

Abstract
Introduction
Human papillomavirus (HPV) is an important risk factor for oropharyngeal cancer. Individuals with human immunodeficiency virus (HIV) have higher oral HPV prevalence but the risk factors for oral HPV infection are not well understood for either HIV-positive or HIV-negative individuals.
Methods
This study was nested within the MACS (men) and WIHS (women) cohorts. Exfoliated oral epithelial cells were collected from 379 HIV-positive and 266 at-risk HIV-negative individuals using a rinse and gargle with Scope™ mouthwash. Samples were tested for 36 types of HPV DNA using PGMY09/11 consensus primers and reverse line blot hybridization. Risk factors for oral HPV infection were explored using logistic regression with generalized estimating equations (GEE) in this cross-sectional analysis.
Results
Prevalent oral HPV infection was common (34%), including HPV16 infection in 5.7% of participants. HIV-positive individuals had increased odds of prevalent oral HPV infection compared to HIV-negative individuals (aOR=2.1, 95%CI=1.6–2.8). Risk factors for prevalent oral HPV differed in HIV-positive and HIV-negative participants. Among HIV-negative individuals, higher number of recent oral sex or rimming partners were strong risk factors for prevalent oral HPV infection (each p-trend<0.01). In contrast, among HIV-positive individuals lower CD4 T-cell count (p-trend<0.001) and higher number of lifetime sexual partners (p-trend=0.03) were strong risk factors.
Conclusions
Oral HPV prevalence was elevated in HIV-positive individuals after controlling for differences in cigarette smoking and sexual behavior, supporting the possibility that HIV may affect the natural history of oral HPV.
Impact
Immunosuppression may contribute to increased persistence or progression of oral HPV infection.
User defined keywords: Oral HPV, HIV, risk factors
CEBP defined keywords: Head and Neck/Oral Cancer; Epidemiology; Infections and the etiology of cancer, Diet, Alcohol, Smoking, and other Lifestyle Factors; Biomarkers of Human Exposure to carcinogens and DNA damaging agents; DNA tumor viruses
Introduction
Human Papillomavirus (HPV) infection has recently been identified as a causal factor in a subset of head and neck squamous cell cancers, primarily oropharyngeal cancers.(1–4) These HPV-positive tumors represent a growing cancer burden; the incidence of oropharyngeal cancers has increased over the past several decades,(5–8) in stark contrast to the decreasing incidence of other head and neck cancer sub-sites.(8, 9) It has been hypothesized that changes in sexual behavior may have caused this increase, although this has not been well evaluated.
Initial studies suggest that HIV-positive individuals have an elevated risk of oropharyngeal cancer, as well as other HPV-related cancers.(8, 10–13) This increase could be explained by the effects of HIV-related immunosuppression on HPV, but alternatively might be explained by higher rates of smoking(14) and the shared sexual risk factors between HIV and HPV.
The prevalence of oral HPV16 infection, the HPV type which accounts for the majority of HPV-positive oropharynx cancers,(1) has been estimated to be approximately 1.3% among healthy adults.(15) Higher oral HPV16 prevalence has been reported among HIV-positive individuals (2–6%).(16–18) In initial studies, oral HPV prevalence was associated with cigarette use, higher number of recent and lifetime oral sexual partners, and immunosuppression;(17, 19–22) however, the relative contribution of each of these factors on the higher prevalence of oral HPV among HIV-positive individuals is unclear.
The effect of immunosuppression on oral HPV natural history is unknown. Recent research suggests highly active antiretroviral therapy (HAART) may not decrease oral HPV prevalence(16, 22) or oral warts.(23, 24) This contrasts with the HAART era reductions seen in other oral lesions(24) and HIV shedding in saliva.(25) Lower CD4 T cell count is known to be associated with increased cervical HPV incidence, persistence, and progression to pre-cancer, but the effect of immunosupression on oral HPV has not been evaluated.(26, 27) The current study evaluated differences in risk factors for prevalent oral HPV infection in HIV-positive and HIV-negative individuals. Understanding these differences may shed light on whether the increased oral HPV prevalence and higher incidence of oropharyngeal cancers among people with HIV may be due to differences in sexual behavior (HPV acquisition), tobacco use (a known cause of head and neck cancer), or HIV-related immunosuppression.
Methods
Study Population and Study Design
This cross-sectional study was based within two multi-site U.S. cohort studies of HIV-positive and at-risk HIV-negative individuals: one cohort of women, the Women Interagency HIV Study (WIHS)(28, 29) and one cohort of men who have sex with men (MSM), the Multicenter AIDS Cohort Study (MACS).(30–32) These cohorts were designed to be methodologically similar and include HIV-negative individuals at risk for HIV infection based on their sexual or injection drug use behaviors. The current study is the initial phase of a larger natural history study of oral HPV infection in these two cohorts.
Briefly, the MACS and WIHS began in 1984 and 1994 respectively, with additional enrollment in 1987–91 (MACS- only), and 2001–03. MACS and WIHS participants undergo a semi-annual interview which includes medical history, demographic, and behavioral questions. There is also a physical examination and venipuncture, where the blood is tested for CD4 T cell count and HIV viral load. Between April 2009 and March 2010, we enrolled a convenience sample of 365 men and 280 women.
The study design stratified enrollment by cohort (365 MACS and 280 WIHS), HIV status (379 HIV-positive and 266 HIV-negative), and among HIV-positive individuals by ever/never HAART use (312 HAART experienced and 67 never HAART users). To enrich for HAART-naïve participants; all interested HAART naïve participants at these sites were enrolled. We enrolled 192 HIV-positive and 173 HIV-negative men from the Baltimore, Chicago and Pittsburgh MACS sites, and 187 HIV-positive, 93 HIV-negative women from the Brooklyn, Bronx, and Chicago WIHS sites. This sample represents 25% of current MACS and 26% of current WIHS participants at the sites enrolled. The study protocol was approved by the MACS and WIHS executive committees as well as the Institutional Review Boards at each site. Written informed consent was received from each participant.
An oral rinse sample was collected as part of this sub-study using a 30 second swish and gargle of 10 mL of Scope™ mouthwash, as previously described.(33) Relevant behavioral measures routinely collected by the MACS and WIHS were also evaluated in this study. Self reported lifetime use and past six months use (called recent use hereafter) of recreational and therapeutic drugs, alcohol, cigarettes, and sexual behavior were collected by interview administered questionnaire in the WIHS and computer assisted self interview (CASI) in the MACS. Fellatio (performing oral sex on a man) was defined as “he put his penis in your mouth” in the MACS and “a blow job or putting his penis in your mouth” in the WIHS. Cunnilingus (performing oral sex on a woman) was defined as “you used your tongue to touch or lick her genitals (vagina, clitoris)” in the MACS and any reported sexual activity with a female in the WIHS. The number of male or female partners an individual performed fellatio or cunnilingus on is referred to as the number of oral sex partners hereafter. Data on rimming, collected only in the MACS, was defined as “you used your tongue to touch or lick his or her anus/butt”. Updated information on lifetime oral sex history was acquired for most participants, but the complete history was not acquired for a proportion of MACS (44%) and WIHS (21%) participants. The updated number of lifetime oral sex partners for these individuals was imputed (see statistical methods below). Recent cigarette smoking was defined as using at least one cigarette per day for the past six months. Recent alcohol use was defined as drinking at least once in the past month.
The definition of HAART was guided by the DHHS/Kaiser Panel(34) and is defined as: the reported use of three or more antiretroviral medications, one of which has to be a protease inhibitor (PI), a non-nucleoside reverse transcriptase inhibitor (NNRTI), one of the NRTIs abacavir or tenofovir, an integrase inhibitor, or an entry inhibitor. Nadir CD4 was the lowest CD4 T cell count observed while in the MACS/WIHS study.
Laboratory Analyses
After collection, oral rinse samples were stored at 4°C and shipped to a laboratory run by Dr. Maura Gillison at the Ohio State University for processing and testing. DNA was isolated from Scope™ oral rinse samples by centrifugation, re-suspended in Phosphate buffered saline (PBS), and purified using a magnetic bead-based automated platform (QIAsymphony SP, Qiagen), as previously described.(35) The purified DNA was then analyzed for 36 different HPV types using PGMY09/11 PCR primer pools and reverse line blot hybridization. Samples were considered evaluable if β-globin positive, and considered insufficient and excluded from the analysis if β-globin negative. HPV types detected were classified into non-oncogenic (low-risk) and oncogenic (high-risk) type categories as previously established by the World Health Organization’s International Agency for Research on Cancer (IARC).(36–38) Oncogenic HPV types included HPV 16, 18, 31, 33, 35, 39, 45, 51, 52, 56, 58, 59, 68, and 73. All other types detected were considered non-oncogenic including HPV 6, 11, 26, 40, 42, 53, 54, 55, 61, 62, 64, 66, 67, 69, 70, 71, 72, 81, 82, 83, 84, and 89.
Statistical Analyses
Characteristics of HIV-positive and HIV-negative individuals were compared using chi-square tests for categorical data, and t-tests for continuous variables. Overall oral HPV status was defined as positive for anyone who had any of the 36 HPV types detected, while all others were considered HPV-negative. Additionally, type-specific HPV prevalence was estimated where participants were categorized as positive or negative for each of the 36 different types of HPV tested.
While the number of lifetime sexual partners at MACS and WIHS study baseline was collected for all participants, 34% of the 645 participants were not asked about their updated number of lifetime number of oral sex partners. Therefore, an updated number of lifetime oral sex partners were imputed for these individuals by calculating the average increase in lifetime oral sexual partners from baseline to current visit among the 425 participants with complete sexual behavioral data. These increases were averaged within subgroups defined by gender, years of follow-up, and number of oral sex partners in the past six months and then imputed to individuals without updated lifetime sexual data within each strata. Results were similar when the 220 individuals without an updated measure of lifetime number of oral sex partners were excluded from the analysis.
Risk factors for oral HPV infection were assessed using logistic regression models with robust variance and generalized estimating equations (GEE) to adjust for within-individual correlations related to multiple observations of the same person (i.e., multiple HPV types) using previously described methods.(39, 40) Crude and adjusted odds ratios (OR & aOR), and 95% confidence intervals (CI) were reported. Type-specific risk factors for oral HPV16 infection and multiple HPV infection were calculated using standard logistic regression models. Factors statistically significant (p<0.05) in the univariate analysis and those considered relevant based on previous literature (age, sexual behavior, gender) were included in multivariate models. Models were stratified by HIV-status, per the study design. The final multivariate model for HIV-negative subjects included age, gender, recent cigarette use, number of recent (last six months) and lifetime oral sex partners, and education level. The final multivariate model for HIV-positive subjects included these variables as well as current CD4 T cell count (called current CD4 hereafter), study site, and recent alcohol use. Analyses that stratified by cohort (MACS vs. WIHS) study were also performed. Fourteen individuals had incomplete covariate information. Therefore, our multivariate analyses were based upon 631 individuals.
Trends in the odds ratios were tested using continuous data when available (age, current CD4, HIV viral load, number of recent and lifetime oral sexual partners) and considering ordinal values as a single continuous variable when data was collected ordinally (education, recent cigarette and alcohol use). Correlation between variables was tested using Pearson’s correlation coefficient. All statistical tests were two-sided and considered significant at α=0.05 level. STATA software (version 10.0; Stata Corp., College Station, TX) was used for all statistical analyses.
Results
Participant characteristics
Characteristics of the 645 participants enrolled are shown in Table 1, stratified by HIV-status and gender. Participants in this study sample were similar to those in the MACS and WIHS cohorts. Participants in the MACS sample were similar to the larger MACS population with regards to median current CD4 (550 vs. 557 cells//µL), median age (52 vs. 54 years), proportion White (66% vs. 66%) and proportion sexually active (71% vs 66%, each p>0.05). Participants in the WIHS samples were similar to the larger WIHS population with regards to median age (45 vs. 46 years) and the proportion White (11% vs. 15%), but those in the WIHS study sample had lower median current CD4 (458 vs. 510 cells/µL) and were more likely to be sexually active in the past six months (71 vs. 63%, each p<0.05) when compared to the entire WIHS cohort. By design, the proportion of HIV-infected participants which were HAART naïve was larger in our sample (19%) than the current MACS (6%) or WIHS (7%) study populations.
Table 1.
Characteristics of men from the Multicenter AIDS Cohort Study (MACS) men) and women from the Women’s Interagency HIV Study (WIHS) at the time of their enrollment into this study between April 2009 and March 2010
| Demographics | Overall | Women: WIHS (%) | Men: MACS (%) | ||
|---|---|---|---|---|---|
| HIV- positive |
HIV- negative |
HIV- positive |
HIV- negative |
||
| N=645 | N=187 | N=93 | N=192 | N=173 | |
| Age: age in years | |||||
| <45 | 198 | 44% | 61% | 17% | 16% |
| 45–54 | 231 | 37% | 26% | 44% | 30% |
| ≥54 | 216 | 19% | 13% | 39% | 54% |
| Race and Ethnicity | |||||
| White non-Hispanic | 271 | 11% | 10% | 59% | 74% |
| African American non-Hispanic | 322 | 70% | 76% | 40% | 25% |
| Hispanic (any race) | 40 | 15% | 12.0% | 0% | 0.6% |
| Other race | 12 | 3.7% | 2.2% | 1.0% | 0.6% |
| Education | |||||
| Any college education | 397 | 30% | 37% | 80% | 89% |
| High school degree | 126 | 30% | 32% | 16% | 6.4% |
| <High school degree | 119 | 40% | 32% | 4.7% | 4.1% |
| Study Site | |||||
| Chicago (MACS and WIHS) | 177 | 32% | 34% | 27% | 19% |
| Baltimore (MACS) | 175 | 0% | 0% | 41% | 55% |
| Pittsburgh (MACS) | 105 | 0% | 0% | 32% | 27% |
| Bronx (WIHS) | 93 | 32% | 34% | NA | NA |
| Brooklyn (WIHS) | 95 | 35% | 31% | NA | NA |
| BEHAVORIAL | |||||
| Number of Cigarettes smoked per day past 6 months | |||||
| <1 ("non-smoker") | 419 | 54% | 52% | 68% | 82% |
| 1 – 9 | 126 | 31% | 31% | 12% | 10% |
| 10–19 | 67 | 13% | 14% | 11% | 5.2% |
| 20 or more | 31 | 2.1% | 3.2% | 10% | 2.9% |
| Number of Alcoholic Drinks consumed past 6 months | |||||
| <1 month ("non-drinker") | 307 | 67% | 54% | 41% | 31% |
| 1/month - <2 per week | 167 | 19% | 24% | 27% | 34% |
| 2–14 per week | 110 | 12% | 17% | 24% | 24% |
| 15 or more per week | 44 | 1.6% | 5% | 7.9% | 12% |
| SEXUAL ACTIVITY | |||||
| Any sexual activity in last 6 months | |||||
| No | 188 | 32% | 23% | 32% | 27% |
| Yes | 455 | 68% | 77% | 68% | 73% |
| Number of male or female partners performed oral sex on in last 6 months | |||||
| 0 partners | 335 | 77% | 60% | 39% | 35% |
| 1 partner | 162 | 20% | 32% | 25% | 28% |
| 2 to 4 partners | 95 | 4% | 7.5% | 20% | 25% |
| 5 or more partners | 52 | 0% | 0% | 16% | 13% |
| Among those performing oral sex in last 6 months: always used barrier | |||||
| No | 280 | 72% | 97.0% | 90% | 98.0% |
| Yes | 27 | 27% | 2.7% | 10% | 1.8% |
| Number of rimming partners in last 6 months* | |||||
| 0 partners | 248 | 67% | 69% | ||
| 1 partner | 60 | 17% | 16% | ||
| 2 to 4 partners | 35 | 8.4% | 11% | ||
| 5 or more partners | 20 | 6.8% | 4.1% | ||
| Lifetime number of oral sex partners | |||||
| 0–4 partners | 218 | 66% | 67% | 8.0% | 9.4% |
| 4–19 partners | 120 | 21% | 19% | 18% | 17% |
| 20–99 partners | 140 | 7.0% | 8.6% | 29% | 38% |
| 100 or more partners | 159 | 5.9% | 4.3% | 45% | 35% |
| HIV-Related | |||||
| Current HAART Use | |||||
| No | 101 | 27% | 27% | ||
| Yes | 278 | 73% | 73% | ||
| Current CD4 cell count: cells/µL | |||||
| >500 | 200 | 46% | 60% | ||
| 200–500 | 139 | 40% | 34% | ||
| <200 | 40 | 14% | 6.8% | ||
| Current HIV viral load: copies/mL | |||||
| <50 | 288 | 54% | 72% | ||
| 50–20,000 | 61 | 32% | 18% | ||
| ≥ 20,000 | 46 | 14% | 9.4% | ||
| Nadir^ CD4 cell count: cells/µL | |||||
| >500 | 52 | 18% | 11% | ||
| 200–500 | 200 | 57% | 53% | ||
| <200 | 112 | 26% | 37% | ||
Data on number of rimming partners was only available in the MACS.
This was the nadir (lowest) CD4 cell count observed while in the MACS/WIHS study.
In this study, most HIV-positive participants were receiving HAART, with median nadir and current CD4 of 266 and 524 cells/µL, respectively. HIV-positive individuals were less educated, and less likely to have recently performed oral sex or to drink alcohol than HIV-negative individuals (each p<0.05, Table 1). HIV-positive individuals were also more likely to be from the WIHS, to be African American, and to smoke cigarettes than HIV-negative individuals (each p<0.05, Table 1).
Oral HPV prevalence
Oral HPV prevalence (34%), including infection with multiple HPV types (14%) was high in this study population (Table 2). The overall prevalence of oncogenic oral HPV infections was lower than that of non-oncogenic infections (18% vs. 23%, p=0.03). However, HPV16 was the most common HPV type detected in the study (prevalence of 5.7%), detected in 2.2% and 5.4% of HIV-negative and HIV-positive women (p=0.21), respectively and in 6.9% and 6.8% of HIV-negative and HIV-positive MSM (p=0.95), respectively. HPV16 constituted a larger proportion of infections detected among HIV-negative than HIV-positive participants (16% vs. 8% p=0.04). The distribution of all oral HPV types detected by HIV status are displayed in Supplemental Table 2, including the most commonly detected oncogenic (HPV16, 59 and 33) and non-oncogenic (HPV55, 62 and 53) types.
Table 2.
Oral HPV Prevalence in HIV-positive and HIV-negative individuals
| Oral HPV Infection | Oral HPV Prevalence |
|||||||
|---|---|---|---|---|---|---|---|---|
| HIV-positive | HIV-negative | χ2 p-value HIV+ vs. HIV− |
Overall N=645 |
|||||
| Women N=187 |
Men N=192 |
Total N=379 |
Women N=93 |
Men N=173 |
Total N=266 |
|||
| Any | 35% | 45% | 40% | 18% | 28% | 25% | <0.001 | 34% |
| Non-oncogenic | 27% | 31% | 29% | 11% | 16% | 14% | <0.001 | 18% |
| Oncogenic | 18% | 23% | 21% | 8.6% | 17% | 14% | 0.03 | 23% |
| HPV 16 | 5.4% | 6.8% | 6.1% | 2.2% | 6.9% | 5.3% | 0.67 | 5.7% |
| Other oncogenic | 17% | 20% | 18% | 7.5% | 11% | 10% | 0.004 | 15% |
| Multiple concurrent | 18% | 19% | 19% | 7.5% | 6.4% | 6.8% | <0.001 | 14% |
Risk factors for prevalent oral HPV infection
HIV-positive individuals were significantly more likely than HIV-negative participants to have a prevalent oral HPV infection detected (adjusted odds ratio [aOR]=2.1, 95%CI=1.6–2.8). This was true for both oncogenic (aOR=1.8, 95%CI=1.3–2.7) and non-oncogenic (aOR=2.3, 95%CI=1.6–3.4) types of oral HPV. Oral HPV16 infection, however, was similarly common among HIV-positive and HIV-negative individuals (aOR=1.3, 95%CI=0.62–2.7).
Recent cigarette smoking was associated with significantly increased odds of oral HPV among both HIV-positive and HIV-negative individuals. There were, however, notable differences between HIV-positive and HIV-negative participants in other risk factors for oral HPV infection (Table 3). The number of recent oral sex partners was the strongest risk factor for prevalent oral HPV among HIV-negative (p-trend=0.003) but not HIV-positive (p-trend=0.88) participants. In the MACS, where data on rimming (oral-anal contact) was collected, number of recent rimming partners was also significantly associated with oral HPV among HIV-negative MSM. However, the number of recent oral sex and rimming partners were highly correlated (r=0.65). In contrast to that observed for recent sex behavior, lifetime oral sex behavior was associated with oral HPV prevalence in HIV-positive (p-trend=0.03), but not HIV-negative (p-trend=0.11) individuals. Odds of oral HPV also increased significantly with older age among HIV-negative individuals (Table 3, p-trend=0.01). Always using a condom during oral sex, race/ethnicity, cigarette smoking intensity and duration, and recent marijuana use were not associated with odds of oral HPV in HIV-positive or HIV-negative individuals (data not shown).
Table 3.
Risk factors associated with prevalent oral HPV infection in univariate and multivariate analysis, by HIV-status.
|
Risk Factors |
Overall Oral HPV Prevalence |
OR (95%CI) |
|||
|---|---|---|---|---|---|
| HIV-positive | HIV-negative | ||||
| Univariate | Multivariate | Univariate | Multivariate | ||
| Age | |||||
| <45 | 31% | 1 | 1 | 1 | 1 |
| 45–54 | 36% | 0.92 (0.63–1.3) | 0.84 (0.57–1.2) | 1.7 (0.85–3.2) | 1.2 (0.54–2.7) |
| ≥54 | 35% | 1.1 (0.71–1.6) | 1.2 (0.77–1.8) | 1.8 (0.97–3.4) | 2.1 (0.96–4.4) |
| p-trend | 0.48* | 0.30* | 0.02 | 0.01 | |
| Gender | |||||
| Female (WIHS) | 30% | 1 | 1 | 1 | 1 |
| Male (MACS) | 38% | 1.2 (0.82–1.6) | 3.0 (1.7–5.1) | 1.2 (0.71–2.2) | 0.97 (0.45–2.1) |
| Education | |||||
| Any College | 33% | 1 | 1 | 1 | 1 |
| High school degree | 33% | 1.3 (0.87–2.1) | 1.8 (1.0–3.1) | 1.2 (0.53–2.5) | 1.3 (0.56–2.9) |
| < High school degree | 38% | 1.5 (1.0–2.3) | 2.1 (1.2–3.5) | 0.94 (0.44–2.0) | 0.90 (0.34–2.3) |
| p-trend | 0.02 | <0.001 | 0.99 | 0.66 | |
| BEHAVORIAL | |||||
| Smoked Cigarettes in past 6 months | |||||
| No (<1 per day) | 29% | 1 | 1 | 1 | 1 |
| Yes | 44% | 1.8 (1.3–2.5)* | 1.7 (1.2–2.3)* | 1.8 (1.1–2.9)* | 2.8 (1.8–4.4)* |
| Consumed Alcoholic Drinks in past 6 months | |||||
| No (<1 per month) | 37% | 1 | 1 | 1 | |
| Yes | 31% | 0.73 (0.51–1.0) | 0.74 (0.49–1.1) | 1.2 (0.70–2.0) | |
| SEXUAL ACTIVITY | |||||
| Number of oral sex partners in last 6 months | |||||
| 0 partners | 32% | 1 | 1 | 1 | 1 |
| 1 partner | 32% | 0.92 (0.63–1.3) | 0.90 (0.60–1.4) | 0.95 (0.49–1.8) | 1.4 (0.69–2.9) |
| 2 to 4 partners | 36% | 0.84 (0.47–1.5) | 0.85 (0.50–1.5) | 1.7 (0.92–3.1) | 2.9 (1.5–5.8) |
| 5 or more partners | 46% | 1.3 (0.71–2.3) | 1.2 (0.63–2.1) | 1.8 (0.92–3.4) | 2.7 (1.3–5.8) |
| p-trend | 0.46 | 0.88 | 0.01* | 0.003* | |
| Lifetime number of oral sex partners | |||||
| 0–4 partners | 28% | 1 | 1 | 1 | 1 |
| 5–19 partners | 32% | 1.2 (0.74–1.9) | 1.2 (0.72–1.9) | 1.4 (0.61–3.0) | 1.4 (0.59–3.1) |
| 20–99 partners | 34% | 1.3 (0.78–2.1) | 1.5 (0.82–2.7) | 1.0 (0.51–2.1) | 0.87 (0.33–2.3) |
| 100 or more partners | 44% | 1.4 (0.94–2.2) | 1.8 (1.0–3.2) | 1.6 (0.83–3.1) | 1.3 (0.52–3.4) |
| p-trend | 0.05 *# | 0.03*# | 0.03# | 0.11# | |
| Number of rimming partners in last 6 months** | |||||
| 0 partners | 33% | 1 | 1^ | 1 | 1^ |
| 1 partner | 43% | 1.1 (0.68–1.8) | 1.3 (0.75–2.1) | 1.6 (0.81–3.1) | 2.4 (1.1–5.0) |
| 2 to 4 partners | 46% | 1.0 (0.51–1.9) | 1.0 (0.51–1.9) | 2.1 (0.97–4.4) | 2.7 (1.2–6.1) |
| 5 or more partners | 50% | 1.0 (0.31–3.2) | 1.0 (0.31–2.9) | 2.5 (1.4–4.7) | 3.0 (1.6–5.9) |
| p-trend | 0.67 | 0.51 | <0.001 | 0.002 | |
| HIV RELATED | |||||
| Current CD4 T cell count | |||||
| >500 cells/uL | 37% | 1 | 1 | ||
| 200–500 cells/uL | 41% | 1.7 (1.2–2.4) | 1.6 (1.1–2.3) | ||
| <200 cells/uL | 58% | 2.6 (1.7–4.1) | 2.1 (1.3–3.2) | ||
| p-trend | <0.001 | <0.001 | |||
| Nadir CD4 T cell count | |||||
| >500 cells/uL | 26% | 1 | |||
| 200–500 cells/uL | 38% | 1.8 (0.98–3.2) | |||
| <200 cells/uL | 50% | 2.2 (1.2–4.1) | |||
| p-trend | 0.003 | ||||
| Current HAART | |||||
| No | 34% | 1 | |||
| Yes | 43% | 1.1 (0.73–1.6) | |||
| Current HIV viral load | |||||
| <50 copies/mL | 38% | 1 | |||
| 50–20,000 copies/mL | 39% | 1.3 (0.90–2.0) | |||
| ≥ 20,000 copies/mL | 59% | 2.3 (1.5–3.5) | |||
| p-trend | 0.001 | ||||
Model adjusted for age, gender, education, current cigarette use, and number of recent and lifetime oral sex partners. HIV-positive model was also adjusted for alcohol use, study site, and current CD4 T cell count.
Effect modification by MACS/WIHS study cohort not included in this model, but is reported in Table 4.
The data for rimming presented is in analysis among MACS participants only (because rimming was not measured in the WIHS) and number of recent oral sex partners was not adjusted for in this model because number of recent oral and rimming partners were strongly correlated (r=0.65). Rimming was not adjusted for in the other variables presented in the table.
Lifetime oral sex partners p-trend excludes 46 individuals with >500 lifetime sex partners. When these individuals were included p-trend is attenuated.
Severity of immunosuppression was the strongest risk factor for prevalent oral HPV among those with HIV (p-trend<0.001, Figure 1 and Table 3, 4) including an association with lower current and nadir CD4, and higher HIV viral load (Table 3). Current CD4 was moderately correlated with current HIV viral load (r=0.48) and with nadir CD4 (r=0.28). However, when modeled together current CD4 was a stronger predictor than either nadir CD4 or current HIV-viral load (Supplemental Table 1). HIV-positive individuals with current CD4>500 remained at significantly increased odds of oral HPV (aOR=1.6, 95%CI=1.1–2.3) but had similar odds of HPV16 (aOR=0.47, 95%CI=0.16–1.4) compared to HIV-negative participants. Oral HPV prevalence was similar among HIV-positive HAART ever users and never users (42% vs. 34%, p=0.24) and current HAART users and non-users (43% vs. 34%, p=0.11).
Figure 1.
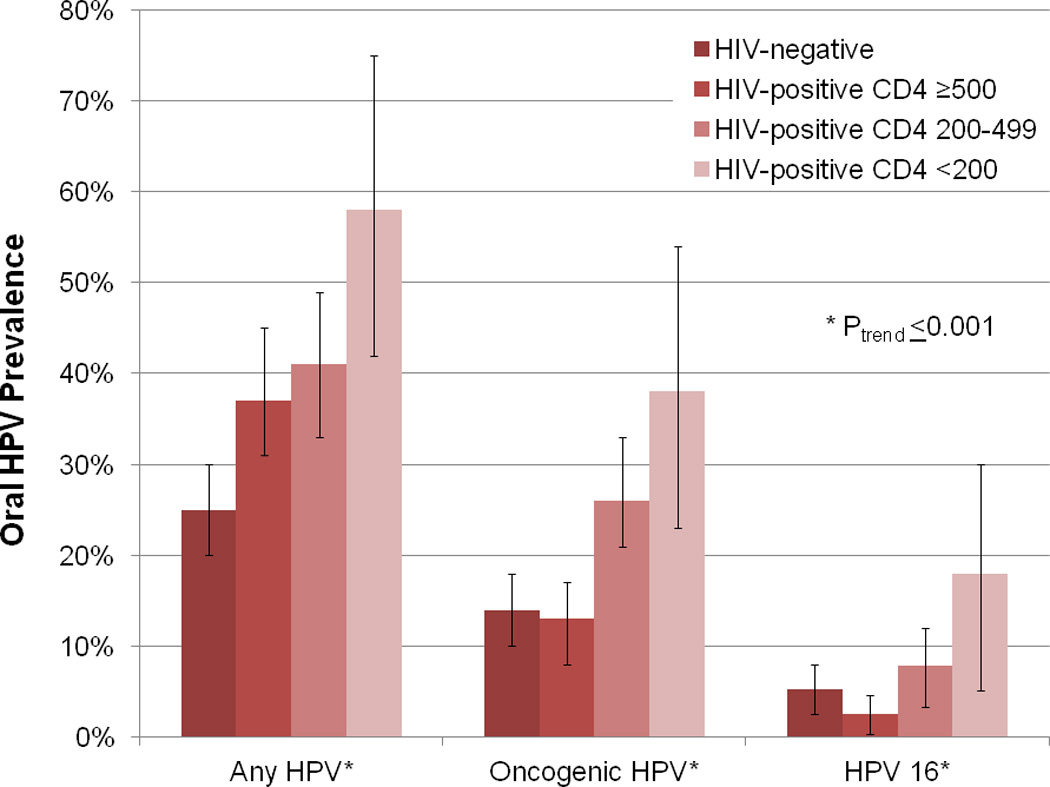
Oral HPV Prevalence (unadjusted) by HIV status and current CD4 T cell count among 379 HIV-positive individuals
Table 4.
Multivariate risk factors for prevalent oral HPV infection among HIV-positive and HIV-negative subjects stratified by study cohort (MACS men compared with WIHS women).
| Risk Factors | Adjusted OR (95%CI) |
|||
|---|---|---|---|---|
| HIV-positive | HIV-negative | |||
| Men | Women | Men | Women | |
| Age | ||||
| <45 | 1 | 1 | 1 | 1 |
| 45–54 | 0.65 (0.39–1.5) | 0.84 (0.48–1.5) | 1.1 (0.43–2.6) | 1.2 (0.37–3.9) |
| ≥54 | 0.76 (0.43–1.3) | 1.8 (0.97–3.4) | 1.9 (0.74–4.7) | 1.0 (0.20–5.6) |
| p-trend | 0.44 | 0.03 | 0.07 | 0.31 |
| Education | ||||
| Any College | 1 | 1 | 1 | 1 |
| High school degree | 1.8 (0.81–4.0) | 1.5 (0.75–3.1) | 1.5 (0.42–5.3) | 1.0 (0.25–4.1) |
| < High school degree | 1.7 (0.73–3.9) | 1.7 (0.94–3.1) | 1.5 (0.44–4.8) | 0.54 (0.15–1.9) |
| p-trend | 0.02 | 0.07 | 0.20 | 0.38 |
| BEHAVORIAL | ||||
| Smoked Cigarettes in past 6 months | ||||
| No (<1 per day) | 1 | 1 | 1 | 1 |
| Yes | 1.2 (0.73–2.0) | 2.2 (1.4–3.7) | 1.7 (0.84–3.5) | 14 (3.2–64) |
| Consumed Alcoholic Drinks in past 6 months | ||||
| No (<1 per month) | 1 | 1 | ||
| Yes | 0.76 (0.49–1.2) | 0.95 (0.47–1.9) | ||
| SEXUAL ACTIVITY | ||||
| Number of oral sex partners in last 6 months | ||||
| 0 partners | 1 | 1 | 1 | 1 |
| 1 partner | 1.0 (0.55–1.8) | 0.93 (0.48–1.8) | 1.4 (0.57–3.3) | 1.1 (0.33–3.8) |
| 2 to 4 partners | 1.0 (0.57–1.9) | ~~ | 3.3 (1.6–6.8) | ~~ |
| 5 or more partners | 1.4 (0.74–2.5) | ~~ | 3.1 (1.5–6.3) | ~~ |
| p-trend | 0.75 | 0.31 | 0.005 | ~~ |
| Lifetime number of sex partners | ||||
| 0–4 partners | 1 | 1 | 1 | 1 |
| 5–19 partners | 0.81 (0.32–2.1) | 1.0 (0.55–1.8) | 1.8 (0.48–6.4) | 1.1 (0.32–3.6) |
| 20–99 partners | 0.68 (0.22–2.1) | 2.3 (1.4–3.9) | 1.0 (0.31–3.2) | 1.5 (0.16–14) |
| 100 or more partners | 0.82 (0.26–2.6) | 1.5 (0.46–4.7) | ||
| p-trend | 0.42# | <0.001# | 0.16# | 0.09# |
| Number of rimming partners in last 6 months^ | ||||
| 0 partners | 1 | 1 | ||
| 1 partner | 1.3 (0.75–2.1) | 2.4 (1.1–5.0) | ||
| 2 to 4 partners | 1.0 (0.51–1.9) | 2.7 (1.2–6.1) | ||
| 5 or more partners | 1.0 (0.31–2.9) | 3.0 (1.5–5.9) | ||
| p-trend | 0.51 | 0.002 | ||
| HIV RELATED | ||||
| Current CD4 T cell count | ||||
| >500 cells/uL | 1 | 1 | ||
| 200–500 cells/uL | 1.6 (0.93–2.8) | 1.6 (0.92–2.6) | ||
| <200 cells/uL | 1.9 (1.1–3.4) | 2.1 (1.2–3.6) | ||
| p-trend | 0.06 | <0.001 | ||
Models adjusted for age, education, current cigarette use, number of recent and lifetime oral sex partners. HIV-positive models also adjusted for study site, current alcohol use, and current CD4 T cell count.
These categories had less than 10 individuals and therefore were not included in the models.
The data for rimming presented is in analysis among MACS participants only (since rimming was not measured in the WIHS) and number of recent oral sex partners was not adjusted for in this model since number of recent oral nd rimming partners were strongly correlated (r=0.65). Rimming was not adjusted for in other models presented in the table.
Lifetime oral sex partners p-trend excludes 46 individuals with >500 lifetime sex partners. When these individuals were included p-trend is attenuated.
A strong dose response with lower current CD4 was observed among both HAART-naïve (p-trend=0.03) and HAART-experienced (p-trend=0.002) individuals. This trend was especially strong for HPV16 infection where the median current CD4 was 238 cells/uL among those with HPV16 infection compared to 481 cells/uL among those infected with other HPV types (p=0.002). The association between current CD4 and oral HPV16 was significantly stronger than the association of current CD4 with all other HPV types (p=0.02). Contrasting individuals with current CD4<200 to HIV-positive individuals with current CD4≥500, the OR for HPV16 was over four fold greater than the OR for all other HPV types (aOR=4.5, 95%CI=1.3–16).
When the study population was stratified by MACS/WIHS cohort, current CD4 remained influential among HIV-positive individuals in both cohorts, but there were differences by cohort in other risk factors. The associations of cigarette smoking and lifetime number of oral sexual partners with oral HPV prevalence were more notable among WIHS participants, while recent number oral sex partners was more notable among MACS participants (Table 4).
Conclusions
The prevalence of oral HPV observed in this study is one of the highest ever reported in a non-cancer population. Specifically, this prevalence was higher than that reported in previous studies of HIV-positive (40% vs. 16–37%)(16, 17, 21, 22, 41) and HIV-negative (25% vs. 4–18%)(15, 19, 42–44) individuals. This may be explained at least in part by the older age and higher number of past and recent sexual partners of our population.(45, 46) The findings suggest that the higher oral HPV prevalence among HIV-positive individuals is not fully explained by differences in sexual behavior and cigarette smoking. Indeed, after controlling for cigarette smoking and sexual behavior, odds of oral HPV remained significantly elevated in HIV-positive compared to HIV-negative individuals, and were strongly associated with reduced current CD4. These findings are consistent with there being a strong independent association of HIV-related immunosuppression with the burden of oral HPV infection.
Risk factors for prevalent oral HPV infection differed among HIV-positive and HIV-negative individuals in this study. While odds of oral HPV infection were associated with recent number of oral sex partners in HIV-negative individuals, they were associated with lifetime number of oral sex partners and current CD4 in HIV-positive individuals. These differences are consistent with the hypothesis that prevalent oral HPV infections may represent primarily recently acquired infection among HIV-negative adults but in HIV-positive adults may be more likely to represent persistent, or previously acquired re-activated oral HPV infections. The strong association between current CD4 and oral HPV prevalence in this study is consistent with previous research demonstrating an association between immunosuppression and increased risk of cervical HPV persistence (27, 47, 48) and progression to cervical cancer (26, 49, 50). In longitudinal follow-up of this study population we will explore whether HIV-related immunosuppression may have a similar effect on oral HPV natural history.
Our findings suggest that reduced current CD4 may have a stronger effect on oral HPV16 prevalence than other HPV types. This is in contrast to a previous study on cervical HPV in the WIHS which reported a weaker effect of reduced current CD4 on cervical HPV16 infection than on other cervical HPV types.(39, 51) It is unclear whether there may be immunologic differences between the cervix and the oral cavity which might affect the relationship between CD4 and HPV type-specific clearance. Considering the relatively higher prevalence of oral HPV16 in this population (5.7%) and that HPV16 constitutes a larger percentage of HPV-positive oropharyngeal cancers than cervical cancers(1, 52) further exploration is warranted.
The significant association of recent oral sexual behavior with increased odds of oral HPV among HIV-negative participants in this study is consistent with several previous studies,(19, 21, 41) although no association with oral sex was reported in one other recent study.(53) To our knowledge, this is the first study to identify rimming (oral-anal contact) as a potential transmitter of oral HPV. As anal HPV prevalence is high among MSM,(54, 55) it is conceivable that rimming could lead to oral HPV exposure. However, while 32% of MACS participants reported rimming in the past six months, the behavior was highly correlated with oral sex behavior. Thus, it is difficult to determine whether there is an independent role for rimming in the transmission of oral HPV infection.
This study included participants from two high-risk cohorts, the MACS and the WIHS, with distinct study populations. While the findings were similar in the two cohorts, the associations between prevalent oral HPV with cigarette smoking and recent and lifetime sexual behavior differed between WIHS and MACS participants. Reasons for these differences are unclear and may be explained by the small sample sizes in stratified analyses. Alternatively, the effects of cigarette smoking on oral HPV persistence, if any, may be small in comparison to the risk of new acquisition with sexual risk taking and might therefore be harder to observe in a population such as the MACS with high median number of sexual partners (and thus heavier HPV exposure) than in the WIHS. In addition, the impact of age and tobacco-related immunosuppression may be expected to be less apparent among HIV-positive individuals, which might explain the lack of association among HIV-positive MACS participants, who were older and had lower nadir CD4 than WIHS participants. The higher number of lifetime sexual partners in the MACS may have led to saturation of risk that could explain why this association was significant in the WIHS, but not the MACS. The higher level of sexual risk taking in the MACS likely also explains why recent sexual behavior was more notable in the MACS than the WIHS.
There are several limitations to this study. The HIV-positive and HIV-negative populations studied were selected because of their high risk and may not be representative of others in the general population. Second, while we report heterogeneity in some risk factors by HIV-status and gender, some of these stratified analyses were underpowered. In addition, as oral HPV infection was only measured at one time point, we cannot differentiate between transient newly acquired infection and persistent or re-activated latent infections. Third, while oral HPV infections detected with the oral rinse have been strongly associated with odds of oropharyngeal cancer (3) and shown to have a higher DNA yield and quality than other oral sampling techniques such as focal brush sampling(56–58), oral rinse sampling cannot differentiate the site of infection, i.e. oral cavity or oropharynx. Lastly, while a strength of MACS and WIHS data is their extensive characterization of sexual risk behavior over time, each study relies upon self-reported data and missing values were imputed for lifetime number of oral sex partners which could lead to misclassification. Strengths of this study include the detailed biological and behavioral data collected, the optimized oral rinse processing and HPV testing technique,(35) and the inclusion of both HIV-positive and risk-matched HIV-negative individuals of both genders.
This study suggests that oral HPV infection is common in HIV-positive and at risk HIV-negative women and MSM. HIV-positive individuals had a higher prevalence of oral HPV infection and different risk factors associated with infection than HIV-negative individuals. Whether HIV-related immunosuppression has an effect on oral HPV natural history, similar to that known for cervical HPV, will need to be explored longitudinally.
Supplementary Material
Acknowledgements
Data in this manuscript were collected by the Multicenter AIDS Cohort Study (MACS) with centers (Principal Investigators) at The Johns Hopkins Bloomberg School of Public Health (Joseph B. Margolick, Lisa P. Jacobson), Howard Brown Health Center, Feinberg School of Medicine, Northwestern University, and Cook County Bureau of Health Services (John P. Phair, Steven M. Wolinsky), and University of Pittsburgh (Charles R. Rinaldo). The MACS is funded by the National Institute of Allergy and Infectious Diseases, with additional supplemental funding from the National Cancer Institute. UO1-AI-35042, UL1-RR025005(GCRC), UO1-AI-35043, UO1-AI-35039, UO1-AI-35040, UO1-AI-35041.
Data in this manuscript were also collected by the Women's Interagency HIV Study (WIHS) Collaborative Study Group with centers (Principal Investigators) at New York City/Bronx Consortium (Kathryn Anastos); Brooklyn, NY (Howard Minkoff); The Connie Wofsy Study Consortium of NorthernCalifornia (Ruth Greenblatt); Chicago Consortium (Mardge Cohen); Data Coordinating Center (Stephen Gange). The WIHS is funded by the National Institute of Allergy and Infectious Diseases (UO1-AI-35004, UO1-AI-31834, UO1-AI-34994, UO1-AI-34989, UO1-AI-34993, and UO1-AI-42590) and by the Eunice Kennedy Shriver National Institute of Child Health and Human Development (UO1-HD-32632). The study is co-funded by the National Cancer Institute, the National Institute on Drug Abuse, and the National Institute on Deafness and Other Communication Disorders. Funding is also provided by the National Center for Research Resources (UCSF-CTSI Grant Number UL1 RR024131). The contents of this publication are solely the responsibility of the authors and do not necessarily represent the official views of the National Institutes of Health.
Grant Support:
This study was made possible by a supplement to U01-A1-35043 by NIH/NCI (PI Jacobson), by R01 DE021395 (PI D’Souza), and by P30 AI 082151 (PI Landry).
References
- 1.Kreimer AR, Clifford GM, Boyle P, Franceschi S. Human papillomavirus types in head and neck squamous cell carcinomas worldwide: A systematic review. Cancer Epidemiol Biomarkers Prev. 2005;14(2):467–475. doi: 10.1158/1055-9965.EPI-04-0551. [DOI] [PubMed] [Google Scholar]
- 2.Gillison ML. Human papillomavirus-associated head and neck cancer is a distinct epidemiologic, clinical, and molecular entity. Semin Oncol. 2004;31(6):744–754. doi: 10.1053/j.seminoncol.2004.09.011. [DOI] [PubMed] [Google Scholar]
- 3.D'Souza G, Kreimer AR, Viscidi R, Pawlita M, Fakhry C, Koch WM, et al. Case-control study of human papillomavirus and oropharyngeal cancer. N Engl J Med. 2007;356(19):1944–1956. doi: 10.1056/NEJMoa065497. [DOI] [PubMed] [Google Scholar]
- 4.Hansson BG, Rosenquist K, Antonsson A, Wennerberg J, Schildt EB, Bladstrom A, et al. Strong association between infection with human papillomavirus and oral and oropharyngeal squamous cell carcinoma: A population-based case-control study in southern sweden. Acta Otolaryngol. 2005;125(12):1337–1344. doi: 10.1080/00016480510043945. [DOI] [PubMed] [Google Scholar]
- 5.Ryerson AB, Peters ES, Coughlin SS, Chen VW, Gillison ML, Reichman ME, et al. Burden of potentially human papillomavirus-associated cancers of the oropharynx and oral cavity in the US: 1998–2003. Cancer. 2008;113(10 Suppl):2901–2909. doi: 10.1002/cncr.23745. [DOI] [PubMed] [Google Scholar]
- 6.Nasman A, Attner P, Hammarstedt L, Du J, Eriksson M, Giraud G, et al. Incidence of human papillomavirus (HPV) positive tonsillar carcinoma in stockholm, sweden: An epidemic of viral-induced carcinoma? Int J Cancer. 2009;125(2):362–366. doi: 10.1002/ijc.24339. [DOI] [PubMed] [Google Scholar]
- 7.Attner P, Du J, Nasman A, Hammarstedt L, Ramqvist T, Lindholm J, et al. The role of human papillomavirus in the increased incidence of base of tongue cancer. Int J Cancer. 2010;126(12):2879–2884. doi: 10.1002/ijc.24994. [DOI] [PubMed] [Google Scholar]
- 8.Chaturvedi AK, Engels EA, Anderson WF, Gillison ML. Incidence trends for human papillomavirus-related and -unrelated oral squamous cell carcinomas in the united states. J Clin Oncol. 2008;26(4):612–619. doi: 10.1200/JCO.2007.14.1713. [DOI] [PubMed] [Google Scholar]
- 9.Sturgis EM, Cinciripini PM. Trends in head and neck cancer incidence in relation to smoking prevalence: An emerging epidemic of human papillomavirus-associated cancers? Cancer. 2007;110(7):1429–1435. doi: 10.1002/cncr.22963. [DOI] [PubMed] [Google Scholar]
- 10.Grulich AE, van Leeuwen MT, Falster MO, Vajdic CM. Incidence of cancers in people with HIV/AIDS compared with immunosuppressed transplant recipients: A meta-analysis. Lancet. 2007;370(9581):59–67. doi: 10.1016/S0140-6736(07)61050-2. [DOI] [PubMed] [Google Scholar]
- 11.Frisch M. Human papillomavirus-associated cancers in patients with human immunodeficiency virus infection and acquired immunodeficiency syndrome. J Natl Cancer Inst. 2000;92(18):1500–1510. doi: 10.1093/jnci/92.18.1500. [DOI] [PubMed] [Google Scholar]
- 12.Frisch M, Biggar RJ, Engels EA, Goedert JJ AIDS-Cancer Match Registry Study Group. Association of cancer with AIDS-related immunosuppression in adults. JAMA. 2001;285(13):1736–1745. doi: 10.1001/jama.285.13.1736. [DOI] [PubMed] [Google Scholar]
- 13.Patel P, Hanson DL, Sullivan PS, Novak RM, Moorman AC, Tong TC, et al. Incidence of types of cancer among HIV-infected persons compared with the general population in the united states: 1992–2003. Ann Intern Med. 2008;148(10):728–736. doi: 10.7326/0003-4819-148-10-200805200-00005. [DOI] [PubMed] [Google Scholar]
- 14.Gillison ML. Oropharyngeal cancer: A potential consequence of concomitant HPV and HIV infection. Curr Opin Oncol. 2009;21(5):439–444. doi: 10.1097/CCO.0b013e32832f3e1b. [DOI] [PubMed] [Google Scholar]
- 15.Kreimer AR, Bhatia RK, Messeguer AL, Gonzalez P, Herrero R, Giuliano AR. Oral human papillomavirus in healthy individuals: A systematic review of the literature. Sex Transm Dis. 2010;37(6):386–391. doi: 10.1097/OLQ.0b013e3181c94a3b. [DOI] [PubMed] [Google Scholar]
- 16.Cameron JE, Mercante D, O'Brien M, Gaffga AM, Leigh JE, Fidel PL, Jr, et al. The impact of highly active antiretroviral therapy and immunodeficiency on human papillomavirus infection of the oral cavity of human immunodeficiency virus-seropositive adults. Sex Transm Dis. 2005;32(11):703–709. doi: 10.1097/01.olq.0000175398.34610.2e. [DOI] [PubMed] [Google Scholar]
- 17.Fakhry C, D'souza G, Sugar E, Weber K, Goshu E, Minkoff H, et al. Relationship between prevalent oral and cervical human papillomavirus infections in human immunodeficiency virus-positive and -negative women. J Clin Microbiol. 2006;44(12):4479–4485. doi: 10.1128/JCM.01321-06. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 18.Fakhry C, Sugar E, D'Souza G, Gillison M. Two-week versus six-month sampling interval in a short-term natural history study of oral HPV infection in an HIV-positive cohort. PLoS One. 2010;5(7):e11918. doi: 10.1371/journal.pone.0011918. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 19.D'Souza G, Agrawal Y, J H, Bodison D, Gillison ML. Oral sexual behaviors associated with prevalent oral human papillomavirus (HPV) infection. Journal of Infectious Disease. 2009;199:1–7. doi: 10.1086/597755. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 20.Smith EM, Swarnavel S, Ritchie JM, Wang D, Haugen TH, Turek LP. Prevalence of human papillomavirus in the oral cavity/oropharynx in a large population of children and adolescents. Pediatr Infect Dis J. 2007;26(9):836–840. doi: 10.1097/INF.0b013e318124a4ae. [DOI] [PubMed] [Google Scholar]
- 21.Kreimer AR, Alberg AJ, Daniel R, Gravitt PE, Viscidi R, Garrett ES, et al. Oral human papillomavirus infection in adults is associated with sexual behavior and HIV serostatus. J Infect Dis. 2004;189(4):686–698. doi: 10.1086/381504. [DOI] [PubMed] [Google Scholar]
- 22.D'Souza G, Fakhry C, Sugar EA, Seaberg EC, Weber K, Minkoff HL, et al. Six-month natural history of oral versus cervical human papillomavirus infection. Int J Cancer. 2007;121(1):143–150. doi: 10.1002/ijc.22667. [DOI] [PubMed] [Google Scholar]
- 23.Greenspan D, Canchola AJ, MacPhail LA, Cheikh B, Greenspan JS. Effect of highly active antiretroviral therapy on frequency of oral warts. Lancet. 2001;357(9266):1411–1412. doi: 10.1016/S0140-6736(00)04578-5. [DOI] [PubMed] [Google Scholar]
- 24.Greenspan D, Gange SJ, Phelan JA, Navazesh M, Alves ME, MacPhail LA, et al. Incidence of oral lesions in HIV-1-infected women: Reduction with HAART. J Dent Res. 2004;83(2):145–150. doi: 10.1177/154405910408300212. [DOI] [PubMed] [Google Scholar]
- 25.Navazesh M, Mulligan R, Kono N, Kumar SK, Nowicki M, Alves M, et al. Oral and systemic health correlates of HIV-1 shedding in saliva. J Dent Res. 2010;89(10):1074–1079. doi: 10.1177/0022034510375290. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 26.Massad LS, Ahdieh L, Benning L, Minkoff H, Greenblatt RM, Watts H, et al. Evolution of cervical abnormalities among women with HIV-1: Evidence from surveillance cytology in the women's interagency HIV study. J Acquir Immune Defic Syndr. 2001;27(5):432–442. doi: 10.1097/00126334-200108150-00003. [DOI] [PubMed] [Google Scholar]
- 27.Strickler HD, Burk RD, Fazzari M, Anastos K, Minkoff H, Massad LS, et al. Natural history and possible reactivation of human papillomavirus in human immunodeficiency virus-positive women. J Natl Cancer Inst. 2005;97(8):577–586. doi: 10.1093/jnci/dji073. [DOI] [PubMed] [Google Scholar]
- 28.Barkan SE, Melnick SL, Preston-Martin S, Weber K, Kalish LA, Miotti P, et al. The women's interagency HIV study. WIHS collaborative study group. Epidemiology. 1998;9(2):117–125. [PubMed] [Google Scholar]
- 29.Bacon MC, von Wyl V, Alden C, Sharp G, Robison E, Hessol N, et al. The women's interagency HIV study: An observational cohort brings clinical sciences to the bench. Clinical and Vaccine Immunology. 2005;12(9):1013–1019. doi: 10.1128/CDLI.12.9.1013-1019.2005. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 30.Kaslow RA, Ostrow DG, Detels R, Phair JP, Polk BF, Rinaldo CR., Jr The multicenter AIDS cohort study: Rationale, organization, and selected characteristics of the participants. Am J Epidemiol. 1987;126(2):310–318. doi: 10.1093/aje/126.2.310. [DOI] [PubMed] [Google Scholar]
- 31.Dudley J, Jin S, Hoover D, Metz S, Thackeray R, Chmiel J. The multicenter AIDS cohort study: Retention after 9 1/2 years. Am J Epidemiol. 1995;142(No. 3):323–330. doi: 10.1093/oxfordjournals.aje.a117638. [DOI] [PubMed] [Google Scholar]
- 32.Silvestre AJ, Hylton JB, Johnson LM, Houston C, Witt M, Jacobson L, et al. Recruiting minority men who have sex with men for HIV research: Results from a 4-city campaign. Am J Public Health. 2006;96(6):1020–1027. doi: 10.2105/AJPH.2005.072801. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 33.D'Souza G, Sugar E, Ruby W, Gravitt P, Gillison M. Analysis of the effect of DNA purification on detection of human papillomavirus in oral rinse samples by PCR. J Clin Microbiol. 2005;43(11):5526–5535. doi: 10.1128/JCM.43.11.5526-5535.2005. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 34.Guidelines for the use of antiretroviral agents in HIV-1-infected adults and adolescents [Internet] Department of Health and Human Services. c2009 [updated 2009 Dec 1; cited 2010 Nov 24]. Available from: http://aidsinfonihgov/contentfiles/AdultandAdolescentGLpdf.
- 35.Broutian TR, He X, Gillison ML. Automated high throughput DNA isolation for detection of human papillomavirus in oral rinse samples. J Clin Virol. 2011;50(4):270–275. doi: 10.1016/j.jcv.2010.12.005. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 36.Cogliano V, Baan R, Straif K, Grosse Y, Secretan B, El Ghissassi F, et al. Carcinogenicity of human papillomaviruses. Lancet Oncol. 2005;6(4):204. doi: 10.1016/s1470-2045(05)70086-3. [DOI] [PubMed] [Google Scholar]
- 37.Schiffman M, Clifford G, Buonaguro FM. Classification of weakly carcinogenic human papillomavirus types: Addressing the limits of epidemiology at the borderline. Infect Agent Cancer. 2009;4:8. doi: 10.1186/1750-9378-4-8. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 38.Munoz N, Bosch FX, de Sanjose S, Herrero R, Castellsague X, Shah KV, et al. Epidemiologic classification of human papillomavirus types associated with cervical cancer. N Engl J Med. 2003;348(6):518–527. doi: 10.1056/NEJMoa021641. [DOI] [PubMed] [Google Scholar]
- 39.Xue X, Gange SJ, Zhong Y, Burk RD, Minkoff H, Massad LS, et al. Marginal and mixed-effects models in the analysis of human papillomavirus natural history data. Cancer Epidemiol Biomarkers Prev. 2010;19(1):159–169. doi: 10.1158/1055-9965.EPI-09-0546. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 40.Zeger SL, Liang KY, Albert PS. Models for longitudinal data: A generalized estimating equation approach. Biometrics. 1988;44(4):1049–1060. [PubMed] [Google Scholar]
- 41.Coutlee F, Trottier AM, Ghattas G, Leduc R, Toma E, Sanche G, et al. Risk factors for oral human papillomavirus in adults infected and not infected with human immunodeficiency virus. Sex Transm Dis. 1997;24(1):23–31. doi: 10.1097/00007435-199701000-00006. [DOI] [PubMed] [Google Scholar]
- 42.Herrero R. Human papillomavirus and oral cancer: The international agency for research on cancer multicenter study. CancerSpectrum Knowledge Environment. 2003;95(23):1772–1783. doi: 10.1093/jnci/djg107. [DOI] [PubMed] [Google Scholar]
- 43.Giovannelli L, Campisi G, Lama A, Giambalvo O, Osborn J, Margiotta V, et al. Human papillomavirus DNA in oral mucosal lesions. J Infect Dis. 2002;185(6):833–836. doi: 10.1086/339193. [DOI] [PubMed] [Google Scholar]
- 44.Smith EM, Ritchie JM, Summersgill KF, Hoffman HT, Wang DH, Haugen TH, et al. Human papillomavirus in oral exfoliated cells and risk of head and neck cancer. J Natl Cancer Inst. 2004;96(6):449–455. doi: 10.1093/jnci/djh074. [DOI] [PubMed] [Google Scholar]
- 45.Wilson TE, Massad LS, Riester KA, Barkan S, Richardson J, Young M, et al. Sexual, contraceptive, and drug use behaviors of women with HIV and those at high risk for infection: Results from the women's interagency. HIV study AIDS. 1999;13(5):591–598. doi: 10.1097/00002030-199904010-00008. [DOI] [PubMed] [Google Scholar]
- 46.Difranceisco W, Ostrow DG, Chmiel JS. Sexual adventurism, high-risk behavior, and human immunodeficiency virus-1 seroconversion among the chicago MACS-CCS cohort, 1984 to 1992. A case-control study Sex Transm Dis. 1996;23(6):453–460. doi: 10.1097/00007435-199611000-00003. [DOI] [PubMed] [Google Scholar]
- 47.Ahdieh L, Klein RS, Burk R, Cu-Uvin S, Schuman P, Duerr A, et al. Prevalence, incidence, and type-specific persistence of human papillomavirus in human immunodeficiency virus (HIV)-positive and HIV-negative women. J Infect Dis. 2001;184(6):682–690. doi: 10.1086/323081. [DOI] [PubMed] [Google Scholar]
- 48.Harris TG, Burk RD, Palefsky JM, Massad LS, Bang JY, Anastos K, et al. Incidence of cervical squamous intraepithelial lesions associated with HIV serostatus, CD4 cell counts, and human papillomavirus test results. JAMA. 2005;293(12):1471–1476. doi: 10.1001/jama.293.12.1471. [DOI] [PubMed] [Google Scholar]
- 49.Six C, Heard I, Bergeron C, Orth G, Poveda JD, Zagury P, et al. Comparative prevalence, incidence and short-term prognosis of cervical squamous intraepithelial lesions amongst HIV-positive and HIV-negative women. AIDS. 1998;12(9):1047–1056. [PubMed] [Google Scholar]
- 50.Durante AJ, Williams AB, Da Costa M, Darragh TM, Khoshnood K, Palefsky JM. Incidence of anal cytological abnormalities in a cohort of human immunodeficiency virus-infected women. Cancer Epidemiol Biomarkers Prev. 2003;12(7):638–642. [PubMed] [Google Scholar]
- 51.Strickler HD. Human papillomavirus type 16 and immune status in human immunodeficiency virus-seropositive women. CancerSpectrum Knowledge Environment. 2003;95(14):1062–1071. doi: 10.1093/jnci/95.14.1062. [DOI] [PubMed] [Google Scholar]
- 52.Smith JS, Lindsay L, Hoots B, Keys J, Franceschi S, Winer R, et al. Human papillomavirus type distribution in invasive cervical cancer and high-grade cervical lesions: A meta-analysis update. Int J Cancer. 2007;121(3):621–632. doi: 10.1002/ijc.22527. [DOI] [PubMed] [Google Scholar]
- 53.Kreimer AR, Villa A, Nyitray AG, Abrahamsen M, Papenfuss M, Smith D, et al. The epidemiology of oral HPV infection among a multinational sample of healthy men. Cancer Epidemiol Biomarkers Prev. 2011;20(1):172–182. doi: 10.1158/1055-9965.EPI-10-0682. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 54.Palefsky JM, Holly EA, Ralston ML, Jay N. Prevalence and risk factors for human papillomavirus infection of the anal canal in human immunodeficiency virus (HIV)-positive and HIV-negative homosexual men. J Infect Dis. 1998;177(2):361–367. doi: 10.1086/514194. [DOI] [PubMed] [Google Scholar]
- 55.de Pokomandy A, Rouleau D, Ghattas G, Vezina S, Cote P, Macleod J, et al. Prevalence, clearance, and incidence of anal human papillomavirus infection in HIV-infected men: The HIPVIRG cohort study. J Infect Dis. 2009;199(7):965–973. doi: 10.1086/597207. [DOI] [PubMed] [Google Scholar]
- 56.Garcia-Closas M, Egan KM, Abruzzo J, Newcomb PA, Titus-Ernstoff L, Franklin T, et al. Collection of genomic DNA from adults in epidemiological studies by buccal cytobrush and mouthwash. Cancer Epidemiol Biomarkers Prev. 2001;10(6):687–696. [PubMed] [Google Scholar]
- 57.Rogers NL, Cole SA, Lan HC, Crossa A, Demerath EW. New saliva DNA collection method compared to buccal cell collection techniques for epidemiological studies. Am J Hum Biol. 2007;19(3):319–326. doi: 10.1002/ajhb.20586. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 58.Heath EM, Morken NW, Campbell KA, Tkach D, Boyd EA, Strom DA. Use of buccal cells collected in mouthwash as a source of DNA for clinical testing. Arch Pathol Lab Med. 2001;125(1):127–133. doi: 10.5858/2001-125-0127-UOBCCI. [DOI] [PubMed] [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.