

This systematic review and meta-analysis evaluates the speech perception, sound localization, device use, and subjective outcomes reported in published studies of pediatric patients who received a cochlear implant for single-sided deafness.
Key Points
Question
Is cochlear implantation in children with single-sided deafness associated with improved audiological and patient-reported outcomes?
Findings
In this systematic review and meta-analysis of 12 studies that evaluated 119 children with single-sided deafness, speech perception in noise and quiet as well as sound localization improved after cochlear implantation. Patient-reported audiological outcomes and cochlear implant use rates were higher among children with a shorter duration of deafness.
Meaning
Findings from this study can be used to inform future research efforts, refine cochlear implantation candidacy criteria, and aid in family counseling and shared decision-making.
Abstract
Importance
In 2019, the US Food and Drug Administration approved cochlear implantation for children with single-sided deafness (SSD). The absence of robust clinical data specific to pediatric patients to guide shared decision-making and to identify potential advantages is a challenge in family counseling.
Objective
To evaluate the audiological and patient-reported outcomes in children who underwent cochlear implantation for SSD and to assess the association between time of implantation, subjective outcomes, and cochlear implant device use rates.
Data Source
MEDLINE, Embase, Scopus, Cochrane, and PubMed were searched for English-language articles that were published in a peer-reviewed journal from database inception to February 18, 2020.
Study Selection
Inclusion criteria were designed to capture studies that evaluated pediatric patients (1) younger than 18 years, (2) with a diagnosis of SSD for which they underwent a cochlear implantation, and (3) with at least 1 outcome of interest measured numerically: speech perception, sound localization, device use, and patient-reported outcomes. Of the 526 articles reviewed, 12 (2.3%) met the selection criteria.
Data Extraction and Synthesis
The Meta-analyses Of Observational Studies in Epidemiology (MOOSE) reporting guidelines were followed. Data were pooled using fixed-effect and random-effect models. The following information was obtained from each article: study characteristics, patient characteristics, hearing loss and intervention characteristics, and outcomes.
Main Outcomes and Measures
Outcomes were (1) postoperative changes in speech perception (in quiet was measured as a proportion of correct responses, and in noise was measured as decibel signal to noise ratio for speech reception threshold) and sound localization (measured in degree of localization error), (2) patient-reported audiological outcomes (measured by the speech, spatial, and qualities of hearing scale), and (3) device use rates among children who received cochlear implantation for SSD.
Results
Twelve observational studies that evaluated 119 children (mean [SD] age, 6.6 [4.0] years) with SSD who received a cochlear implant were included. Most children showed clinically meaningful improvement in speech perception in noise (39 of 49 children [79.6%]) and in quiet (34 of 42 children [81.0%]). Long duration of deafness (>4 years in congenital SSD and >7 years in perilingual SSD) was the most commonly proposed reason for lack of improvement. Sound localization as measured by degrees of error from true location (mean difference [MD], –24.78°; 95% CI, –34.16° to –15.40°; I2 = 10%) improved statistically significantly after cochlear implantation. Patients with acquired SSD and shorter duration of deafness compared with those with congenital SSD reported greater improvements in speech (MD, 2.27; 95% CI, 1.89-2.65 vs 1.58; 95% CI, 1.00-2.16) and spatial (MD, 2.95; 95% CI, 2.66-3.24 vs 1.68; 95% CI, 0.96-2.39) hearing qualities. The duration of deafness among device nonusers was statistically significantly longer than the duration of deafness among regular device users (median difference, 6.84; 95% CI, 4.02-9.58).
Conclusions and Relevance
This systematic review and meta-analysis found that cochlear implantation for children with SSD was associated with clinically meaningful improvements in audiological and patient-reported outcomes; shorter duration of deafness may lead to better outcomes. These findings can guide future research efforts, refine cochlear implantation candidacy criteria, and aid in family counseling and shared decision-making.
Introduction
Sensorineural unilateral hearing loss (UHL) has an estimated incidence of 1 in 1000 live births in the United States.1,2 The prevalence increases to approximately 3% to 6.3% among children aged 6 to 19 years once delayed-onset congenital UHL and acquired causes accumulate.2,3,4
Children with single-sided deafness (SSD), the most severe form of UHL, often struggle with speech perception in noise and sound localization because of lack of binaural auditory input. This outcome has been associated with the absence of binaural hearing effects, such as the binaural squelch effect,5,6 the head shadow effect,7,8 and the binaural redundancy effect.9,10
Single-sided deafness has been shown to have implications for children’s speech-language development, cognition, and quality of life, placing them at an increased risk for psychosocial and behavioral difficulties and inferior functioning in educational settings compared with their peers with normal hearing.2,11,12,13
Until recently, standard clinical practice for auditory rehabilitation of children with SSD consisted of either observation alone, contralateral routing of signal hearing aids, or osseo-integrated hearing devices, all of which rely on routing of signals to the normal hearing ear. Although cochlear implantation for SSD has increased over the past several years, it has been mostly limited to adults and to off-label use for children in the US.14
In a historic step, in July 2019, the US Food and Drug Administration granted a first-time approval of cochlear implantation for SSD in children 5 years or older.15 The absence of robust clinical data to guide shared decision-making and to identify potential advantages represents a major challenge in the counseling of families of children with SSD. We performed this systematic review and meta-analysis to evaluate the audiological and patient-reported outcomes in children who underwent cochlear implantation for SSD and to assess the association between time of implantation, subjective outcomes, and cochlear implant use rates. We hypothesized that children with short duration of deafness prior to cochlear implantation would have improved audiological and patient-reported outcomes.
Methods
This systematic review and meta-analysis adhered to the Meta-analyses Of Observational Studies in Epidemiology (MOOSE) reporting guidelines (eTable 1 in the Supplement).16 The need for institutional review board approval was waived because of the Common Rule and because the study analyzed data exclusively from published literature. This study was conducted from January 4, 2020, to April 4, 2020.
Study Selection and Search Strategy
Inclusion criteria were studies that involved patients (1) younger than 18 years, (2) with a diagnosis of SSD for which they underwent a cochlear implantation, and (3) with at least 1 outcome of interest measured numerically: speech perception, sound localization, device use, and patient-reported outcomes. Speech perception in quiet was measured as a proportion of correct responses, and speech perception in noise was measured as decibel (dB) signal to noise ratio for speech reception threshold; sound localization was measured in degree of localization error; device use was measured by hours per day of device use; and patient-reported outcomes were measured by the speech, spatial, and qualities of hearing scale (SSQ). The SSQ is a validated standardized questionnaire that has been shown to be sensitive in measuring bilateral and unilateral hearing abilities across 3 domains, thus yielding 3 subscale scores (score range: 1-10, with the highest score indicating the best result).17,18 The SSQ has been validated for adults, children, and parent proxy for young children.17,18,19
The other 2 inclusion criteria were publication in a peer-reviewed journal and a study design that examined human participants. Only studies and patients who met the definition of SSD were deemed qualified for inclusion in this study. Single-sided deafness was defined as a 1-sided pure-tone average of 90 dB or higher or an auditory brain stem response of 80 or higher with normal hearing in the contralateral ear. Exclusion criteria included (1) studies that were not available in the English language, (2) studies in which pediatric data were not separable from adult data, (3) studies of cochlear implantation only for asymmetric hearing loss or partial deafness (residual hearing in low frequencies), and (4) single case reports.
A search of MEDLINE, Embase, Scopus, Cochrane, and PubMed databases was performed by a medical librarian for articles that were published from database inception to February 18, 2020. The terms SSD, cochlear implant, pediatric, and all of their synonyms were combined in the search strategy (the complete search strategy is outlined in the eMethods in the Supplement). After the initial search, duplicates were removed. Two of us (L.B., E.A.R.) independently screened the titles and abstracts of all potentially eligible articles and searched the bibliographies of each study to identify additional articles. Articles that appeared to meet eligibility criteria underwent a full-text screening. Selection criteria were applied, discrepancies in the article selection were resolved through discussion between the investigators, and a final list of studies was obtained. In case of overlapping cohorts, the most recent or comprehensive study was selected.
Data Extraction and Quality Assessment
One of us (L.B.) extracted data from the included articles, and another (E.A.R.) independently validated the data using standardized data forms. The following information was obtained from each article: study characteristics (design, period, location, and follow-up time), patient characteristics (number, implantation age, and sex), hearing loss and intervention characteristics (hearing loss cause, duration of deafness, preimplant pure-tone average or auditory brain stem response, and device type), and outcomes (speech perception in noise and quiet, sound localization, and daily device use). No attempt was made to contact the authors of studies with missing information. For studies that reported data in graph form only, the values were estimated with digitizing software (Engauge Digitizer, version 12.1; Mark Mitchell20).
The Newcastle-Ottawa Scale (NOS; score range: 1-9, with the highest score indicating lowest risk of bias)21 was completed independently by 2 of us (L.B., E.A.R.). Studies that received a score of less than 6 points were considered to have a high risk for bias, and the possibility of their exclusion was discussed by all authors (eTable 2 in the Supplement).
Statistical Analysis
Review Manager, version 5.3 (Cochrane),22 and Stata, version 15 (StataCorp LLC), were used to perform all of the analyses. Meta-analyses were conducted only when studies were comparable in terms of design and outcomes. If a meta-analysis was deemed inappropriate because of heterogeneous data or risk of bias, outcomes were evaluated at the individual study level through table and narrative review. Mean difference (MD) with 95% CIs was used for continuous data in studies that reported the same outcome measure and unit. In studies with median and range data only, we used an accepted method of estimating mean and SD.23 Depending on heterogeneity, either the fixed-effects or the random-effects model was applied to obtain pooled effect size estimates, 95% CIs, and P values through the inverse variance method.24 The I2 and χ2 statistics were used to evaluate the percentage variability of the results attributed to heterogeneity between studies.25 If substantial heterogeneity was denoted (χ2 P ≤ .10 or I2 > 50%), we used the random-effects model; otherwise, the fixed-effects model was applied. Daily device use was stratified as regular (>7 hours/d), limited (1-7 hours/d), or none (<1 hour/d). Data for the duration of deafness and implantation age were pooled in meta-analyses. The pooled data distribution was determined via the Kolmogorov-Smirnov test of normality. We used the independent unpaired, 2-tailed t test to compare means when normal distribution was identified and the Mann-Whitney test to compare medians in cases of non-normal distribution.
Results
The search strategy yielded 522 articles, of which 12 (2.3%) met the selection criteria for the systematic review (Figure 1). Six of these were included in the meta-analysis. Sound localization and patient-reported outcomes (through the SSQ) were amenable to a meta-analysis, whereas speech perception outcomes in noise and quiet were not based on high between-study heterogeneity. One study with 5 patients (1 of whom had UHL)26 and a patient from an included study27 were excluded because they did not meet the definition of SSD. All studies were case series with small sample sizes that ranged from 3 to 23 patients. The mean (SD) NOS score was 6.4 (0.9) (eTable 2 in the Supplement). For most studies, comparability points were deducted for lack of adjustments. Studies that scored 5 were still included because of the challenges with adjusting small cohorts and the valuable information obtained from each patient. Two pairs of studies28,29,30,31 had 1 to 2 overlapping patients. However, all 4 studies were included because each evaluated a different outcome of interest (eTable 3 in the Supplement).
Figure 1. Flow Diagram for Search and Study Selection Process.

AHL indicates asymmetric hearing loss; SSD, single-sided deafness.
Table 1 summarizes the characteristics of analyzed studies27,28,29,30,31,32,33,34,35,36,37,38 and patients. All 12 studies were observational cohort studies, collectively spanning more than a decade from 2004 to 2019. The studies were conducted in Europe (n = 8 [66.7%]), North America (3 [25.0%]), and Australia (1 [8.3%]). Overall, 119 children with a mean (SD) age of 6.6 (4.0) years were included, and most children (70 [58.8%]) had congenital SSD. The median (interquartile range [IQR]) duration of deafness was statistically significantly shorter in children with acquired SSD than in those with congenital SSD (1.3 [0.8-3.0] years vs 4.1 [1.7-6.9] years; median difference, 2.8; 95% CI, 1.08-4.52).
Table 1. Characteristics of Patients and Studies.
| Source | Location | Study period | No. of patients analyzed | Mean (SD) [range], y | Cause, No. | Preoperative PTA or ABR, mean (SD) [range], dBa | Device type, No. | Follow-up, mean (SD) [range], yb | ||
|---|---|---|---|---|---|---|---|---|---|---|
| Age at implantation | Duration of deafness | Poor ear | Good ear | |||||||
| Arndt et al,28 2015 | Freiburg, Germany | 2008-2014 | 14 (20 Total but 6 had no postoperative data) | 10.9 (3.7) [4.3-18] | 4.3 (4.0) [0.3-13.8] |
|
NA | NA |
|
1 |
| Beck et al,29 2017 | Freiburg, Germany | NA | 10 | 4.8 (3.5) [1.8-13.8] | 4.8 (3.5) [1.8-13.8] | Congenital: 4 CMV, 3 unknown, 1 hypoxia (?), 1 ototoxic med, 1 ANSD | ABR threshold: >90 | ABR: 21.1 (3.3) [20-30] | NA | 1.4 (1.1) [0.3-2.8] |
| Deep et al,27 2020 | New York, United States | 2011-2019 | 13 | 4.5 (2.8) [1-9.3] | 3.0 (2.2) [0.6-7] |
|
ABR: 108.1 (16.4) [90-125] | ABR: 15.1 (4.9) [10-25] |
|
3.4 (1.6) [1.2-6] |
| Ehrmann-Mueller et al,32 2020 | Wuerzburg, Germany | 2011-2013 | 7 | 8.6 (4.3) [3.6-16.3] | 7.7 (4.1) [3.8-16.3] | Congenital: 5 unknown, 1 CMV Acquired:1 trauma |
ABR: 100 | ABR: 10 | 7 MED-EL Concerto | 6.3 [5.3-7.8] |
| Ramos Macías et al,30 2016 | Gran Canaria, Spain | 2004-2011 | 2 (11 Total but 9 had AHL) | 4 (1) [3-5] | NA | Acquired: 2 unknown | NA | NA | 2 Nucleus AG | 1 |
| Ramos Macías et al,31 2019 | Gran Canaria, Spain | 2013-2016 | 23 | 7.2 (2.9) [0.9-11.2] | 1.3 (0.8) [0.5-4.1] |
|
NA | NA |
|
1 |
| Polonenko et al,33 2017 | Toronto, Canada | NA | 7 | 5.9 (5.9) [1.1-14.5] | 2.5 (1.1) [1.1-3.6] |
|
NA | NA | NA | 0.3 (0.4) |
| Rahne and Plontke,34 2016 | Halle, Germany | 2011-2014 | 4 (21 Total but 17 adults) | 8.3 (1.3) [7-10] | 6 (2.6) [1.5-8] |
|
ABR threshold: >90 | ABR: 10 (2.8) [6-14] |
|
0.08, 0.25, 0.5, 1 |
| Sangen et al,35 2019 | Leuven, Belgium | NA | 6 | 1.2 (0.5) [0.7-2.2] | 1.2 (0.5) [0.7-2.2] | Congenital: 4 CMV, 1 CN abnormality, 1 trauma | ABR threshold: ≥80 | ABR threshold: ≤35 | NA | 1.9 (1) [1-2.7] |
| Távora-Vieira and Rajan,36 2016 | Australia | NA | 3 | 4.2 (2.2) [1.4-6.8] | 4.2 (2.2) [1.4-6.8] | Congenital: 3 unknown | ABR threshold: >90 | ABR: 10 (5) [5-15] | 3 MED-EL OPUS 2 | 1, 2, 3 |
| Thomas et al,37 2017 | Bochum, Germany | 2012-2016 | 21 | 5.4 (3) [0.8-11.3] | 5.4 (3) [0.8-11.3] | 21 Congenital | NA | NA |
|
1.75 (1.25) [1.1-3.6] |
| Zeitler et al,38 2019 | Arizona, United States | 2011-2017 | 9 | 8.6 (3.8) [1.5-15.1] | 4.1 (3.1) [0.8-9.5] |
|
ABR:101.3 (15.1) [72.5-120] | ABR threshold: ≤25 |
|
1.1 (0.7) [0.25-2.3] |
Abbreviations: ABR, auditory brain stem response; AHL, asymmetric hearing loss; ANSD, auditory neuropathy spectrum disorder; CMV, cytomegalovirus; CN, cochlear nerve; EVA, enlarged vestibular aqueduct; NA, not available; PTA, pure-tone average; SHL, sudden hearing loss.
ABR is reported when PTA is not available.
Individual postoperative assessment times are reported when mean follow-up time is not available.
Audiological Outcomes
Speech Perception in Noise
Eight studies27,28,30,32,34,36,37,38 (66.7%) evaluated 49 children in total assessed speech perception in noise (Table 2). All studies presented background noise at 60 to 70 dB, and although various configurations were used, all studies measured the sound and noise from 0° azimuth (S0N0) testing configuration, and we reported these results for consistency. Among the 5 studies (involving 35 of 49 children [71.4%] in whom speech perception in noise was assessed) whose outcome was the change in dB signal to noise ratio for speech reception threshold, the mean improvement with the implant ranged from 0 dB to 2.7 dB. Among the remaining 3 studies whose outcome was the percentage of correct answers on word and sentence tests, the mean improvement with the implant ranged from 2.0% to 51.7%. Thirty-nine of 49 children (79.6%) experienced improved speech perception in noise after cochlear implantation.
Table 2. Audiological Outcomes.
| Source | Test conditions | No. of patients with available dataa | Outcome by postoperative time | Meaning and notesb | |
|---|---|---|---|---|---|
| Without cochlear implant | With cochlear implant | ||||
| Speech perception in noise (S0N0: speech and noise from front) | |||||
| Arndt et al,28 2015 (acquired) |
|
9 | −4.2 (1.2) dB |
|
Improvement was statistically significant in the speech deaf ear/noise NH ear condition only. |
| Arndt et al,28 2015 (congenital/perilingual) |
|
4 | −4.3 (0.6) dB |
|
No statistically significant improvement with device, which was attributed to long DD (>4 y) and CMV cause in congenital SSD (n = 2) and long DD (>7 y) in perilingual SSD. |
| Rahne and Plontke,34 2016 |
|
4 | −2.7 (1.5) dB |
|
Improvement with device in all children; subjective advantage also reported. |
| Thomas et al,37 2017 |
|
14 |
|
|
Statistically significant improvement with implant; no statistically significant difference between implantation age of <6 y and >6 y. 9 Children (64%) had greater than 1.5 dB difference in noise-speech perception. |
| Deep et al,27 2020 |
|
5 |
|
|
No statistically significant improvement with implant, which was explained by excellent performance of acoustic ear alone, creating a ceiling effect in detecting a meaningful difference with binaural hearing. |
| Ehrman-Mueller et al,32 2020 |
|
7 |
|
|
Statistically significant improvement with implant among all children, although widely variable. No clear association between outcomes and hearing loss cause, DD, or implantation age was observed. |
| Ramos Macías et al,30 2016 |
|
2 | 15.8 (2.8) dB |
|
Both children with acquired perilingual/postlingual HL improved postimplantation, which was attributed to DD <3 y. |
| Távora-Vieira and Rajan,36 2016 |
|
1 | −5.5 dB |
|
No difference with implant, which was attributed to long DD of 6.8 y. |
| Zeitler et al,38 2019 |
|
3 | NA |
|
Improvement with implant in all children. |
| Speech perception in quiet (implant ear–only condition) | |||||
| Deep et al,27 2020 |
|
6 | 9.3 (13.9%) |
|
Improvement with cochlear implant in all children. Children with shorter DD (1.1-3 y) had greater improvement (>40%) than children with longer DD (3-7 y). |
| Zeitler et al,38 2019 |
|
6 | 17.8 (11.3%) |
|
Improvement with cochlear implant in all children. Because of small sample size, association of DD and deafness cause with % improvement could not be determined. |
| Beck et al,29 2017 |
|
7 | NA | 34.3 (36.6%)c | Patients receiving implantation at younger age (1.8-3.2 y; n = 3) had better outcomes than those at older age (4-13.8 y; n = 4). All had congenital SSD. |
| Rahne and Plontke,34 2016 |
|
4 |
|
|
1 Child improved with cochlear implant over time (DD 1.5 y); 3 children did not improve over time (DD 7-8 y); 1 child had radiologically hypoplastic CN, and 1 had questionable patency of CN. They still received implantation because all children reported a positive response after electrical stimulation of the promontory. |
| Ramos Macías et al,31 2019 |
|
17 | NA |
|
All children had scores ≥48% in implant ear–only condition, and ≥92% in binaural condition (no masking). |
| Távora-Vieira and Rajan,36 2016 |
|
2 | NA |
|
Cochlear implant was advantageous only in the child with shorter (1.4 y) DD but not in the child with longer (6.8 y) DD-auditory stimulations perceived as vibration only. |
| Sound localization | |||||
| Ehrman-Mueller et al,32 2020 |
|
4-6 |
|
|
Improvement with cochlear implant in all children, although it did not reach statistical significance. All parents reported observing improved localization abilities, especially in road traffic. |
| Ramos Macías et al,31 2019 |
|
23 | Negative result in all conditions in all children |
|
|
| Thomas et al,37 2017 |
|
14 |
|
|
Statistically significant improvement with cochlear implant when stimuli presented at −90° (NH ear) and +90° (cochlear implant ear) but not from front (0°). |
Abbreviations: AZBio, Arizona Biomedical Institute Sentence Test; BKB-SIN, Bamford-Kowal-Bench Speech in Noise test; CMV, cytomegalovirus; CN, cochlear nerve; dB, decibel; DD, duration of deafness; HINT, hearing in noise test; NH, normal hearing; NU-CHIPS, Northwestern University-Children's Perception of Speech; OlSa, Oldenberg Sentence Test; RMS, root mean square; SNR, signal to noise ratio; SRT, speech reception threshold; SSD, single-sided deafness; WRS, word recognition score.
The number of patients may be smaller than total patients in each study as only those with available outcomes are reported.
Statistical significance pertains to the significance reported in each source study.
Postoperative time was not available.
Overall, 530,32,34,37,38 of the 8 studies (with 30 of 49 children [61.2%]) that assessed speech perception in noise reported a clinically meaningful improvement with the implant among all patients. Two of these studies32,37 (21 of 49 children [42.8%]) calculated and identified a statistically significant improvement. The remaining 3 studies27,28,36 evaluated 19 children (38.8%). Arndt et al,28 who consistently stratified the results by congenital or perilingual vs acquired (postlingual) SSD, did not report a clinically or statistically meaningful difference of sound perception in noise in the S0N0 testing condition among children (n = 9) with acquired SSD. They did report a clinically and statistically meaningful improvement in the speech deaf ear, noise normal hearing ear testing condition.28 Arndt et al28 attributed the lack of improvement in the 4 children with congenital or perilingual SSD to long duration of deafness (>4 years in congenital SSD; >7 years in perilingual SSD) and cytomegalovirus (CMV) deafness cause. Deep et al27 evaluated 5 children and attributed the lack of improvement to a ceiling effect created by the excellent normal hearing ear. Távora-Vieira and Rajan36 evaluated 1 child and attributed the lack of improvement to the long duration of deafness (>6.8 years), which included the critical period for binaural hearing development. Among these 3 studies, long duration of deafness was cited as the reason for the lack of improvement in 5 of the 10 (50%) children in whom no clinical or statistical improvement was noted.
Speech Perception in Quiet
Six studies27,29,31,34,36,38 of 42 children, assessed speech perception in quiet in the implant ear–only (masking of normal hearing ear) (Table 2). The outcome in all studies was the proportion of correct answers. Six unique age-appropriate sentence tests and monosyllabic or multisyllabic word tests were used: Arizona Biomedical Institute Sentence Test,38 consonant-vowel nucleus-consonant word test,27,36,38 Freiburger Speech Test,34 Lexical Neighborhood Test,27,38 Mainzer speech perception test,34 and the Northwestern University-Children’s Perception of Speech.36
The mean scores achieved with the implant ranged from 0% to 100%. Overall, 34 children (81.0%) experienced improvement from the cochlear implantation, and their mean scores ranged from 56% to 100%. Three27,31,38 of the 6 studies, evaluating 29 children (69.0%), reported an implant-associated change for all children. For example, Deep et al27 noted that children who received an implant after a shorter duration of deafness (3 years) had greater improvement than children who underwent an implantation later. The remaining 3 studies29,34,36 (evaluating 13 children [30.2%]) reported postimplantation advantages in 5 children. For the remaining 7 children (16.7%), the authors cited long duration of deafness (>4 years,29,34 >7 years,34 and >6.8 years36) as the probable reason for lack of observed improvement. None of the studies conducted a statistical analysis for speech perception in quiet outcome.
Sound Localization
Sound localization was assessed in 6 studies.28,31,32,34,36,37 Researchers used between 3 to 13 loudspeakers, with various stimuli presented at 55 to 70 dB. Three of the studies28,34,36 used the root-mean-square (RMS) localization error as the outcome unit to assess preoperative vs postoperative (1-2.2 years) binaural performance and were combined for a meta-analysis (Figure 2). Device use was associated with decreased RMS error and improved sound localization (MD, –24.78°; 95% CI, –34.16° to –15.40°). Heterogeneity was not substantial (I2 = 10%; P = .36), and a fixed-effects model was used. Results of 3 studies31,32,37 with data incompatible for meta-analysis are summarized in Table 2. Most children in these studies (n = 55 of 62 [88.7%]) showed improvement in sound localization 1 to 2 years after cochlear implantation, with mean reduction of 24.78° in localization error. All studies reported clinical improvement of sound localization at most angles.
Figure 2. Meta-analysis Forest Plots of Mean Differences for Sound Localization .
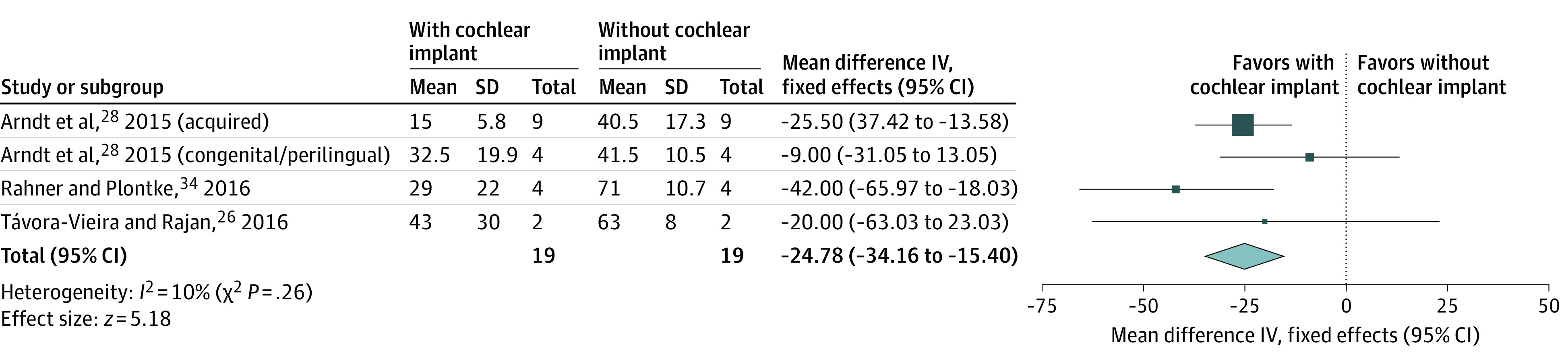
Root-mean-square localization error is the outcome unit. Results of Arndt et al28 are stratified according to the original article reporting. Boxes indicate relative sample size; diamonds, overall mean difference; IV, inverse variance model; and horizontal lines, 95% CIs.
Patient-Reported Outcomes
Four studies28,29,31,37 used the SSQ as a patient-reported auditory questionnaire. The questionnaire items were scored from 1 to 10, completed before and after (1-3 years) cochlear implantation, and combined in a meta-analysis (Figure 3). The outcomes were divided into congenital vs acquired SSD and are presented herein accordingly. Cochlear implantation was associated with statistically significant improvements in all 3 domains (speech hearing, spatial hearing, and hearing quality). Children with acquired SSD had statistically significantly greater improvements compared with children with congenital SSD in the speech (MD, 2.27; 95% CI, 1.89-2.65 vs 1.58; 95% CI, 1.00-2.16) (Figure 3A) and spatial (MD, 2.95; 95% CI, 2.66-3.24 vs 1.68; 95% CI, 0.96-2.39) (Figure 3B) hearing domains. The mean (SD) implantation age of children with congenital SSD was statistically significantly younger than the implantation age of children with acquired SSD (5.1 [3.2] years vs 9.5 [3.0] years; MD, 3.39; 95% CI, 1.41-7.39). The median (IQR) duration of deafness, however, was statistically significantly shorter in the acquired SSD group vs the congenital SSD group (1 [0.8-1.5] years vs 4.1 [1.7-6.8] years; median difference, 3.11; 95% CI, 1.29-3.91). Hearing quality scores (Figure 3C) had high heterogeneity (congenital I2 = 81% vs acquired I2 = 88%), even though the same SSQ questionnaire and same studies were used for the speech (Figure 3A) and spatial (Figure 3B) subscale categories. Given the low heterogeneity in the other 2 subscale categories, low risk of bias in all studies (NOS score ≥6), and no other justified reason to remove this part of the questionnaire, we retained this analysis.
Figure 3. Meta-analysis Forest Plots of Mean Differences in Scores on Speech, Spatial, and Qualities (SSQ) of Hearing Stratified by Congenital vs Acquired Single-Sided Deafness .
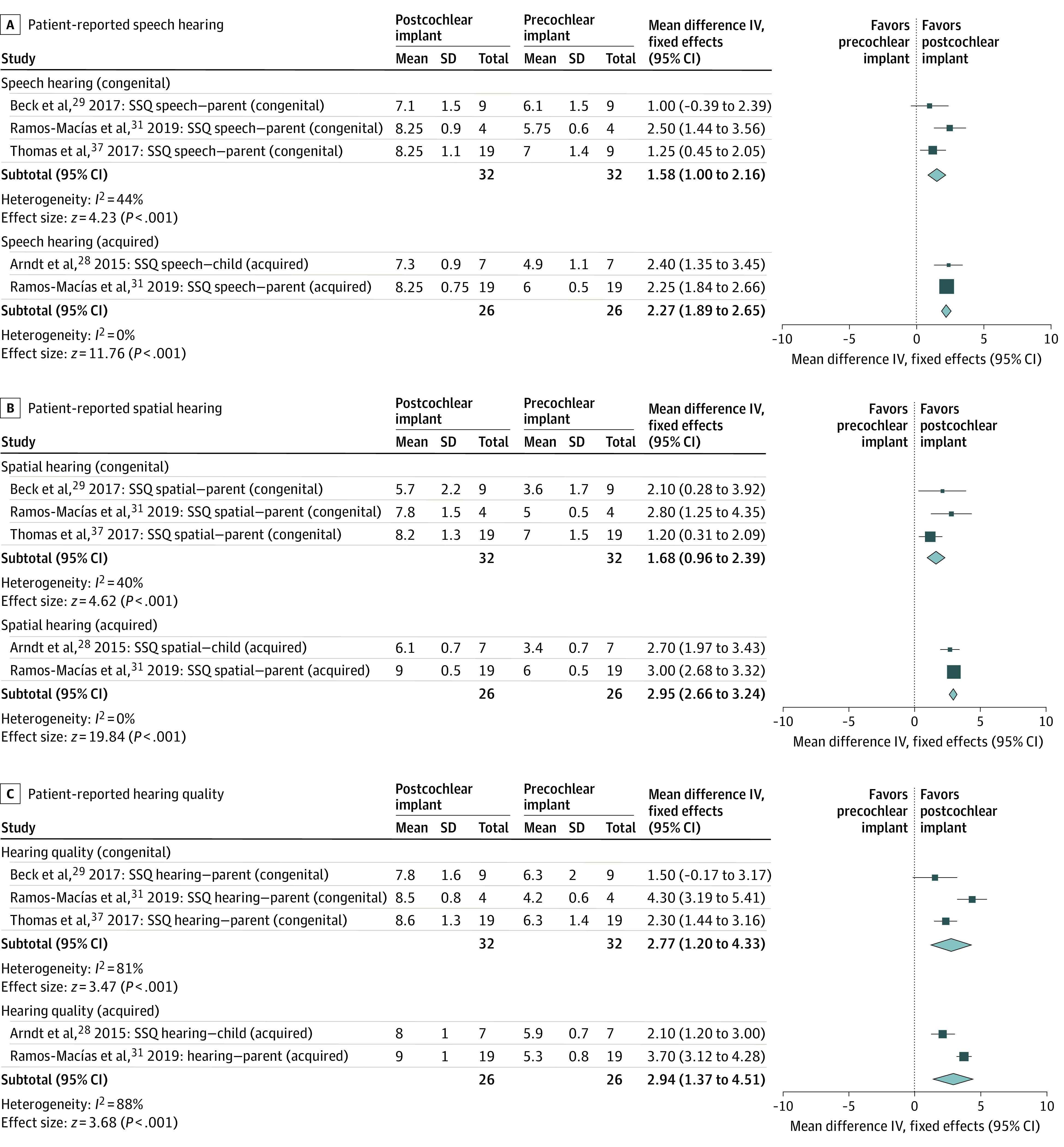
Boxes indicate relative sample size; diamonds, overall mean difference; IV, inverse variance model; and horizontal lines, 95% CIs.
Device Use and Duration of Deafness
Eleven studies27,28,29,31,32,35,36,37,38,39,40 reported on both the duration of deafness and the frequency of device use after a median (IQR) follow-up of 1.6 (1-2.1) years. To capture device use, 3 of the studies27,33,35 reported device data logging (n = 36). Of 101 children, most (75 [74.3%]) used the device regularly. The remaining 21 children (20.8%) reported limited device use, and 5 (4.9%) became nonusers. Nonuse was explained by the lack of advantage (n = 3),28,37,38 unpleasant electrical stimulation (n = 1),36 and lack of adequate family support (n = 1).27 The median (IQR) duration of deafness among nonusers was statistically significantly longer than the duration of deafness of limited users (9.0 [5.8-11.7] years vs 3.3 [1.2-5.4] years; median difference, 5.75; 95% CI, 2.45-9.05) and regular users (9.0 [5.8-11.7] years vs 2.2 [1.1-5.3] years; median difference, 6.84; 95% CI, 4.02-9.58) (eFigure in the Supplement). The mean (SD) implantation age of nonusers was statistically significantly older than the implantation age of limited users (9.3 [3.3] years vs 4.1 [3.4] years; MD, 5.21; 95% CI, 1.70-8.70) and regular users (9.3 [3.3] years vs 6.0 [3.4] years; MD, 3.26; 95% CI, 0.18-6.42).
Discussion
Cochlear implantation for children with SSD has been performed worldwide for several years. However, comprehensive clinical data that evaluate the outcomes are scant. Only 1 systematic review of 5 studies41 and 1 nonsystematic review42 are available in the literature and both were published before the 2019 Food and Drug Administration approval for this indication in the US.15
Results of the present systematic review show that most children (79.6%) experienced improved speech perception in noise after cochlear implantation, which was clinically meaningful according to the study authors.27,28,30,32,34,36,37,38 Two studies,28,29,30,31,32,34,36,37 however, emphasized the lack of improvement among children with congenital SSD who received an implant after age 4 years. In addition, these studies reported a high prevalence of CMV-related SSD, which was possibly a factor in inferior outcomes.28,37,43,44,45 The heterogeneity of demographic and clinical factors within small cohorts may have also had implications for the outcomes, as suggested by Deep et al.27
In this review, 4 studies26,27,31,38 reported implant-associated changes for most children, such as higher scores in speech perception in quiet, whereas 3 studies29,34,36 indicated that only children with shorter duration of deafness (<4-7 years) acquired a clinically significant speech recognition improvement after implantation. Shorter duration of deafness in the ear without an implant was recognized as advantageous in a previous multicenter clinical trial by Peters et al,46 which found that, among children who underwent sequential bilateral cochlear implants, the duration of less than 4 years in between implants was associated with faster and greater degree of improvements in speech perception in quiet. Studies of sequential bilateral cochlear implants in children reported mean preoperative speech perception in quiet outcome of 0% to 17% with monaural hearing aid–only condition, increasing to mean speech perception in quiet outcome of 40% to 100% after 3 months to 1 year of a second implant.46,47 The studies in this review reported that the cochlear implantation–only condition mean preoperative speech perception in quiet scores were between 0% to 36%,27,38 increasing to mean postoperative speech perception in quiet scores of 30% to 100%.26,27,29,31,36,38 The comparability in the cochlear implantation–only speech perception in quiet outcome between children with SSD and conventional cochlear implantation candidates suggests that the presence of normal hearing in the contralateral ear (either after the implant normalizing hearing thresholds in 1 ear or in the setting of SSD) did not impair the performance of the device. This finding is contrary to those in some adult studies, which suggest that cochlear implantation for people with SSD is associated with inferior performance in the cochlear implant–only condition.48,49
Most children (55 of 62 children [88.7%] in whom sound localization was assessed) also showed improvement in sound localization 1 to 2 years after cochlear implantation. Although not all studies reached individual statistical significance, largely owing to their small sample size, the present meta-analysis detected a clinically and statistically significant improvement. We identified a statistically significant decrease of 24.78° in RMS localization error, with postimplantation means that ranged from 15° to 43° RMS, which was comparable to the RMS in children with bilateral implants.50 Evaluating 127 children with bilateral implants, Killan et al50 identified shorter interimplant interval, later deafness onset, prolonged experience with 2 devices, and a MED-EL device as statistically significantly associated with superior localization abilities. Although the small sample size in the present study precluded us from performing a similar linear regression analysis as that in the Killan et al50 study, it is possible that 1 or more of the factors they found had implications for the wide range of localization abilities.
Four studies evaluated patient-reported outcomes with the SSQ questionnaire. Caregivers filled out the questionnaire in 3 studies,29,31,37 and children filled it out in 1 study.28
Results of this study suggest that children with congenital SSD had inferior results on patient-reported auditory performance questionnaires compared with children with acquired SSD. In addition, among those who completed the SSQ questionnaire, patients with acquired SSD had substantially shorter duration of deafness than those with congenital SSD, suggesting that longer duration of deafness may be associated with the worse patient-reported outcomes in the congenital SSD group. Early auditory stimulation is important in the development and maturation of the auditory cortex; with lack of appropriate stimulation, children with long duration of congenital deafness show abnormal cortical response latencies when they undergo cochlear implantation.51,52 Patients with acquired hearing loss likely have shorter duration of hearing loss and more timely intervention compared with patients with congenital hearing loss.28,31 Subsequently, with known worse implant performance in long-standing untreated congenital hearing loss, it is not too surprising that patients with acquired hearing loss performed better on auditory performance questionnaires in the studies we reviewed. As a correlate, results of this study show that children with longer duration of deafness were more likely to be nonusers of implants. Because longer duration of deafness was associated with inferior outcomes, children likely perceived less value, which may have been a factor in nonuse. Half of the nonusers in this review cited the lack of improvement as a reason for not using their device.
An overarching theme suggested by these findings is that shorter duration of deafness, ranging from less than 4 to 7 years, is associated with greater postimplantation improvement in both audiological and patient-reported outcomes in children with SSD. These findings are comparable to results in children with bilateral congenital deafness. Ample data and an overall agreement support that children with bilateral congenital deafness gain the most advantage when cochlear implantation occurs within a sensitive period of central auditory development, during which auditory neuronal pathways are at maximal plasticity.53,54 Cortical auditory responses were shown to reach normal range in children who received an implant before age 3.5 years, and abnormal responses were observed in children who received an implant after age 7 years, even after long-term implant use.53,55,56,57,58 These electrophysiological findings also correlate with speech and language performance studies that found children who underwent cochlear implantation before age 3 to 4 years, or those with shorter duration of deafness, achieved substantially better speech perception scores and language skills vs children who received an implant after age 5 to 7 years.59,60,61,62
However, data on the association of implantation age and duration of deafness with auditory pathway reorganization, as well as with audiological outcomes, after cochlear implantation in children with unilateral hearing loss are limited and inconclusive. Polonenko et al39 identified restored cortical organization after implantation, and 6 months of device use, before age 3.6 years in 5 children with CMV- and enlarged vestibular aqueduct–related SSD. Sharma et al63 also reported cortical reorganization in a child with progressive idiopathic SSD from age 5 who underwent cochlear implantation at age 9.86 years. These authors39,63 hypothesized that either the patient’s prior experience with sound in the deaf ear (owing to the progressive nature of the hearing loss) or stimulation through crossed pathways from the normal hearing ear would explain the favorable results at this late age. Neither of these 2 studies offered definitive conclusions regarding the optimal age or duration of deafness for implantation.
A 2018 systematic review of 8 studies that included 78 adults with postlingual SSD concluded that longer duration of deafness had a substantial negative correlation with speech perception outcomes.64 Although a lack of postimplantation improvement after 10 years of deafness was witnessed, only 5 patients were followed for that length of time, and the authors concluded that no specific time cutoffs for cochlear implantation could be inferred.64 The present study emphasizes the need for more robust research that seeks to identify the optimal cochlear implantation age and the duration of deafness that could prohibit favorable outcomes in children with SSD.
Limitations
This study has limitations. It selected studies with small sample sizes. It also was unable to control for the heterogeneity of the pediatric SSD population, including deafness cause, onset and duration, age at implantation, device manufacturers, and extent and availability of social and rehabilitative support systems. The limitations of the quantitative syntheses included the use of study-level data when individual patient data were not available. The use of variable tests and configurations to evaluate audiological outcomes suggests further between-study heterogeneity. However, only studies with comparable outcomes and design were included in the meta-analysis. This approach, although not free from pitfalls, allowed a clearer result interpretation than could be achieved with a qualitative review and was used in previous meta-analyses of adults with hearing loss.65,66 In addition, previous works have suggested that, other than duration of deafness and implantation timing (which are 2 of the most important outcome determinants in pediatric cochlear implant recipients62,67,68), comorbid conditions, such as inner ear malformations and genetic mutations, have implications for the outcomes.69,70,71,72 Unfortunately, inconsistent reporting of comorbidities and their direct association with outcomes and device use rates in the studies that we examined precluded us from offering a comorbidity analysis. With sufficient sample size, this topic should be analyzed in future research on the cochlear implant SSD pediatric population.
Conclusions
This systematic review and meta-analysis found that, among children with SSD, cochlear implantation was associated with improved objective and subjective auditory outcomes. Children with acquired SSD and shorter durations of deafness, however, reported experiencing greater advantages and were less likely to become nonusers of implant devices. These results can be used to guide research efforts, refine cochlear implantation candidacy criteria, and aid in family counseling and shared decision-making. The heterogeneity and small sample sizes of the included studies emphasize the need for robust clinical studies.
eTable 1. MOOSE (Meta-analyses Of Observational Studies in Epidemiology) Checklist
eTable 2. Newcastle-Ottawa Scale for Quality Assessment of Nonrandomized Studies in Meta-Analyses
eTable 3. Reasons for Article Exclusions Following Full-Text Review
eMethods. Complete Search Strategy
eFigure. Box Plot Comparison of Median and Interquartile Ranges of Duration of Deafness Between CI Usage Groups
eReferences
References
- 1.Barsky-Firkser L, Sun S. Universal newborn hearing screenings: a three-year experience. Pediatrics. 1997;99(6):E4. doi: 10.1542/peds.99.6.e4 [DOI] [PubMed] [Google Scholar]
- 2.Lieu JEC. Permanent unilateral hearing loss (UHL) and childhood development. Curr Otorhinolaryngol Rep. 2018;6(1):74-81. doi: 10.1007/s40136-018-0185-5 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 3.Ross DS, Visser SN, Holstrum WJ, Qin T, Kenneson A. Highly variable population-based prevalence rates of unilateral hearing loss after the application of common case definitions. Ear Hear. 2010;31(1):126-133. doi: 10.1097/AUD.0b013e3181bb69db [DOI] [PubMed] [Google Scholar]
- 4.Shargorodsky J, Curhan SG, Curhan GC, Eavey R. Change in prevalence of hearing loss in US adolescents. JAMA. 2010;304(7):772-778. doi: 10.1001/jama.2010.1124 [DOI] [PubMed] [Google Scholar]
- 5.Ma N, Morris S, Kitterick PT. Benefits to speech perception in noise from the binaural integration of electric and acoustic signals in simulated unilateral deafness. Ear Hear. 2016;37(3):248-259. doi: 10.1097/AUD.0000000000000252 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 6.Akeroyd MA. The psychoacoustics of binaural hearing. Int J Audiol. 2006;45(suppl 1):S25-S33. doi: 10.1080/14992020600782626 [DOI] [PubMed] [Google Scholar]
- 7.Van Wanrooij MM, Van Opstal AJ. Contribution of head shadow and pinna cues to chronic monaural sound localization. J Neurosci. 2004;24(17):4163-4171. doi: 10.1523/JNEUROSCI.0048-04.2004 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 8.Brungart DS, Rabinowitz WM. Auditory localization of nearby sources. Head-related transfer functions. J Acoust Soc Am. 1999;106(3, pt 1):1465-1479. doi: 10.1121/1.427180 [DOI] [PubMed] [Google Scholar]
- 9.Bronkhorst AW, Plomp R. The effect of head-induced interaural time and level differences on speech intelligibility in noise. J Acoust Soc Am. 1988;83(4):1508-1516. doi: 10.1121/1.395906 [DOI] [PubMed] [Google Scholar]
- 10.Dunn CC, Tyler RS, Oakley S, Gantz BJ, Noble W. Comparison of speech recognition and localization performance in bilateral and unilateral cochlear implant users matched on duration of deafness and age at implantation. Ear Hear. 2008;29(3):352-359. doi: 10.1097/AUD.0b013e318167b870 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 11.Lieu JE. Unilateral hearing loss in children: speech-language and school performance. B-ENT. 2013;(suppl 21):107-115. [PMC free article] [PubMed] [Google Scholar]
- 12.Lieu JE, Tye-Murray N, Fu Q. Longitudinal study of children with unilateral hearing loss. Laryngoscope. 2012;122(9):2088-2095. doi: 10.1002/lary.23454 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 13.Anne S, Lieu JEC, Cohen MS. Speech and language consequences of unilateral hearing loss: a systematic review. Otolaryngol Head Neck Surg. 2017;157(4):572-579. doi: 10.1177/0194599817726326 [DOI] [PubMed] [Google Scholar]
- 14.Zeitler DM, Dorman MF. Cochlear implantation for single-sided deafness: a new treatment paradigm. J Neurol Surg B Skull Base. 2019;80(2):178-186. doi: 10.1055/s-0038-1677482 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 15.MED-EL USA FDA approves MED-EL USA’s cochlear implants for single-sided deafness and asymmetric hearing loss. Press release. Published July 22, 2019. Accessed January 20, 2020. https://s3.medel.com/downloadmanager/downloads/us_research/en-US/SSD+FDA+Approval+Press+Release_FINAL_7.22.19.pdf
- 16.Stroup DF, Berlin JA, Morton SC, et al. Meta-analysis of observational studies in epidemiology: a proposal for reporting. Meta-analysis Of Observational Studies in Epidemiology (MOOSE) group. JAMA. 2000;283(15):2008-2012. doi: 10.1001/jama.283.15.2008 [DOI] [PubMed] [Google Scholar]
- 17.Gatehouse S, Noble W. The Speech, Spatial and Qualities of Hearing Scale (SSQ). Int J Audiol. 2004;43(2):85-99. doi: 10.1080/14992020400050014 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 18.Galvin KL, Mok M, Dowell RC. Perceptual benefit and functional outcomes for children using sequential bilateral cochlear implants. Ear Hear. 2007;28(4):470-482. doi: 10.1097/AUD.0b013e31806dc194 [DOI] [PubMed] [Google Scholar]
- 19.Sanderson G, Ariyaratne TV, Wyss J, Looi V. A global patient outcomes registry: cochlear paediatric implanted recipient observational study (Cochlear(™) P-IROS). BMC Ear Nose Throat Disord. 2014;14:10. doi: 10.1186/1472-6815-14-10 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 20.Engauge Digitizer Version 12.1. Accessed March 3, 2020. http://markummitchell.github.io/engauge-digitizer
- 21.Wells GA, Shea B, O’Connell DPJ, Welch V, Losos MTP The Newcastle–Ottawa Scale (NOS) for assessing the quality of nonrandomised studies in meta-analyses. Published 2014. Accessed January 3, 2019. http://www.ohri.ca/programs/clinical_epidemiology/oxford.asp
- 22.Review Manager (RevMan) Version 5.3. Cochrane; 2014. Accessed February 20, 2020. https://training.cochrane.org/online-learning/core-software-cochrane-reviews/revman/revman-5-download
- 23.Hozo SP, Djulbegovic B, Hozo I. Estimating the mean and variance from the median, range, and the size of a sample. BMC Med Res Methodol. 2005;5:13. doi: 10.1186/1471-2288-5-13 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 24.Higgins JP, Thompson SG, Deeks JJ, Altman DG. Measuring inconsistency in meta-analyses. BMJ. 2003;327(7414):557-560. doi: 10.1136/bmj.327.7414.557 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 25.Higgins JP, Thompson SG. Quantifying heterogeneity in a meta-analysis. Stat Med. 2002;21(11):1539-1558. doi: 10.1002/sim.1186 [DOI] [PubMed] [Google Scholar]
- 26.Greaver L, Eskridge H, Teagle HFB. Considerations for pediatric cochlear implant recipients with unilateral or asymmetric hearing loss: assessment, device fitting, and habilitation. Am J Audiol. 2017;26(2):91-98. doi: 10.1044/2016_AJA-16-0051 [DOI] [PubMed] [Google Scholar]
- 27.Deep NL, Gordon SA, Shapiro WH, Waltzman SB, Roland JT Jr, Friedmann DR. Cochlear implantation in children with single-sided deafness. Laryngoscope. 2020. doi: 10.1002/lary.28561 [DOI] [PubMed] [Google Scholar]
- 28.Arndt S, Prosse S, Laszig R, Wesarg T, Aschendorff A, Hassepass F. Cochlear implantation in children with single-sided deafness: does aetiology and duration of deafness matter? Audiol Neurootol. 2015;20(suppl 1):21-30. doi: 10.1159/000380744 [DOI] [PubMed] [Google Scholar]
- 29.Beck RL, Aschendorff A, Hassepaß F, et al. Cochlear implantation in children with congenital unilateral deafness: a case series. Otol Neurotol. 2017;38(10):e570-e576. doi: 10.1097/MAO.0000000000001597 [DOI] [PubMed] [Google Scholar]
- 30.Ramos Macías Á, Borkoski-Barreiro SA, Falcón González JC, Ramos de Miguel Á. AHL, SSD and bimodal CI results in children. Eur Ann Otorhinolaryngol Head Neck Dis. 2016;133(suppl 1):S15-S20. doi: 10.1016/j.anorl.2016.04.017 [DOI] [PubMed] [Google Scholar]
- 31.Ramos Macías Á, Borkoski-Barreiro SA, Falcón González JC, de Miguel Martínez I, Ramos de Miguel Á. Single-sided deafness and cochlear implantation in congenital and acquired hearing loss in children. Clin Otolaryngol. 2019;44(2):138-143. doi: 10.1111/coa.13245 [DOI] [PubMed] [Google Scholar]
- 32.Ehrmann-Mueller D, Kurz A, Kuehn H, et al. Usefulness of cochlear implantation in children with single sided deafness. Int J Pediatr Otorhinolaryngol. 2020;130:109808. doi: 10.1016/j.ijporl.2019.109808 [DOI] [PubMed] [Google Scholar]
- 33.Polonenko MJ, Papsin BC, Gordon KA. Children with single-sided deafness use their cochlear implant. Ear Hear. 2017;38(6):681-689. doi: 10.1097/AUD.0000000000000452 [DOI] [PubMed] [Google Scholar]
- 34.Rahne T, Plontke SK. Functional result after cochlear implantation in children and adults with single-sided deafness. Otol Neurotol. 2016;37(9):e332-e340. doi: 10.1097/MAO.0000000000000971 [DOI] [PubMed] [Google Scholar]
- 35.Sangen A, Dierckx A, Boudewyns A, et al. Longitudinal linguistic outcomes of toddlers with congenital single-sided deafness—six with and twelve without cochlear implant and nineteen normal hearing peers. Clin Otolaryngol. 2019;44(4):671-676. doi: 10.1111/coa.13347 [DOI] [PubMed] [Google Scholar]
- 36.Távora-Vieira D, Rajan GP. Cochlear implantation in children with congenital unilateral deafness: mid-term follow-up outcomes. Eur Ann Otorhinolaryngol Head Neck Dis. 2016;133(suppl 1):S12-S14. doi: 10.1016/j.anorl.2016.04.016 [DOI] [PubMed] [Google Scholar]
- 37.Thomas JP, Neumann K, Dazert S, Voelter C. Cochlear implantation in children with congenital single-sided deafness. Otol Neurotol. 2017;38(4):496-503. doi: 10.1097/MAO.0000000000001343 [DOI] [PubMed] [Google Scholar]
- 38.Zeitler DM, Sladen DP, DeJong MD, Torres JH, Dorman MF, Carlson ML. Cochlear implantation for single-sided deafness in children and adolescents. Int J Pediatr Otorhinolaryngol. 2019;118:128-133. doi: 10.1016/j.ijporl.2018.12.037 [DOI] [PubMed] [Google Scholar]
- 39.Polonenko MJ, Gordon KA, Cushing SL, Papsin BC. Cortical organization restored by cochlear implantation in young children with single sided deafness. Sci Rep. 2017;7(1):16900. doi: 10.1038/s41598-017-17129-z [DOI] [PMC free article] [PubMed] [Google Scholar]
- 40.Sangen A, Royackers L, Desloovere C, Wouters J, van Wieringen A. Single-sided deafness affects language and auditory development - a case-control study. Clin Otolaryngol. 2017;42(5):979-987. doi: 10.1111/coa.12826 [DOI] [PubMed] [Google Scholar]
- 41.Peters JP, Ramakers GG, Smit AL, Grolman W. Cochlear implantation in children with unilateral hearing loss: a systematic review. Laryngoscope. 2016;126(3):713-721. doi: 10.1002/lary.25568 [DOI] [PubMed] [Google Scholar]
- 42.Boyd PJ. Potential benefits from cochlear implantation of children with unilateral hearing loss. Cochlear Implants Int. 2015;16(3):121-136. doi: 10.1179/1754762814Y.0000000100 [DOI] [PubMed] [Google Scholar]
- 43.Shin JJ, Keamy DG Jr, Steinberg EA. Medical and surgical interventions for hearing loss associated with congenital cytomegalovirus: a systematic review. Otolaryngol Head Neck Surg. 2011;144(5):662-675. doi: 10.1177/0194599811399241 [DOI] [PubMed] [Google Scholar]
- 44.Yoshida H, Takahashi H, Kanda Y, Kitaoka K, Hara M. Long-term outcomes of cochlear implantation in children with congenital cytomegalovirus infection. Otol Neurotol. 2017;38(7):e190-e194. doi: 10.1097/MAO.0000000000001483 [DOI] [PubMed] [Google Scholar]
- 45.Ciorba A, Bovo R, Trevisi P, Bianchini C, Arboretti R, Martini A. Rehabilitation and outcome of severe profound deafness in a group of 16 infants affected by congenital cytomegalovirus infection. Eur Arch Otorhinolaryngol. 2009;266(10):1539-1546. doi: 10.1007/s00405-009-0944-5 [DOI] [PubMed] [Google Scholar]
- 46.Peters BR, Litovsky R, Parkinson A, Lake J. Importance of age and postimplantation experience on speech perception measures in children with sequential bilateral cochlear implants. Otol Neurotol. 2007;28(5):649-657. doi: 10.1097/01.mao.0000281807.89938.60 [DOI] [PubMed] [Google Scholar]
- 47.Zeitler DM, Kessler MA, Terushkin V, et al. Speech perception benefits of sequential bilateral cochlear implantation in children and adults: a retrospective analysis. Otol Neurotol. 2008;29(3):314-325. doi: 10.1097/MAO.0b013e3181662cb5 [DOI] [PubMed] [Google Scholar]
- 48.Finke M, Strauß-Schier A, Kludt E, Büchner A, Illg A. Speech intelligibility and subjective benefit in single-sided deaf adults after cochlear implantation. Hear Res. 2017;348:112-119. doi: 10.1016/j.heares.2017.03.002 [DOI] [PubMed] [Google Scholar]
- 49.Sladen DP, Frisch CD, Carlson ML, Driscoll CLW, Torres JH, Zeitler DM. Cochlear implantation for single-sided deafness: a multicenter study. Laryngoscope. 2017;127(1):223-228. doi: 10.1002/lary.26102 [DOI] [PubMed] [Google Scholar]
- 50.Killan C, Scally A, Killan E, Totten C, Raine C. Factors affecting sound-source localization in children with simultaneous or sequential bilateral cochlear implants. Ear Hear. 2019;40(4):870-877. doi: 10.1097/AUD.0000000000000666 [DOI] [PubMed] [Google Scholar]
- 51.Sharma A, Campbell J. A sensitive period for cochlear implantation in deaf children. J Matern Fetal Neonatal Med. 2011;24(suppl 1):151-153. doi: 10.3109/14767058.2011.607614 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 52.Heman-Ackah SE, Roland JT Jr, Waltzman SB. Cochlear implantation in late childhood and adolescence: is there such a thing as ‘too late’? Expert Rev Med Devices. 2012;9(3):201-204. doi: 10.1586/erd.12.21 [DOI] [PubMed] [Google Scholar]
- 53.Kral A, Sharma A. Developmental neuroplasticity after cochlear implantation. Trends Neurosci. 2012;35(2):111-122. doi: 10.1016/j.tins.2011.09.004 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 54.Sharma A, Dorman MF, Kral A. The influence of a sensitive period on central auditory development in children with unilateral and bilateral cochlear implants. Hear Res. 2005;203(1-2):134-143. doi: 10.1016/j.heares.2004.12.010 [DOI] [PubMed] [Google Scholar]
- 55.Sharma A, Dorman MF, Spahr AJ. A sensitive period for the development of the central auditory system in children with cochlear implants: implications for age of implantation. Ear Hear. 2002;23(6):532-539. doi: 10.1097/00003446-200212000-00004 [DOI] [PubMed] [Google Scholar]
- 56.Dorman MF, Sharma A, Gilley P, Martin K, Roland P. Central auditory development: evidence from CAEP measurements in children fit with cochlear implants. J Commun Disord. 2007;40(4):284-294. doi: 10.1016/j.jcomdis.2007.03.007 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 57.Sharma A, Gilley PM, Dorman MF, Baldwin R. Deprivation-induced cortical reorganization in children with cochlear implants. Int J Audiol. 2007;46(9):494-499. doi: 10.1080/14992020701524836 [DOI] [PubMed] [Google Scholar]
- 58.Sharma A, Nash AA, Dorman M. Cortical development, plasticity and re-organization in children with cochlear implants. J Commun Disord. 2009;42(4):272-279. doi: 10.1016/j.jcomdis.2009.03.003 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 59.Svirsky MA, Teoh SW, Neuburger H. Development of language and speech perception in congenitally, profoundly deaf children as a function of age at cochlear implantation. Audiol Neurootol. 2004;9(4):224-233. doi: 10.1159/000078392 [DOI] [PubMed] [Google Scholar]
- 60.McConkey Robbins A, Koch DB, Osberger MJ, Zimmerman-Phillips S, Kishon-Rabin L. Effect of age at cochlear implantation on auditory skill development in infants and toddlers. Arch Otolaryngol Head Neck Surg. 2004;130(5):570-574. doi: 10.1001/archotol.130.5.570 [DOI] [PubMed] [Google Scholar]
- 61.Holt RF, Svirsky MA. An exploratory look at pediatric cochlear implantation: is earliest always best? Ear Hear. 2008;29(4):492-511. doi: 10.1097/AUD.0b013e31816c409f [DOI] [PMC free article] [PubMed] [Google Scholar]
- 62.Niparko JK, Tobey EA, Thal DJ, et al. ; CDaCI Investigative Team . Spoken language development in children following cochlear implantation. JAMA. 2010;303(15):1498-1506. doi: 10.1001/jama.2010.451 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 63.Sharma A, Glick H, Campbell J, Torres J, Dorman M, Zeitler DM. Cortical plasticity and reorganization in pediatric single-sided deafness pre- and postcochlear implantation: a case study. Otol Neurotol. 2016;37(2):e26-e34. doi: 10.1097/MAO.0000000000000904 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 64.Cohen SM, Svirsky MA. Duration of unilateral auditory deprivation is associated with reduced speech perception after cochlear implantation: a single-sided deafness study. Cochlear Implants Int. 2019;20(2):51-56. doi: 10.1080/14670100.2018.1550469 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 65.Gaylor JM, Raman G, Chung M, et al. Cochlear implantation in adults: a systematic review and meta-analysis. JAMA Otolaryngol Head Neck Surg. 2013;139(3):265-272. doi: 10.1001/jamaoto.2013.1744 [DOI] [PubMed] [Google Scholar]
- 66.Maidment DW, Barker AB, Xia J, Ferguson MA. A systematic review and meta-analysis assessing the effectiveness of alternative listening devices to conventional hearing aids in adults with hearing loss. Int J Audiol. 2018;57(10):721-729. doi: 10.1080/14992027.2018.1493546 [DOI] [PubMed] [Google Scholar]
- 67.Pulsifer MB, Salorio CF, Niparko JK. Developmental, audiological, and speech perception functioning in children after cochlear implant surgery. Arch Pediatr Adolesc Med. 2003;157(6):552-558. doi: 10.1001/archpedi.157.6.552 [DOI] [PubMed] [Google Scholar]
- 68.Nikolopoulos TP, Dyar D, Archbold S, O’Donoghue GM. Development of spoken language grammar following cochlear implantation in prelingually deaf children. Arch Otolaryngol Head Neck Surg. 2004;130(5):629-633. doi: 10.1001/archotol.130.5.629 [DOI] [PubMed] [Google Scholar]
- 69.Bille J, Fink-Jensen V, Ovesen T. Outcome of cochlear implantation in children with cochlear malformations. Eur Arch Otorhinolaryngol. 2015;272(3):583-589. doi: 10.1007/s00405-014-2883-z [DOI] [PubMed] [Google Scholar]
- 70.Bauer PW, Wippold FJ II, Goldin J, Lusk RP. Cochlear implantation in children with CHARGE association. Arch Otolaryngol Head Neck Surg. 2002;128(9):1013-1017. doi: 10.1001/archotol.128.9.1013 [DOI] [PubMed] [Google Scholar]
- 71.Busi M, Rosignoli M, Castiglione A, et al. Cochlear implant outcomes and genetic mutations in children with ear and brain anomalies. Biomed Res Int. 2015;2015:696281. doi: 10.1155/2015/696281 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 72.Wu CC, Lee YC, Chen PJ, Hsu CJ. Predominance of genetic diagnosis and imaging results as predictors in determining the speech perception performance outcome after cochlear implantation in children. Arch Pediatr Adolesc Med. 2008;162(3):269-276. doi: 10.1001/archpediatrics.2007.59 [DOI] [PubMed] [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.
Supplementary Materials
eTable 1. MOOSE (Meta-analyses Of Observational Studies in Epidemiology) Checklist
eTable 2. Newcastle-Ottawa Scale for Quality Assessment of Nonrandomized Studies in Meta-Analyses
eTable 3. Reasons for Article Exclusions Following Full-Text Review
eMethods. Complete Search Strategy
eFigure. Box Plot Comparison of Median and Interquartile Ranges of Duration of Deafness Between CI Usage Groups
eReferences