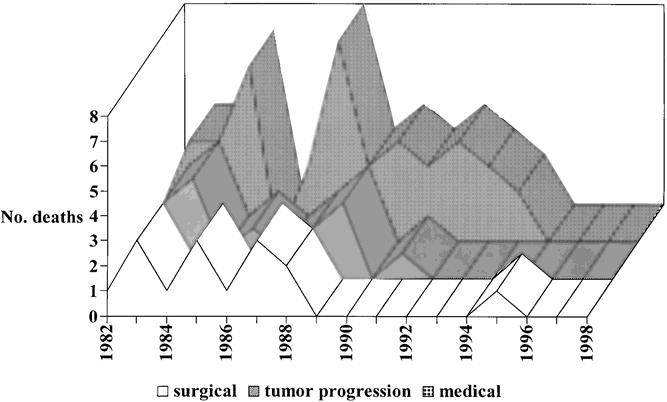
Results: The study group comprised 710 patients who underwent one-stage esophageal resection between 1982 and 1998. A transthoracic esophagectomy was the preferred approach in 590 patients (83%). The overall hospital death rate was 11%. The leading causes of hospital death were pulmonary complications (45.5%) and progression of malignant disease (21.5%); anastomotic leakage accounted for 9% of deaths. During the study period, the hospital death rate decreased from 16% to 3.2%, and the incidence of postoperative respiratory failure decreased from 15.5% to 6.5%. Perioperative factors that correlated with the decreased death rate over time were the increased postoperative use of epidural analgesia and bronchoscopy (for clearance of pulmonary secretions), a decrease in history of smoking, and a decrease in surgical blood loss of more than 1,000 mL.
Conclusions: In this series of predominantly transthoracic esophagectomies, there has been a decline in the hospital death rate to less than 5%. These results are largely attributable to factors aimed at reducing postoperative pulmonary complications.
Figures
Similar articles
-
An audit of surgical outcomes of esophageal squamous cell carcinoma.Eur J Cardiothorac Surg. 2007 Mar;31(3):536-44. doi: 10.1016/j.ejcts.2006.12.002. Epub 2007 Jan 11. Eur J Cardiothorac Surg. 2007. PMID: 17222561
-
Predictive factors for postoperative pulmonary complications and mortality after esophagectomy for cancer.Ann Surg. 2004 Nov;240(5):791-800. doi: 10.1097/01.sla.0000143123.24556.1c. Ann Surg. 2004. PMID: 15492560 Free PMC article.
-
In-hospital mortality after a surgical resection for esophageal cancer: analyses of the associated factors and historical changes.Ann Surg Oncol. 2011 Jun;18(6):1757-65. doi: 10.1245/s10434-010-1502-5. Epub 2011 Jan 5. Ann Surg Oncol. 2011. PMID: 21207167 Clinical Trial.
-
Factors affecting postoperative course and survival after en bloc resection for esophageal carcinoma.Ann Thorac Surg. 2004 Oct;78(4):1177-83. doi: 10.1016/j.athoracsur.2004.02.068. Ann Thorac Surg. 2004. PMID: 15464466 Review.
-
Intrathoracic oesophageal anastomosis: is it worth the risk?Aust N Z J Surg. 2000 Sep;70(9):677-80. doi: 10.1046/j.1440-1622.2000.01923.x. Aust N Z J Surg. 2000. PMID: 10976899 Review. No abstract available.
Cited by
-
The prognostic value of irradiated lung volumes on the prediction of intra-/ post-operative mortality in patients after neoadjuvant radiochemotherapy for esophageal cancer. A retrospective multicenter study.J Cancer. 2015 Jan 20;6(3):254-60. doi: 10.7150/jca.10796. eCollection 2015. J Cancer. 2015. PMID: 25663943 Free PMC article.
-
Endoscopic assessment 1 day after esophagectomy for predicting cervical esophagogastric anastomosis-relating complications.Surg Endosc. 2016 Apr;30(4):1564-71. doi: 10.1007/s00464-015-4379-3. Epub 2015 Jul 14. Surg Endosc. 2016. PMID: 26169637
-
Postoperative complications and perioperative management of lung resection in patients with a history of oesophagectomy for oesophageal carcinoma.Interact Cardiovasc Thorac Surg. 2021 Aug 18;33(3):418-425. doi: 10.1093/icvts/ivab076. Interact Cardiovasc Thorac Surg. 2021. PMID: 34363468 Free PMC article.
-
Ventilatory and intensive care requirements following oesophageal resection.Ann R Coll Surg Engl. 2006 Jul;88(4):354-7. doi: 10.1308/003588406X98694. Ann R Coll Surg Engl. 2006. PMID: 16834853 Free PMC article.
-
An analysis of the factors contributing to a reduction in the incidence of pulmonary complications following an esophagectomy for esophageal cancer.Langenbecks Arch Surg. 2008 Mar;393(2):127-33. doi: 10.1007/s00423-007-0253-7. Epub 2007 Dec 11. Langenbecks Arch Surg. 2008. PMID: 18071746
References
-
- Annual Report 1997–98. Director of Medical and Health Services, Hong Kong Government Press.
-
- Fok M, Law SY, Wong J. Operable esophageal carcinoma: current results from Hong Kong. World J Surg 1994; 18: 355–360. - PubMed
-
- Earlam R, Cunha-Melo JR. Oesophageal squamous cell carcinoma: 1. A critical review of surgery. Br J Surg 1980; 67: 381–390. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous
