

Abstract
Background
Disrupted sleep rhythms may lead to cancer development. We conducted a population-based cohort study to evaluate the incidence and risk of prostate cancer in patients with sleep disorders (SDs).
Methods
Patients newly diagnosed with SDs between 2000 and 2010 were enrolled from the Taiwan Longitudinal Health Insurance Database. A non-SD cohort age-matched (5-y intervals), comorbidities, and medications was randomly sampled from the general population at a 1:1 ratio. The follow-up period extended from the index date of SDs to the diagnosis of prostate cancer, censoring, or the end of 2013. We used Cox proportional hazards models to calculate the risk of prostate cancer.
Results
In total, 41,444 patients were enrolled in each cohort. The mean age of the SD cohort was 48.0 years and that of the non-SD cohort was 47.8 years, with 58.2% of both cohorts aged younger than 50 years. The incidence of prostate cancer increased with age. The overall incidence of prostate cancer was higher in the SD cohort than in the non-SD cohort (9.56 vs 6.36 per 10,000 person-y), with an adjusted hazard ratio of 1.42 (95% CI = 1.20–1.69). Age-specific analysis revealed a 1.35-fold increased risk of prostate cancer in the patients aged ≥65 years in the SD cohort compared with the non-SD counterparts (95% CI = 1.10–1.65).
Conclusions
Patients with SDs are associated with increased risk of prostate cancer.
Keywords: Sleep disorders (SDs), Prostate cancer, Cohort study
Background
Sleep disorders (SDs) are one of the most common problems in the general population. The cause of SDs can be a primary disorder or secondary to various psychiatric and medical illnesses. The prevalence of SDs tends to increase with age. Approximately 41% of the elderly experienced difficulty initiating sleep onset insomnia, sleep maintaining insomnia, or early morning awakening insomnia. [1] Inadequate and nonrestorative sleep impairs quality of life and lead to future depression development and adverse health consequences. [2–5]
Previous studies have suggested that sleep disruption and circadian dysrhythmia may increase the risk of breast cancer in women. [6, 7] Melatonin, a pineal hormone, is related to circadian rhythm and sleep. [8] Recent studies have indicated that melatonin carries potentially chemopreventive, oncostatic, and anticarcinogenic effects. [9, 10] Prostate cancer has become a major public health issue in men worldwide, though the etiology of the disease remains elucidative. Two studies have reported that short sleep duration is associated with increased risk of prostate cancer. [11, 12] However, Markt et al. [13] conducted a prospective study and did not find association between sleep duration and risk of prostate cancer.
Prostate cancer is a leading cancer in men and causes a considerable economic and public health burden. [14] The incidence of prostate cancer has rapidly increased from 26.2 per 100,000 population in 2002 to 47.9 per 100,000 population in 2012 in Taiwan. [15] Employment with high job strain and stress might contribute to excess risk of prostate cancer. [16] The residents in urban areas may be associated with prostate cancer. [17] Adult obesity in the epidemiologic study showed association with development of prostate cancer. [18] Urinary stones may lead to obstruction, infection, and further cancer development. [19] A nested case-control study indicated an association between SDs and cancer. [20] People use hypnotics, mainly benzodiazepines and nonbenzodiazepine agents, to aid sleep or treat anxiety. However, hypnotic use may be related to increased cancer risk. [21] Therefore, we conducted a large population-based cohort study to investigate the risk of prostate cancer in patients with SDs compared with people without SDs after controlling for hypnotic use and potential covariates.
Methods
Data source
We conducted a retrospective population-based cohort study by using the Taiwan Longitudinal Health Insurance Database (LHID). The Taiwan government launched the National Health Insurance (NHI) program in 1995. Approximately 99% of the total population of approximately 23 million people, participate in the program. [22] The LHID is a sub-database of the National Health Insurance Research Database (NHIRD), which was established by the National Health Insurance Administration (NHIA) and is maintained by the National Health Research Institutes. The LHID contains the longitudinally linked data of 1,000,000 enrollees randomly sampled from the NHIRD. The LHID was released with de-identified data, rendering researchers unable to identify the study patients. Diseases in the database are coded according to the 2001 International Classification of Diseases, Ninth Revision, Clinical Modification (ICD-9-CM). The institutional review board (IRB) of China Medical University Hospital approved this study (IRB ID number: CMUH104-REC2–115).
Sampled patients
To evaluate the risk of prostate cancer in patients with SDs, we compared a SD cohort with a non-SD cohort. From the LHID, we selected male patients who received a first diagnosis of SDs (ICD-9-CM codes 307.4 including nonorganic sleep disorders, insomnia, and circadian rhythm SD, 327 organic sleep disorders, and 780.5 indicating sleep disturbance) between January 1, 2000 and December 31, 2010, and set the first diagnosis day of SDs as the index date. We assembled the non-SD cohort by randomly selecting male patients without a diagnosis of SDs from the LHID, and frequency-matched them with the SD cohort patients by age (5-y intervals), occupation, urbanization level, comorbidities, and medications at a 1:1 ratio. We set the index date of the matched cases as the index date for the non-SD patients. We enrolled only patients who were aged more than 20 years and who did not have a history of prostate cancer (ICD-9-CM code 185) before the index date.
Outcomes, occupation, urbanization level, comorbidities, and medication
All patients were followed until a diagnosis of prostate cancer, withdrawal from the NHI, death, or the end of 2011. We categorized the occupation variable into white collar (working with long indoor work hours, such as business and administration personnel), blue collar (working with long outdoor work hours, such as farmers and laborers), and others (primarily retired, unemployed, and low-income groups). The urbanization variable for the patients’ residing area was categorized into four levels: level 1 being the highest urbanization and level 4 being the least urbanization. We examined pre-existing comorbidities including hyperlipidemia (ICD-9-CM code 272), diabetes (ICD-9-CM code 250), hypertension (ICD-9-CM codes 401–405), urinary stones (ICD-9-CM codes 592.0. 592.1, 594.0, and 594.1), urinary tract infection (ICD-9-CM codes 590 and 595), obesity (ICD-9-CM code 278), anxiety (ICD-9-CM code 300.00), depression (ICD-9-CM codes 296.2, 296.3, 300.4, and 311), chronic obstructive pulmonary disease (COPD, ICD-9-CM codes 491, 492, 496), and alcohol-related illness(ICD-9-CM codes 291, 303, 305, 571.0, 571.1, 571.2, 571.3, 790.3, and V11.3). A medication history of hypnotics and antihypertensive medication use was included in the analysis. In addition, we also evaluated prostate specific antigen (PSA) screening in the study.
Statistical analysis
The demographic and clinical characteristics of the SD and non-SD cohorts, including age (≤ 49, 50–64, and ≥ 65y), occupation category (white collar, blue collar, and others), urbanization level, comorbidities, and medication treatments, were compared using the chi-squared test. For continuous variables, we conducted the Student t test to compare the SD and non-SD cohorts. We computed the incidence rate (per 10,000 person-y) of follow-up for each cohort. To evaluate the risk of prostate cancer for the SD cohort compared with the non-SD cohort, hazard ratios (HRs) and 95% confidence intervals (CIs) were estimated using univariable and multivariable Cox proportional hazards models. The multivariable models were simultaneously adjusted for age; occupation category; urbanization level; comorbidities of hyperlipidemia, diabetes, hypertension, urinary stones, urinary tract infection, obesity, anxiety, and depression; and medication of hypnotics as well as antihypertensive medication, and PSA screening. The cumulative incidence of prostate cancer was calculated using the Kaplan–Meier method and the difference was evaluated using the log-rank test. All analyses were conducted using SAS statistical software (Version 9.4 for Windows; SAS Institute, Inc., Cary, NC, USA), with statistical significance set at P < .05 for a 2-tailed test.
Results
The SD and non-SD cohorts each comprised 41,444 patients. The mean age of the SD cohort was 48.0 years and that of the non-SD cohort was 47.8 years, with 58.2% of both cohorts aged less than 50 years (Table 1). Most of the patients in both cohorts had white-collar jobs (54.3% vs 54.0%) and tended to reside in an urbanized area (59.6% vs 59.1%). The proportions of urinary tract infection and PSA screening in the SD cohort were significantly higher than those in the non-SD cohort.
Table 1.
Comparison of Demographics and Comorbidities of Patients With and Without SDs
| Sleep disorder (N = 41,444) | Control (N = 41,444) | P value | |||
|---|---|---|---|---|---|
| n | % | n | % | ||
| Age, year | 0.58 | ||||
| < 49 | 24,137 | 58.2 | 24,114 | 58.2 | |
| 50–64 | 9629 | 23.2 | 9597 | 23.2 | |
| ≥ 65 | 7701 | 18.6 | 7710 | 18.6 | |
| Mean (SD) # | 48.0 | 16.6 | 47.8 | 16.7 | 034 |
| Occupation | 0.65 | ||||
| White collar | 22,483 | 54.3 | 22,367 | 54.0 | |
| Blue collar | 14,250 | 34.4 | 14,377 | 34.7 | |
| Others‡ | 4711 | 11.4 | 4700 | 11.3 | |
| Urbanization level† | 0.22 | ||||
| 1 (highest) | 12,282 | 29.6 | 12,015 | 29.0 | |
| 2 | 12,417 | 30.0 | 12,472 | 30.1 | |
| 3 | 7350 | 17.7 | 7436 | 17.9 | |
| 4 (lowest) | 9395 | 22.7 | 9521 | 23.0 | |
| Comorbidity | |||||
| Hyperlipidemia | 7524 | 18.2 | 7630 | 18.4 | 0.34 |
| Diabetes | 2187 | 5.28 | 2238 | 5.40 | 0.43 |
| Hypertension | 12,345 | 29.8 | 12,459 | 30.1 | 0.39 |
| Urinary stones | 2770 | 6.68 | 2868 | 6.92 | 0.18 |
| Urinary tract infection | 3039 | 7.33 | 2796 | 6.75 | 0.001 |
| Obesity | 312 | 0.75 | 338 | 0.82 | 0.31 |
| Anxiety | 1775 | 4.28 | 1691 | 4.08 | 0.14 |
| Depression | 1187 | 2.86 | 1191 | 2.87 | 0.93 |
| COPD | 4939 | 11.9 | 5033 | 12.1 | 0.32 |
| Alcohol-related illness | 1573 | 3.80 | 1566 | 3.78 | 0.90 |
| Medication | |||||
| Hypnotics | 23,308 | 56.2 | 23,082 | 55.7 | 0.11 |
| Antihypertensives | 11,657 | 28.1 | 11,748 | 28.4 | 0.48 |
| PSA screening | 5729 | 13.8 | 4523 | 10.9 | < 0.001 |
Chi-square test compared to total SD; #:t test; COPD: Chronic obstructive pulmonary disease
†: The urbanization level was categorized into 4 levels according to the population density of the residential area, with level 1 indicating the highest urbanization and level 4 indicating the lowest urbanization
The overall incidence of prostate cancer was 51% greater in the SD cohort than in the non-SD cohort (9.56 vs 6.36 per 10,000 person-years), with an adjusted HR (aHR) of 1.42 (95% CI = 1.20–1.69) (Table 2). The cumulative incidence of prostate cancer was greater in the SD cohort than in the non-SD cohort (Fig. 1). Age-specific analysis revealed a significantly higher risk of developing prostate cancer in the patients all aged group in the SD cohort compared with the same age group in the non-SD cohort. Occupation category-specific analyses showed that among the patients employed in white-collar positions, those with SDs had a significantly higher risk of prostate cancer than did those without SDs (aHR = 1.67, 95% CI = 1.28–2.18). The SD cohort again exhibited a significantly higher risk of prostate cancer compared with the non-SD cohort when only the patients living in the 2nd highest (aHR = 1.43, 95% CI = 1.03–1.98), 3rd highest (aHR = 1.79, 95% CI = 1.11–2.91), and lowest (aHR = 1.42, 95% CI = 1.03–1.95 for lowest) urbanization level areas were considered. In patients without comorbidities, the risk of prostate cancer was 2.26-fold higher in the SD cohort than in the non-SD cohort (95% CI = 1.46–3.51). Among the patients not prescribed the examined medications, those with SDs had a higher risk of prostate cancer than did those without SDs (aHR = 1.46, 95% CI = 1.07–1.99 for those not prescribed hypnotics; aHR = 1.66, 95% CI = 1.26–2.19 for those not prescribed antihypertensive medication). In patients without PSA screening, the risk of prostate cancer was 1.58-fold higher in the SD cohort than in the non-SD cohort (95% CI = 1.26–1.98).
Table 2.
Comparison of Incidence Densities of Prostate Cancer Hazard Ratios of Men With and Without SDs Stratified by Demographic Characteristics and Comorbidities
| Sleep disorder | ||||||||
|---|---|---|---|---|---|---|---|---|
| Yes | No | |||||||
| Event | PY | Rate# | Event | PY | Rate# | Crude HR (95% CI) | Adjusted HR† (95% CI) | |
| All | 327 | 342,189 | 9.56 | 222 | 349,060 | 6.36 | 1.51(1.28, 1.80)*** | 1.42(1.20, 1.69)*** |
| Age | ||||||||
| < 49 | 14 | 208,908 | 0.67 | 4 | 214,073 | 0.19 | 3.82(1.26, 11.6)* | 3.12(1.02, 9.58)* |
| 50–64 | 94 | 79,239 | 11.9 | 58 | 81,376 | 7.13 | 1.70(1.23, 2.36)** | 1.50(1.08, 2.08)* |
| ≥ 65 | 219 | 54,042 | 40.5 | 160 | 53,610 | 29.8 | 1.36(1.11, 1.67)** | 1.35(1.10, 1.65)** |
| P for trend | 0.23 | |||||||
| Occupation | ||||||||
| White collar | 146 | 187,392 | 7.79 | 89 | 193,265 | 4.61 | 1.71(1.31, 2.23)*** | 1.67(1.28, 2.18)*** |
| Blue collar | 118 | 118,498 | 9.96 | 96 | 118,302 | 8.11 | 1.23(0.94, 1.61) | 1.14(0.87, 1.49) |
| Others‡ | 63 | 36,300 | 17.4 | 37 | 37,493 | 9.87 | 1.77(1.18, 2.66)** | 1.56(1.04, 2.36)* |
| P for trend | 0.06 | |||||||
| Urbanization level | ||||||||
| 1 (highest) | 97 | 99,276 | 9.77 | 74 | 104,986 | 7.05 | 1.40(1.04, 1.90)* | 1.30(0.96, 1.77) |
| 2 | 88 | 103,147 | 8.53 | 60 | 104,878 | 5.72 | 1.51(1.08, 2.09)* | 1.43(1.03, 1.98)* |
| 3 | 46 | 61,671 | 7.46 | 26 | 61,550 | 4.22 | 1.78(1.10, 2.88)* | 1.79(1.11, 2.91)* |
| 4 (lowest) | 96 | 78,094 | 12.3 | 62 | 77,646 | 7.98 | 1.55(1.12, 2.13)** | 1.42(1.03, 1.95)* |
| P for trend | 0.49 | |||||||
| Comorbidity‡ | ||||||||
| No | 66 | 171,700 | 3.84 | 29 | 178,753 | 1.62 | 2.43(1.57, 3.76)*** | 2.26(1.46, 3.51)*** |
| Yes | 261 | 170,489 | 15.3 | 193 | 170,307 | 11.3 | 1.36(1.13, 1.64)** | 1.30(1.08, 1.56)** |
| P for trend | 0.02 | |||||||
| Hyperlipidemia | ||||||||
| No | 221 | 281,496 | 7.85 | 141 | 288,143 | 4.89 | 1.62(1.31, 2.00)*** | 1.52(1.23, 1.88)*** |
| Yes | 106 | 60,693 | 17.5 | 81 | 60,918 | 13.3 | 1.32(0.99, 1.76) | 1.24(0.93, 1.66) |
| P for trend | 0.27 | |||||||
| Diabetes | ||||||||
| No | 288 | 326,577 | 8.82 | 188 | 333,506 | 5.64 | 1.58(1.31, 1.90)*** | 1.47(1.22, 1.77)*** |
| Yes | 39 | 15,611 | 25.0 | 34 | 15,555 | 21.9 | 1.14(0.72, 1.81) | 1.15(0.72, 1.82) |
| P for trend | 0.21 | |||||||
| Hypertension | ||||||||
| No | 132 | 245,636 | 5.37 | 70 | 253,208 | 2.76 | 1.99(1.49, 2.65)*** | 1.79(1.34, 2.40)*** |
| Yes | 195 | 96,553 | 20.2 | 152 | 95,853 | 15.9 | 1.27(1.03, 1.58)* | 1.24(1.00, 1.54)* |
| P for trend | 0.58 | |||||||
| Urinary stones | ||||||||
| No | 302 | 319,449 | 9.45 | 203 | 326,940 | 6.21 | 1.54(1.29, 1.83)*** | 1.45(1.21, 1.73)*** |
| Yes | 25 | 22,740 | 11.0 | 19 | 22,120 | 8.59 | 1.29(0.71, 2.34) | 1.26(0.69, 2.31) |
| P for trend | 0.60 | |||||||
| Urinary tract infection | ||||||||
| No | 290 | 321,203 | 9.03 | 197 | 330,283 | 5.96 | 1.53(1.27, 1.83)*** | 1.44(1.20, 1.73)*** |
| Yes | 37 | 20,986 | 17.6 | 25 | 18,777 | 13.3 | 1.33(0.80, 2.20) | 1.32(0.79, 2.20) |
| P for trend | 0.60 | |||||||
| Obesity | ||||||||
| No | 222 | 346,734 | 6.40 | 323 | 339,663 | 9.51 | 1.50(1.26, 1.78)*** | 1.40(1.18, 1.66)*** |
| Yes | 0 | 2326 | 0.00 | 4 | 2525 | 15.8 | – | – |
| P for trend | 0.95 | |||||||
| Anxiety | ||||||||
| No | 310 | 329,242 | 9.42 | 217 | 335,558 | 6.47 | 1.47(1.23, 1.75)*** | 1.39(1.17, 1.65)*** |
| Yes | 17 | 12,947 | 13.1 | 5 | 13,502 | 3.70 | 3.53(1.30, 9.58)* | 2.72(0.99, 7.48) |
| P for trend | 0.09 | |||||||
| Depression | ||||||||
| No | 317 | 332,890 | 9.52 | 216 | 339,164 | 6.37 | 1.51(1.27, 1.79)*** | 1.43(1.20, 1.70)*** |
| Yes | 10 | 9299 | 10.8 | 6 | 9897 | 6.06 | 1.82(0.66, 5.00) | 1.15(0.41, 3.28) |
| P for trend | 0.74 | |||||||
| COPD | ||||||||
| No | 233 | 304,824 | 7.64 | 156 | 313,361 | 4.98 | 1.55(1.27, 1.90)*** | 1.44(1.17, 1.76)*** |
| Yes | 94 | 37,365 | 25.2 | 66 | 35,699 | 18.5 | 1.36(0.99, 1.86) | 1.35(0.99, 1.85) |
| P for trend | 0.50 | |||||||
| Alcohol-related illness | ||||||||
| No | 318 | 331,360 | 9.60 | 217 | 338,475 | 6.41 | 1.51(1.27, 1.79)*** | 1.41(1.19, 1.68)*** |
| Yes | 9 | 10,829 | 8.31 | 5 | 10,585 | 4.72 | 1.74(0.58, 5.20) | 2.72(0.81, 9.11) |
| P for trend | 0.80 | |||||||
| Medication | ||||||||
| Hypnotics | ||||||||
| No | 97 | 143,651 | 6.75 | 68 | 142,627 | 4.77 | 1.42(1.04, 1.93)* | 1.46(1.07, 1.99)* |
| Yes | 230 | 198,538 | 11.6 | 154 | 206,434 | 7.46 | 1.57(1.28, 1.93)*** | 1.42(1.15, 1.74)*** |
| P for trend | 0.59 | |||||||
| Antihypertensives | ||||||||
| No | 140 | 252,468 | 5.55 | 82 | 260,095 | 3.15 | 1.79(1.36, 2.35)*** | 1.66(1.26, 2.19)*** |
| Yes | 187 | 89,721 | 20.8 | 140 | 88,966 | 15.7 | 1.33(1.07, 1.65)* | 1.28(1.02, 1.59)* |
| P for trend | 0.11 | |||||||
| PSA screening | ||||||||
| No | 193 | 289,171 | 6.67 | 126 | 305,769 | 4.12 | 1.60(1.28, 2.01)*** | 1.58(1.26, 1.98)*** |
| Yes | 134 | 53,018 | 25.3 | 96 | 43,292 | 22.2 | 1.18(0.91, 1.54) | 1.20(0.92, 1.56) |
| P for trend | 0.047 | |||||||
Rate#, incidence rate per 10,000 person-years; Crude HR, relative hazard ratio
Adjusted HR†: multivariable analysis with adjustment for age; occupation category; urbanization level; comorbidities of hyperlipidemia, diabetes, hypertension, urinary stones, urinary tract infection, obesity, anxiety, depression, chronic obstructive pulmonary disease, and alcohol-related illness, and medication of hypnotics as well as antihypertensive medication, and PSA screening; Comorbidity‡: Only one comorbidity (including hyperlipidemia, diabetes, hypertension, urinary stones, urinary tract infection, obesity, anxiety, and depression) classified as the comorbidity group
P < .05, **P < .01, ***P < .001
Fig. 1.
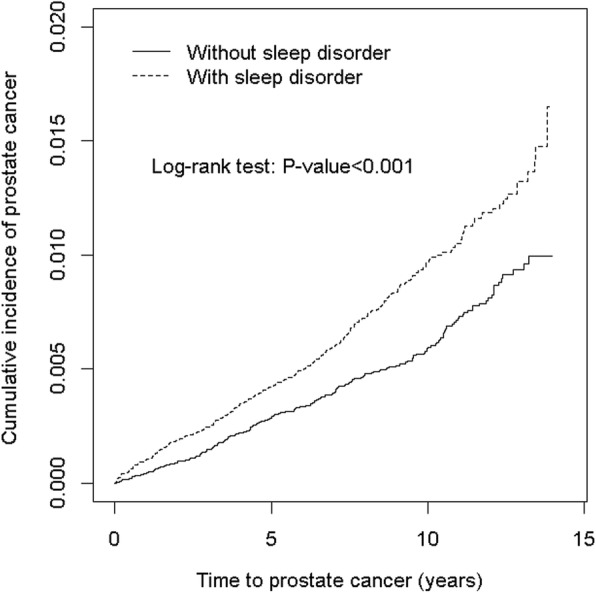
Comparison of Kaplan-Meir analysis-determined cumulative incidence of Prostate cancer of SD and non-SD cohorts
The analysis of HRs for developing prostate cancer was stratified by follow-up time. The SD cohort exhibited a significantly increased risk of prostate cancer compared with the non-SD cohort in follow-up time of ≤1 year (aHR = 2.46, 95% CI = 1.40–4.33) and > 5 years (aHR = 1.36, 95% CI = 1.07–1.73) (Table 3).
Table 3.
Trends of Prostate Cancer Risk Stratified by Follow-Up Years
| Sleep disorder | ||||||||
|---|---|---|---|---|---|---|---|---|
| Yes | No | |||||||
| Follow-up time, years | Event | PY | Rate# | Event | PY | Rate# | Crude HR (95% CI) | Adjusted HR† |
| (95% CI) | ||||||||
| ≤1 | 42 | 41,067 | 10.2 | 17 | 41,066 | 4.14 | 2.47(1.41, 4.34)** | 2.46(1.40, 4.33)** |
| 2–3 | 58 | 79,920 | 7.26 | 42 | 79,951 | 5.25 | 1.38(0.93, 2.06) | 1.37(0.92, 2.03) |
| 4–5 | 65 | 72,438 | 8.97 | 52 | 72,465 | 7.18 | 1.25(0.87, 1.80) | 1.20(0.83, 1.73) |
| > 5 | 162 | 148,765 | 10.9 | 111 | 155,578 | 7.13 | 1.54(1.21, 1.96)*** | 1.36(1.07, 1.73)*** |
Rate#, incidence rate per 10,000 person-years; Crude HR, relative hazard ratio
Adjusted HR†: multivariable analysis with adjustment for age; occupation category; urbanization level; comorbidities of hyperlipidemia, diabetes, hypertension, urinary stones, urinary tract infection, obesity, anxiety, depression, chronic obstructive pulmonary disease, and alcohol-related illness,; and medication of hypnotics as well as antihypertensive medication, and PSA screening
*P < .05, **P < .01
The risk of developing prostate cancer increased with age (aHR = 1.10, 95% CI = 1.09–1.11 every 1 y). Compared to patient of others occupation, patients of white collar occupation had a higher risk of developing prostate cancer (aHR = 1.36, 95% CI = 1.06–1.74). The risk of developing prostate cancer was greater for patients with comorbidities of hyperlipidemia (aHR = 1.36, 95% CI = 1.13–1.64), diabetes (aHR = 1.36, 95% CI = 1.06–1.76), and PSA screening (aHR = 1.99, 95% CI = 1.67–2.36) (Table 4).
Table 4.
HR of Prostate Cancer in Association with Sex, Age, Occupation, Urbanization level, Comorbidities, and Medication in Univariable and Multivariable Cox Regression Models
| Variable | Crude | Adjusted† | ||
|---|---|---|---|---|
| HR | (95% CI) | HR | (95% CI) | |
| Sleep disorder | 1.51 | (1.28, 1.80)*** | 1.42 | (1.20, 1.69)*** |
| Age, year | 1.10 | (1.09, 1.11)*** | 1.10 | (1.09, 1.11)*** |
| Occupation | ||||
| White collar | 1.00 | (Reference) | 1.36 | (1.06, 1.74)* |
| Blue collar | 1.46 | (1.22, 1.76)*** | 1.28 | (0.99, 1.65) |
| Others‡ | 2.21 | (1.75, 2.79)*** | 1.00 | (Reference) |
| Urbanization level† | ||||
| 1 (highest) | 1.43 | (1.09, 1.89)* | 1.31 | (0.99,1 .72) |
| 2 | 1.22 | (0.92, 1.61) | 1.16 | (0.88, 1.54) |
| 3 | 1.00 | (Reference) | 1.00 | (Reference) |
| 4 (lowest) | 1.73 | (1.31, 2.29)*** | 1.25 | (0.94, 1.66) |
| Comorbidity | ||||
| Hyperlipidemia | 2.44 | (2.05, 2.91)*** | 1.36 | (1.13, 1.64)*** |
| Diabetes | 3.32 | (2.59, 4.24)*** | 1.36 | (1.06, 1.76)* |
| Hypertension | 4.49 | (3.77, 5.34)*** | 0.94 | (0.75, 1.18) |
| Urinary stones | 1.28 | (0.94, 1.74) | ||
| Urinary tract infection | 2.17 | (1.66, 2.83)*** | 1.07 | (0.82, 1.40) |
| Obesity | 1.07 | (0.40, 2.87) | ||
| Anxiety | 1.07 | (0.70, 1.65) | ||
| Depression | 1.05 | (0.64, 1.73) | ||
| COPD | 3.54 | (2.95, 4.26)*** | 1.03 | (0.85, 1.25) |
| Alcohol-related illness | 0.85 | (0.50, 1.45) | ||
| Medication | ||||
| Hypnotics | 1.60 | (1.33, 1.92)*** | 0.83 | (0.69, 1.00) |
| Antihypertensives | 4.29 | (3.61, 5.08)*** | 1.17 | (0.94, 1.46) |
| PSA screening | 4.38 | (3.69, 5.19)*** | 1.99 | (1.67, 2.36)*** |
Crude HR, relative hazard ratio; Adjusted HR†: multivariable analysis with adjustment for age; occupation category; urbanization level; comorbidities of hyperlipidemia, diabetes, hypertension, urinary stones, urinary tract infection, and COPD, and medication of hypnotics as well as antihypertensive medication, and PSA screening; COPD: chronic obstructive pulmonary disease
*p < 0.05, **p < 0.01, ***p < 0.001
Discussion
Previous studies have focused on the impact of night shift work and circadian rhythm disorders on cancer risks. [23, 24] We investigated the incidence and risk of prostate cancer in patients with SDs in an Asian population-based cohort study. Our study showed that the men with SDs displayed a greater incidence of prostate cancer than did the men without SDs (9.56 vs 6.36 per 10,000 person-y). The incidence of prostate cancer in our SD cohort was higher than that (4.79 per 10,000) in Taiwan Cancer Registry Database in 2012. [15] The possible reason may be related to considerable comorbidities and poor sleep quality in our SD cohort. [4, 5] Despite we assembled the non-SD cohort by randomly frequency-matched age, age (5-y intervals), occupation, urbanization level, comorbidities, and medications, the proportion of urinary tract infection and PSA screening were higher in the SD cohort than in the non-SD cohort. After adjustment for age, comorbidities, medication, and PSA screening, the men in the SD cohort still had a 1.42-fold increased risk of prostate cancer compared with the men in the non-SD cohort.
The incidence and risk of prostate cancer in our study were different from AGES-Reykjavik cohort study, which used questionnaires to investigate 2012 older men with sleep problems in Iceland and found that 135 of them (6.4%) were diagnosed with prostate cancer during follow-up. [12] However, Sigurdardottir et al. did not evaluate the effect of demographics, comorbidities, and hypnotic use.
The possible biological mechanism of SDs being associated with increased prostate cancer risk remains unclear. Men with reported sleep problems had lower morning levels of urinary 6-sulfatoxymelatonin, which are associated with increased risk of prostate cancer. [25] The 6-sulfatoxymelatonin in urine is the major enzymatic metabolite of melatonin. Melatonin has been observed to inhibit cancer development and growth in both in vitro and in vivo experimental models. [10, 26] Kao et al. indicated that hypnotics may relate to risk of prostate cancer. [27] We found the incidence of prostate cancer higher in patients with hypnotic use than that in patients without hypnotic use. However, the use of hypnotics was not an independent risk factor of prostate cancer in the multivariable Cox regression model.
A reciprocal interaction and regulation between sleep and the immune system exists. A lack of sleep can lead to immune suppression and activate cancer-stimulatory cytokines. [28–30] Studies have reported that patients with SDs are associated with unhealthy habits including excessive alcohol consumption and smoking, which are related to prostate cancer risk. [31–34] COPD is strongly correlated with smoking. [35] We used COPD and alcohol-related illness to evaluate smoking and alcohol consumption habits. The SD cohort exhibited significantly higher proportion of COPD and alcohol-related illness than did the non-SD cohort.
The incidence and risk of prostate cancer increased exponentially with age, which finding was consistent with previous reports. [36] Among men in white-collar employment, those with SDs exhibited a substantially higher risk of developing prostate cancer compared with those without SDs. Insomnia may be considered as a clinical marker of high job strain for white-collar workers. [37] White-collar workers experiencing occupational stress may present SDs. High job strain and stress might contribute to excess risk of prostate cancer. [38] The men who resided in the highest urbanization areas exhibited significantly increased risks of prostate cancer compared with the controls residing in the lowest urbanization areas. These epiphenomena may be associated with stress-related insomnia implicated in cancer development and progression. [16, 39, 40]
Several limitations should be considered when interpreting our results. First, the LHID does not provide detailed patient information such as smoking and alcohol consumption, which may be potential confounding factors for this study. Evidence shows that hypertension, diabetes, and COPD are associated with smoking. [41, 42] Therefore, we adjusted for hypertension, diabetes, and COPD to minimize the smoking confounder. Second, lack of time-varying approach may result in misclassification of exposure. The effect of SD on the risk of prostate cancer may be underestimated because non-SD controls may experience SD before diagnosis of prostate cancer.
The strength of the study lies in the use of a large population-based sample with a longitudinal cohort design. The diagnoses of SDs were made by physicians instead of self-reported in a questionnaire survey. Researchers using the LHID can track patients throughout a study period because the NHIA is the single payer for the NHI program in Taiwan and all beneficiaries are assigned unique identification numbers. The NHIA routinely examines the validity of the reimbursement claims data through administrative and peer-review processes.
Conclusion
We found that patients with SDs are associated with increased prostate cancer risk, which increases with age. Therefore, appropriately managing sleep problems is a crucial healthcare concern, particularly as the number of people with SDs is increasing.
Acknowledgements
We acknowledged Sunny Chung for providing novel idea and editing this manuscript.
Funding
This work was partly supported by grants from the Taiwan Ministry of Health and Welfare Clinical Trial and Research Center for Excellence (MOHW104-TDU-B-212-113002). The funders did not have a role in study design, data collection and analysis, preparation of the manuscript, and publication.
Availability of data and materials
The datasets used and/or analysed during the current study are available from the corresponding author on reasonable request
Abbreviations
- aHR
Adjusted hazard ratio
- CIs
Confidence intervals
- COPD
Chronic obstructive pulmonary disease
- HRs
Hazard ratios
- ICD-9-CM
International Classification of Diseases, Ninth Revision, Clinical Modification
- IRB
Institutional review board
- LHID
Longitudinal Health Insurance Database
- NHI
National Health Insurance
- NHIA
National Health Insurance Administration
- NHIRD
National Health Insurance Research Database
- PSA
Prostate specific antigen
- SDs
Sleep disorders
Authors’ contributions
All authors have contributed significantly, and that all authors are in agreement with the content of the manuscript: Conception/Design: WSC; Collection and data assembly: all authors; Data analysis and interpretation: all authors; Manuscript writing: all authors; Final approval of manuscript: all authors.
Ethics approval and consent to participate
The institutional review board (IRB) of China Medical University Hospital approved this study (IRB ID number: CMUH104-REC2–115). Informed consent for the study participants were waived by the IRB because the study participants were deidentified in the Taiwan Longitudinal Health Insurance Database.
Consent for publication
Not applicable.
Competing interests
The authors declare that they have no competing interests.
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Contributor Information
Wei-Sheng Chung, Phone: 886-4-22294411, Email: chung.w53@msa.hinet.net, Email: albertchung5325@gmail.com.
Cheng-Li Lin, Email: orangechengli@gmail.com.
References
- 1.Tsou MT. Prevalence and risk factors for insomnia in community-dwelling elderly in northern Taiwan. J Clin Gerontol Geriatr. 2013;4(3):75–79. doi: 10.1016/j.jcgg.2013.02.002. [DOI] [Google Scholar]
- 2.Baglioni C, Battagliese G, Feige B, Spiegelhalder K, Nissen C, Voderholzer U, Lombardo C, Riemann D. Insomnia as a predictor of depression: a meta-analytic evaluation of longitudinal epidemiological studies. J Affect Disord. 2011;135(1–3):10–19. doi: 10.1016/j.jad.2011.01.011. [DOI] [PubMed] [Google Scholar]
- 3.Chung WS, Lin CL, Chen YF, Chiang JY, Sung FC, Chang YJ, Kao CH. Sleep disorders and increased risk of subsequent acute coronary syndrome in individuals without sleep apnea: a nationwide population-based cohort study. Sleep. 2013;36(12):1963–1968. doi: 10.5665/sleep.3240. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 4.Chung WS, Chen YF, Lin CL, Chang SN, Hsu WH, Kao CH. Sleep disorders increase the risk of venous thromboembolism in individuals without sleep apnea: a nationwide population-based cohort study in Taiwan. Sleep Med. 2015;16(1):168–172. doi: 10.1016/j.sleep.2014.07.031. [DOI] [PubMed] [Google Scholar]
- 5.Chung WS, Lin HH, Cheng NC. The incidence and risk of herpes zoster in patients with sleep disorders: a population-based cohort study. Medicine. 2016;95(11):e2195. doi: 10.1097/MD.0000000000002195. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 6.Hansen J. Light at night, shiftwork, and breast cancer risk. J Natl Cancer Inst. 2001;93(20):1513–1515. doi: 10.1093/jnci/93.20.1513. [DOI] [PubMed] [Google Scholar]
- 7.Davis S, Mirick DK. Circadian disruption, shift work and the risk of cancer: a summary of the evidence and studies in Seattle. Cancer Causes Control. 2006;17(4):539–545. doi: 10.1007/s10552-005-9010-9. [DOI] [PubMed] [Google Scholar]
- 8.Turek FW, Gillette MU. Melatonin, sleep, and circadian rhythms: rationale for development of specific melatonin agonists. Sleep Med. 2004;5(6):523–532. doi: 10.1016/j.sleep.2004.07.009. [DOI] [PubMed] [Google Scholar]
- 9.Sanchez-Barcelo EJ, Mediavilla MD, Alonso-Gonzalez C, Reiter RJ. Melatonin uses in oncology: breast cancer prevention and reduction of the side effects of chemotherapy and radiation. Expert Opin Investig Drugs. 2012;21(6):819–831. doi: 10.1517/13543784.2012.681045. [DOI] [PubMed] [Google Scholar]
- 10.Jung B, Ahmad N. Melatonin in cancer management: progress and promise. Cancer Res. 2006;66(20):9789–9793. doi: 10.1158/0008-5472.CAN-06-1776. [DOI] [PubMed] [Google Scholar]
- 11.Gapstur SM, Diver WR, Stevens VL, Carter BD, Teras LR, Jacobs EJ. Work schedule, sleep duration, insomnia, and risk of fatal prostate cancer. Am J Prev Med. 2014;46(3 Suppl 1):S26–S33. doi: 10.1016/j.amepre.2013.10.033. [DOI] [PubMed] [Google Scholar]
- 12.Sigurdardottir LG, Valdimarsdottir UA, Mucci LA, Fall K, Rider JR, Schernhammer E, Czeisler CA, Launer L, Harris T, Stampfer MJ, et al. Sleep disruption among older men and risk of prostate cancer. Cancer epidemiology, biomarkers & prevention : a publication of the American Association for Cancer Research, cosponsored by the American Society of Preventive Oncology. 2013;22(5):872–879. doi: 10.1158/1055-9965.EPI-12-1227-T. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 13.Markt SC, Flynn-Evans EE, Valdimarsdottir UA, Sigurdardottir LG, Tamimi RM, Batista JL, Haneuse S, Lockley SW, Stampfer M, Wilson KM, et al. Sleep duration and disruption and prostate Cancer risk: a 23-year prospective study. Cancer epidemiology, biomarkers & prevention : a publication of the American Association for Cancer Research, cosponsored by the American Society of Preventive Oncology. 2016;25(2):302–308. doi: 10.1158/1055-9965.EPI-14-1274. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 14.Wong MC, Goggins WB, Wang HH, Fung FD, Leung C, Wong SY, Ng CF, Sung JJ. Global incidence and mortality for prostate Cancer: analysis of temporal patterns and trends in 36 countries. Eur Urol. 2016;70(5):862–874. doi: 10.1016/j.eururo.2016.05.043. [DOI] [PubMed] [Google Scholar]
- 15.Chiang CJ, Lo WC, Yang YW, You SL, Chen CJ, Lai MS. Incidence and survival of adult cancer patients in Taiwan, 2002-2012. Journal of the Formosan Medical Association = Taiwan yi zhi. 2016;115(12):1076–1088. doi: 10.1016/j.jfma.2015.10.011. [DOI] [PubMed] [Google Scholar]
- 16.Segerstrom SC, Miller GE. Psychological stress and the human immune system: a meta-analytic study of 30 years of inquiry. Psychol Bull. 2004;130(4):601–630. doi: 10.1037/0033-2909.130.4.601. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 17.Sharp L, Donnelly D, Hegarty A, Carsin AE, Deady S, McCluskey N, Gavin A, Comber H. Risk of several cancers is higher in urban areas after adjusting for socioeconomic status. Results from a two-country population-based study of 18 common cancers. Journal of urban health : bulletin of the New York Academy of Medicine. 2014;91(3):510–525. doi: 10.1007/s11524-013-9846-3. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 18.Engeland A, Tretli S, Bjorge T. Height, body mass index, and prostate cancer: a follow-up of 950000 Norwegian men. Br J Cancer. 2003;89(7):1237–1242. doi: 10.1038/sj.bjc.6601206. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 19.Shih CJ, Chen YT, Ou SM, Yang WC, Chen TJ, Tarng DC. Urinary calculi and risk of cancer: a nationwide population-based study. Medicine. 2014;93(29):e342. doi: 10.1097/MD.0000000000000342. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 20.Fang HF, Miao NF, Chen CD, Sithole T, Chung MH. Risk of Cancer in patients with insomnia, parasomnia, and obstructive sleep apnea: a Nationwide nested case-control study. J Cancer. 2015;6(11):1140–1147. doi: 10.7150/jca.12490. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 21.Iqbal U, Nguyen PA, Syed-Abdul S, Yang HC, Huang CW, Jian WS, Hsu MH, Yen Y, Li YC. Is long-term use of benzodiazepine a risk for cancer? Medicine. 2015;94(6):e483. doi: 10.1097/MD.0000000000000483. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 22.NHI: National Health Insurance Database. In.: National Health Insurance Administration; 2015.
- 23.Kubo T, Oyama I, Nakamura T, Kunimoto M, Kadowaki K, Otomo H, Fujino Y, Fujimoto N, Matsumoto T, Matsuda S. Industry-based retrospective cohort study of the risk of prostate cancer among rotating-shift workers. Int J Urol. 2011;18(3):206–211. doi: 10.1111/j.1442-2042.2010.02714.x. [DOI] [PubMed] [Google Scholar]
- 24.Parent ME, El-Zein M, Rousseau MC, Pintos J, Siemiatycki J. Night work and the risk of cancer among men. Am J Epidemiol. 2012;176(9):751–759. doi: 10.1093/aje/kws318. [DOI] [PubMed] [Google Scholar]
- 25.Sigurdardottir LG, Markt SC, Rider JR, Haneuse S, Fall K, Schernhammer ES, Tamimi RM, Flynn-Evans E, Batista JL, Launer L, et al. Urinary melatonin levels, sleep disruption, and risk of prostate cancer in elderly men. Eur Urol. 2015;67(2):191–194. doi: 10.1016/j.eururo.2014.07.008. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 26.Cutando A, Lopez-Valverde A, Arias-Santiago S, DE Vicente J, DE Diego RG. Role of melatonin in cancer treatment. Anticancer Res. 2012;32(7):2747–2753. [PubMed] [Google Scholar]
- 27.Kao CH, Sun LM, Su KP, Chang SN, Sung FC, Muo CH, Liang JA. Benzodiazepine use possibly increases cancer risk: a population-based retrospective cohort study in Taiwan. The Journal of clinical psychiatry. 2012;73(4):e555–e560. doi: 10.4088/JCP.11m07333. [DOI] [PubMed] [Google Scholar]
- 28.Dimitrov S, Lange T, Tieken S, Fehm HL, Born J. Sleep associated regulation of T helper 1/T helper 2 cytokine balance in humans. Brain Behav Immun. 2004;18(4):341–348. doi: 10.1016/j.bbi.2003.08.004. [DOI] [PubMed] [Google Scholar]
- 29.Blask DE. Melatonin, sleep disturbance and cancer risk. Sleep Med Rev. 2009;13(4):257–264. doi: 10.1016/j.smrv.2008.07.007. [DOI] [PubMed] [Google Scholar]
- 30.Besedovsky L, Lange T, Born J. Sleep and immune function. Pflugers Arch. 2012;463(1):121–137. doi: 10.1007/s00424-011-1044-0. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 31.Crum RM, Storr CL, Chan YF, Ford DE. Sleep disturbance and risk for alcohol-related problems. Am J Psychiatry. 2004;161(7):1197–1203. doi: 10.1176/appi.ajp.161.7.1197. [DOI] [PubMed] [Google Scholar]
- 32.Phillips BA, Danner FJ. Cigarette smoking and sleep disturbance. Arch Intern Med. 1995;155(7):734–737. doi: 10.1001/archinte.1995.00430070088011. [DOI] [PubMed] [Google Scholar]
- 33.Velicer CM, Kristal A, White E. Alcohol use and the risk of prostate cancer: results from the VITAL cohort study. Nutr Cancer. 2006;56(1):50–56. doi: 10.1207/s15327914nc5601_7. [DOI] [PubMed] [Google Scholar]
- 34.Huncharek M, Haddock KS, Reid R, Kupelnick B. Smoking as a risk factor for prostate cancer: a meta-analysis of 24 prospective cohort studies. Am J Public Health. 2010;100(4):693–701. doi: 10.2105/AJPH.2008.150508. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 35.Laniado-Laborin R. Smoking and chronic obstructive pulmonary disease (COPD). Parallel epidemics of the 21 century. Int J Environ Res Public Health. 2009;6(1):209–224. doi: 10.3390/ijerph6010209. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 36.Lin WY, Chang YH, Lin CL, Kao CH, Wu HC. Erectile dysfunction and the risk of prostate cancer. Oncotarget. 2017;8(32):52690–52698. doi: 10.18632/oncotarget.17082. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 37.Metlaine A, Sauvet F, Gomez-Merino D, Elbaz M, Delafosse JY, Leger D, Chennaoui M. Association between insomnia symptoms, job strain and burnout syndrome: a cross-sectional survey of 1300 financial workers. BMJ Open. 2017;7(1):e012816. doi: 10.1136/bmjopen-2016-012816. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 38.Blanc-Lapierre A, Rousseau MC, Parent ME. Perceived workplace stress is associated with an increased risk of prostate Cancer before age 65. Front Oncol. 2017. [DOI] [PMC free article] [PubMed]
- 39.Lutgendorf SK, Sood AK, Antoni MH. Host factors and cancer progression: biobehavioral signaling pathways and interventions. J Clin Oncol. 2010;28(26):4094–4099. doi: 10.1200/JCO.2009.26.9357. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 40.Antonova L, Aronson K, Mueller CR. Stress and breast cancer: from epidemiology to molecular biology. Breast Cancer Res. 2011;13(2):208. doi: 10.1186/bcr2836. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 41.Virdis A, Giannarelli C, Neves MF, Taddei S, Ghiadoni L. Cigarette smoking and hypertension. Curr Pharm Des. 2010;16(23):2518–2525. doi: 10.2174/138161210792062920. [DOI] [PubMed] [Google Scholar]
- 42.Chang SA. Smoking and type 2 diabetes mellitus. Diabetes Metab J. 2012;36(6):399–403. doi: 10.4093/dmj.2012.36.6.399. [DOI] [PMC free article] [PubMed] [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.
Data Availability Statement
The datasets used and/or analysed during the current study are available from the corresponding author on reasonable request