

Transhiatal esophagectomy: clinical experience and refinements
- PMID: 10493486
- PMCID: PMC1420884
- DOI: 10.1097/00000658-199909000-00012
Transhiatal esophagectomy: clinical experience and refinements
Abstract
Objective: To review the authors' clinical experience with transhiatal esophagectomy (THE) and the refinements in this procedure that have evolved.
Background: Increased use of THE during the past two decades has generated controversy about the merits and safety of this approach compared with transthoracic esophageal resection. The authors' large THE experience provides a valuable basis for benchmarking data regarding the procedure.
Methods: The results of THE were analyzed retrospectively using the authors' prospectively established esophageal resection database and follow-up information on these patients.
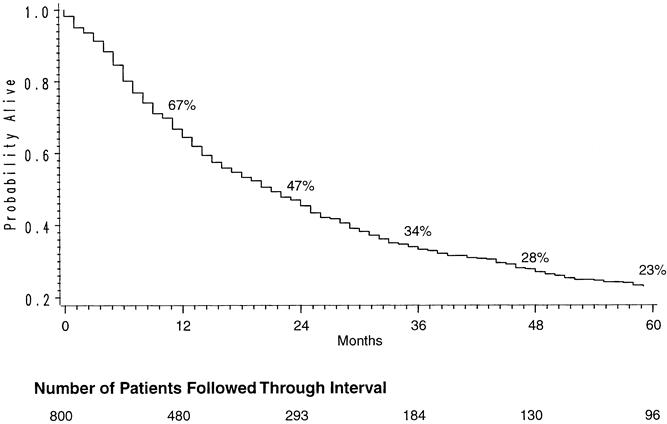
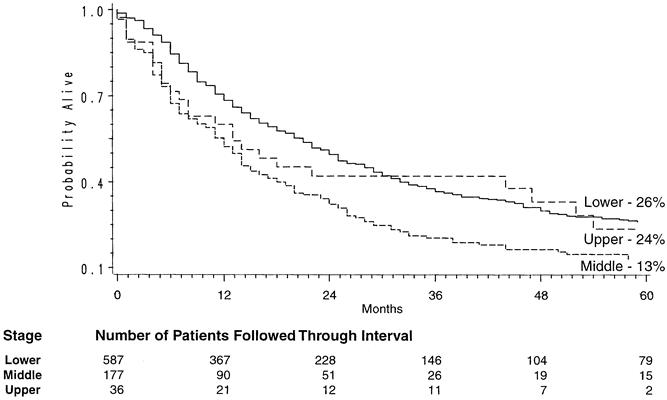
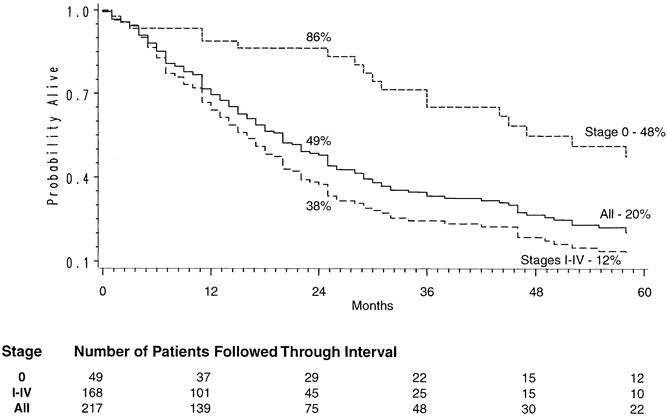
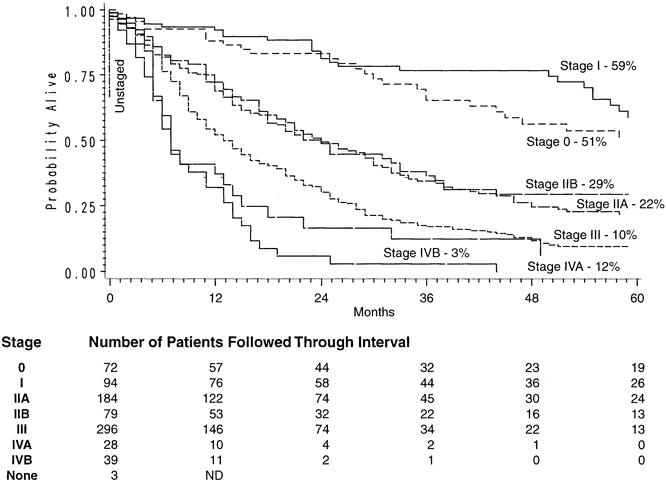
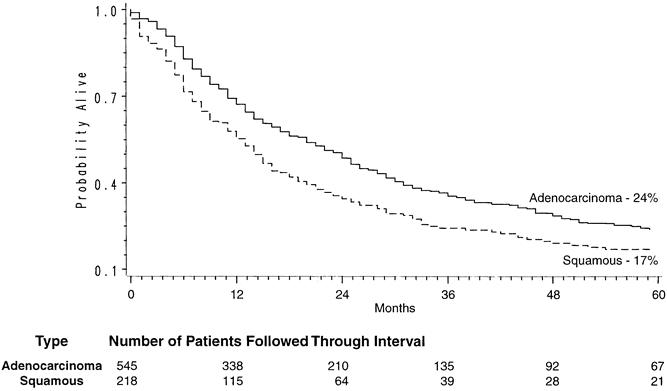
Results: From 1976 to 1998, THE was performed in 1085 patients, 26% with benign disease and 74% with cancer. The procedure was possible in 98.6% of cases. Stomach was the esophageal substitute in 96%. The hospital mortality rate was 4%. Blood loss averaged 689 cc. Major complications were anastomotic leak (13%), atelectasis/pneumonia (2%), intrathoracic hemorrhage, recurrent laryngeal nerve paralysis, chylothorax, and tracheal laceration (<1% each). Actuarial survival of patients with carcinoma equaled or exceeded that reported after transthoracic esophagectomy. Late functional results were good or excellent in 70%. With preoperative pulmonary and physical conditioning, a side-to-side stapled cervical esophagogastric anastomosis (<3% incidence of leak), and postoperative epidural anesthesia, the need for an intensive care unit stay has been eliminated and the length of stay reduced to 7 days.
Conclusion: THE is possible in most patients requiring esophageal resection and can be performed with greater safety and fewer complications than the traditional transthoracic approaches.
Figures
Similar articles
-
Transhiatal esophagectomy for benign and malignant disease.J Thorac Cardiovasc Surg. 1993 Feb;105(2):265-76; discussion 276-7. J Thorac Cardiovasc Surg. 1993. PMID: 8429654
-
Transhiatal esophagectomy for treatment of benign and malignant esophageal disease.World J Surg. 2001 Feb;25(2):196-203. World J Surg. 2001. PMID: 11338022 Review.
-
Two thousand transhiatal esophagectomies: changing trends, lessons learned.Ann Surg. 2007 Sep;246(3):363-72; discussion 372-4. doi: 10.1097/SLA.0b013e31814697f2. Ann Surg. 2007. PMID: 17717440 Free PMC article.
-
[Transhiatal esophagectomy for treatment of benign and malignant esophageal diseases].Rev Med Chir Soc Med Nat Iasi. 2004 Apr-Jun;108(2):390-6. Rev Med Chir Soc Med Nat Iasi. 2004. PMID: 15688820 Romanian.
-
Multimodality therapy for esophageal carcinoma--update.Chest. 1993 Apr;103(4 Suppl):406S-409S. doi: 10.1378/chest.103.4_supplement.406s. Chest. 1993. PMID: 8462336 Review.
Cited by
-
Usefulness of indocyanine green angiography for evaluation of blood supply in a reconstructed gastric tube during esophagectomy.Int Surg. 2012 Oct-Dec;97(4):340-4. doi: 10.9738/CC159.1. Int Surg. 2012. PMID: 23294076 Free PMC article.
-
Optimal management of Barrett's esophagus: pharmacologic, endoscopic, and surgical interventions.Ther Clin Risk Manag. 2011;7:447-58. doi: 10.2147/TCRM.S23425. Epub 2011 Nov 22. Ther Clin Risk Manag. 2011. PMID: 22162921 Free PMC article.
-
Diffusely infiltrative squamous cell carcinoma of the esophagus resembling scirrhous gastric cancer: a case report.Ann Med Surg (Lond). 2023 Feb 7;85(2):266-270. doi: 10.1097/MS9.0000000000000187. eCollection 2023 Feb. Ann Med Surg (Lond). 2023. PMID: 36845766 Free PMC article.
-
Multicenter prospective randomized trial comparing standard esophagectomy with chemoradiotherapy for treatment of squamous esophageal cancer: early results from the Chinese University Research Group for Esophageal Cancer (CURE).J Gastrointest Surg. 2005 Jul-Aug;9(6):794-802. doi: 10.1016/j.gassur.2005.05.005. J Gastrointest Surg. 2005. PMID: 16187480 Clinical Trial.
-
Treatment of thoracic anastomotic leaks after esophagectomy with self-expanding plastic stents.Ann Surg. 2004 Nov;240(5):801-7. doi: 10.1097/01.sla.0000143122.76666.ae. Ann Surg. 2004. PMID: 15492561 Free PMC article.
References
-
- Orringer MB, Sloan H. Esophagectomy without thoracotomy. J Thorac Cardiovasc Surg 1978; 76: 643–654. - PubMed
-
- Katariya K, Harvey JC, Pina E, Beattie EJ. Complications of transhiatal esophagectomy. J Surg Oncol 1994; 57: 157–163. - PubMed
-
- Gandhi SK, Naunheim KS. Complications of transhiatal esophagectomy. Chest Surg Clin North Am 1997; 7: 601–610. - PubMed
-
- Orringer MB, Marshall B, Stirling MC. Transhiatal esophagectomy for benign and malignant disease. J Thorac Cardiovasc Surg 1993; 106: 265–277. - PubMed
-
- Orringer MB, Orringer JS. Transhiatal esophagectomy with thoracotomy: a dangerous operation? J Thorac Cardiovasc Surg 1983; 85: 72–80. - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
