

Abstract
Background
Abdominal obesity predicts a wide range of adverse health outcomes. Over the past several decades, prevalence of abdominal obesity has increased markedly in industrialized countries like the U.S. No previous analyses, however, have evaluated whether there are birth cohort effects for abdominal obesity. Estimating cohort effects is necessary to forecast future health trends and understand past population-level trends.
Methods
This analysis evaluated whether there were birth cohort effects for abdominal obesity for the Silent Generation (born 1925-1945), children of the Great Depression; Baby Boomers (born 1946-1964); or Generation X (born 1965-1980). Cohort effects for prevalence of abdominal obesity were estimated using the median polish method with data collected from the National Health and Nutrition Examination Survey between 1988 and 2008. Respondents were aged 20-74 years.
Results
After taking into account age effects and ubiquitous secular changes, the Silent Generation and Generation X had higher cohort-specific prevalence of abdominal obesity than the Baby Boomers. Effects were more pronounced in women than men.
Conclusions
This work presents a novel finding: evidence that the birth cohorts of the post-World War II Baby Boom appeared to have uniquely low cohort effects on abdominal obesity. The growing prosperity of the post-World-War II U.S. may have exposed the Baby Boom generation to lower levels of psychosocial and socioeconomic stress than previous or subsequent generations. By identifying factors associated with the Baby Boomers’ low cohort-specific sensitivity to the obesogenic environment, the obesity prevention community can identify early-life factors that can protect future generations from excess weight gain.
Keywords: age-period-cohort, obesity, abdominal obesity, demography, sex differences, United States
INTRODUCTION
Age-period-cohort analyses can help evaluate causes of past population-level health trends, predict future health trends, and illuminate causes of individual-level susceptibility to health outcomes. All previous age-period-cohort analysis of obesity examined obesity assessed by body mass index (BMI). This measure of overall obesity is associated with risk of many chronic diseases. However, alternate measures of obesity bear a more direct relationship to chronic disease risk.
In particular, high waist circumference, which we refer to as “abdominal obesity,” predicts chronic diseases, such as type 2 diabetes and cardiovascular disease, better than obesity assessed by BMI.1, 2 Abdominal obesity is highly correlated with total body fat.3 Further, abdominal obesity may more specifically indicate increased amounts of intra-abdominal visceral fat and subcutaneous abdominal fat, which affect hepatic metabolism of insulin and inflammatory markers.4 Moreover, in the U.S., abdominal obesity increased continuously in the 1990s and 2000s and is now present in more than half of U.S. adults.2
This analysis evaluated whether there were cohort effects for abdominal obesity for the Silent Generation (born 1925-1945), children of the Great Depression; Baby Boomers (born 1946-1964); or Generation X (born 1965-1980).5 These particular birth cohorts were examined because it is unclear whether cohort effects increased monotonically throughout the 20th century.
If cohort effects did increase monotonically, increasing prosperity and technology are implicated as major causes of cohort-specific risk.6, 7 One alternative theory draws upon the growing field of developmental origins of health and disease (DOHaD). DOHaD implicates stress, poverty, and poor intrauterine conditions as influences on lifelong cohort specific risk of obesity.8 These factors did not necessarily increase monotonically throughout the 20th century, nor did they affect women and men similarly. Therefore, this analysis will estimate cohort-specific risks for abdominal obesity among 20th-century cohorts of men and women.
METHODS
Sample
This analysis uses data from the National Health and Nutrition Examination Survey (NHANES), a nationally representative sample of the US civilian non-institutionalized population.9-11 The analysis included survey waves conducted between 1988 and 2008: NHANES III, phase 1 (1988-1991), NHANES III, phase 2 (1991-1994), and the continuous surveys (1999-2008) that have been released in two-year increments since 1999. NHANES uses a complex, stratified, multi-stage probability cluster sampling design. The analysis included survey weights in all analyses to correct for oversampling and non-response.12
The dataset was limited to individuals aged 20-74 years who were born in the United States. Those under the age of 20 years were excluded because definitions of excessive waist circumference are not available for children and adolescents.13. Foreign-born respondents were omitted because years spent in another country before immigration violate the age-period-cohort method’s assumption that individuals shared period and birth cohort exposures across their lifespans.14, 15 Respondents missing waist circumference (n=1 348; 4.7%) or pregnant when measured (n=970; 3.6%) were excluded. The final sample included 27 159 individuals.
Measures
Abdominal obesity was assessed using measured waist circumference and defined as ≥88 cm for women and ≥102 cm for men.13 For context, analyses were also performed of obesity assessed using body mass index (BMI). This alternative obesity measure was assessed using body mass index calculated from measured height and weight and defined as BMI ≥30.0 kg/m2.16 Age and sex were self-reported by respondents. The cutpoints for BMI and waist circumference correspond to clinically meaningful measures of obesity.
Analysis
Age-period-cohort analysis is a family of models that uses information on respondent age, time period of observation, and birth cohort to track the prevalence of health outcomes over time. These models generally aim to identify age effects (the distribution of an outcome across the lifespan), period effects (secular trends in the prevalence of an outcome that are evident among all age groups in the population), and birth cohort effects (the concentration of the outcome among individuals who were born in or around the same year). Cohort effects can reflect secular variation in an environmental exposure whose effects vary across age or stages of the lifecourse.17 Therefore, cohort effects are sometimes conceptualized as an interaction of period and age effects.18-20
Age, period, and cohort effects can be estimated using a variety of statistical techniques.21, 22 For the present analysis we utilized the median polish technique.23 The median polish approach operationalizes cohort effects as interaction of period and age effects.18, 20, 24 To implement the median polish technique, we first created an 11 × 5 contingency table of obesity prevalence. The 11 rows represent 11 5-year age groups, while the five columns denote five 5-year blocks of calendar time (Figure 1). Each diagonal represents one of 15 birth cohorts; different blocks in the same diagonal show the different ages and calendar times at which the cohort is observed. Before 1999, NHANES assessed obesity prevalence during periods of variable timing and duration. Therefore, five synthetic 5-year period categories were approximated using the NHANES data (Figure 1).
Figure 1.
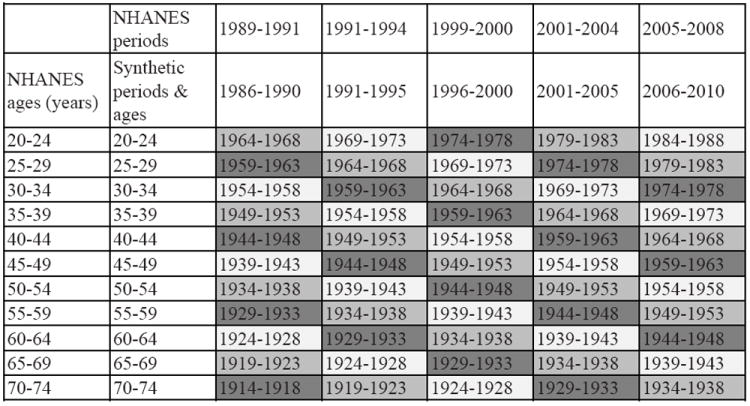
Graphical representation of the construction of 15 synthetic birth cohorts using data from the National Health and Nutrition Examination Survey (NHANES), 1988-2008
Once each contingency table was complete (Table 1), the median polish method was performed by iteratively subtracting the median prevalence value of each row or column from all cells in its respective row or column. This process was repeated until the median values of all rows and columns equaled 0. This process removes the additive period and age effects. The values that remain in the table are non-additive residuals of the period and age effects. The median polish technique interprets these residuals as the sum of cohort effects and random error. Further statistical and conceptual details of the median polish method are given elsewhere.18, 20, 24, 25
Table 1.
Contingency table of prevalence of abdominal obesity arrayed by age and period, U.S.-born respondents to the National Health and Nutrition Examination Survey (NHANES), 1988-20081
| NHANES periods | 1989-1991 | 1991-1994 | 1999-2000 | 2001-2004 | 2005-2008 | |
|---|---|---|---|---|---|---|
|
| ||||||
| NHANES ages (years) | Synthetic ages and periods | 1986-1990 | 1991-1995 | 1996-2000 | 2001-2005 | 2006-2010 |
| 20-24 | 20-24 | 16.75 | 15.66 | 25.53 | 32.53 | 28.25 |
| 25-29 | 25-29 | 19.38 | 21.8 | 39.93 | 34.91 | 36.1 |
| 30-34 | 30-34 | 28.04 | 20.86 | 41.64 | 39.23 | 47.39 |
| 35-39 | 35-39 | 28.61 | 31.59 | 39.1 | 48.05 | 46.61 |
| 40-44 | 40-44 | 38.06 | 39.14 | 50.14 | 48.67 | 56.44 |
| 45-49 | 45-49 | 34.38 | 42.89 | 46.31 | 57.2 | 55.23 |
| 50-54 | 50-54 | 49.25 | 56.62 | 60.17 | 58.89 | 58.55 |
| 55-59 | 55-59 | 55.72 | 56.36 | 62.52 | 62.56 | 64.25 |
| 60-64 | 60-64 | 59.15 | 61.99 | 66.17 | 71 | 68.43 |
| 65-69 | 65-69 | 58.03 | 59.62 | 66.67 | 69.34 | 70.92 |
| 70-74 | 70-74 | 52.52 | 57.12 | 59.61 | 68.51 | 72.11 |
Addominal obesity was calculated using measured waist circumference. Respondents were classified as obese if they (1) were women with waist circumference ≥ 88.0 cm or (2) men with waist circumference ≥ 102.0 cm.
The residuals from the contingency table were used as data in a generalized linear regression model to be regressed on birth cohort. To define mutually exclusive birth cohort categories, each cell in the contingency table was assigned to a synthetic five-year birth cohort category. However, birth year could vary by as much as 9 years for each intersection of a 5-year age and 5-year period category. Therefore, we assigned synthetic five-year cohort categories centered on the median year of the possible 9-year birth range (see Figure 1). The residuals from the contingency table were regressed on these nominal categories of 5-year birth cohort, using 1959-1963 as the reference category. We chose the 1959-1963 birth cohort as the reference in order to maximize statistical robustness; this cohort has relatively many observations across age and time. Additionally, the 1959-1963 birth cohort had uniquely low cohort risk in a previous analyses of overall obesity.26 We also performed sensitivity analyses using the preceding birth cohort (1954-1958).
RESULTS
Descriptive data
The final survey-weighted sample was composed of 51.0% women (n=13 482) and 49.0% men (n=12 721). The racial/ethnic composition of the analytic sample was 79.6% non-Hispanic Whites (n=13 539), 11.9% non-Hispanic Black (n=7,687), 5.8% Hispanic (n=4 507), and 2.7% other (n=470). The sample used for supplemental analyses of overall obesity was similar (n=26 203).
In the earliest synthetic period, 1986-1990, abdominal obesity prevalence was 36.0% (27.5% in men and 44.3% in women). By the latest period, 2006-2010, abdominal obesity prevalence was 52.5% (43.1% in men and 61.5% in women). The respective values for BMI-assessed obesity were 21.1% (18.5% men, 23.6% in women) for 1986-1990 and 34.4% (32.6% men, 36.0% in women) for 2006-2010.
Age and period effects on abdominal obesity
Based on visual inspection of Figure 2, age has a strong influence on abdominal obesity. Abdominal obesity increases with age, even more so than BMI-assessed obesity does. Further, Figure 2 shows that period effects, or secular trends, between the late 1980s and late 2000s contributed to steady increases in abdominal obesity across all age groups.
Figure 2.
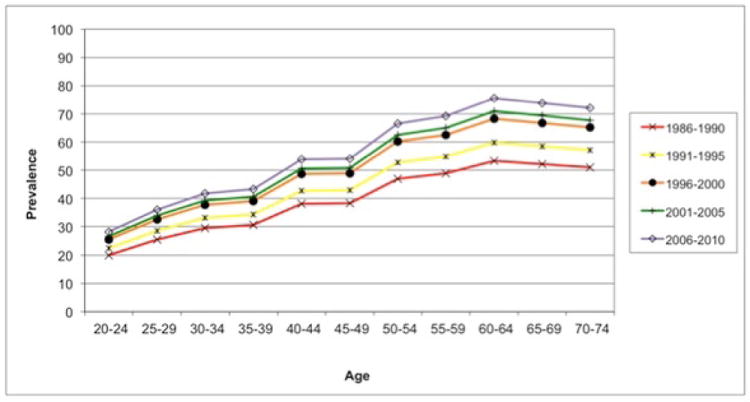
Period effects on abdominal obesity prevalence in overall sample by age group, U.S.-born NHANES respondents, 1988-2008
Cohort effects on abdominal obesity
This analysis found evidence of cohort effects for abdominal obesity among the synthetic birth cohorts corresponding to the Silent Generation (1924-1943), the Baby Boomers (1944-1963), and Generation X (1964-1978). Point estimates for more distantly born (before 1924) and recently born cohorts (after 1978) were estimated but de-emphasized because these estimates are less statistically precise due to relatively few years of observation. The Silent Generation and Generation X show positive cohort effects for abdominal obesity (see Table 2) compared to the 1959-1963 referent birth cohort. For instance, the estimated prevalence ratio (PR) for the 1924-1928 cohort was 1.18 (95% CI: 1.01, 1.37). Similarly, members of the 1974-1978 cohort were 1.22 (1.05, 1.43) times as likely as the referent cohort to have abdominal obesity controlling for age and secular influences.
Table 2.
Cohort effects for prevalence of abdominal obesity, U.S.-born respondents to the National Health and Nutrition Examination Survey (NHANES), 1988-20081
| Synthetic birth cohort | Prevalence ratio | 95% CI | |
|---|---|---|---|
| 1914-1918 | 1.2 | (0.95, 1.50)2 | |
| 1919-1923 | 1.23 | (1.03, 1.46)2 | |
| Silent Generation | 1924-1928 | 1.18 | (1.01, 1.37) |
| 1929-1933 | 1.22 | (1.06, 1.40) | |
| 1934-1938 | 1.17 | (1.03, 1.34) | |
| 1939-1943 | 1.15 | (1.00, 1.31) | |
| Baby Boomers | 1944-1948 | 1.13 | (0.99, 1.29) |
| 1949-1953 | 1.09 | (0.95, 1.24) | |
| 1954-1958 | 1.14 | (1.00, 1.30) | |
| 1959-1963 | 1 | ||
| Generation X | 1964-1968 | 1.13 | (0.99, 1.29) |
| 1969-1973 | 1.14 | (0.99, 1.31) | |
| 1974-1978 | 1.22 | (1.05, 1.43) | |
| 1979-1983 | 1.29 | (1.08, 1.53)2 | |
| 1984-1988 | 1.16 | (0.93, 1.46)2 |
Abdominal obesity was calculated using measured waist circumference. Respondents were classified as obese if they (1) were women with waist circumference ≥ 88.0 cm or (2) men with waist circumference ≥ 102.0 cm.
Inference limited due to small number of data points upon which estimates based.
Within the Baby Boom generation, there was evidence of variation in cohort-specific risk. The latest born members of the Baby Boom generation may have uniquely low cohort risk of abdominal obesity (see Table 2). In fact, when a cohort of earlier-born Boomers (1954-1958) was selected as the referent group, cohort differences showed the same trend but were no longer statistically significant.
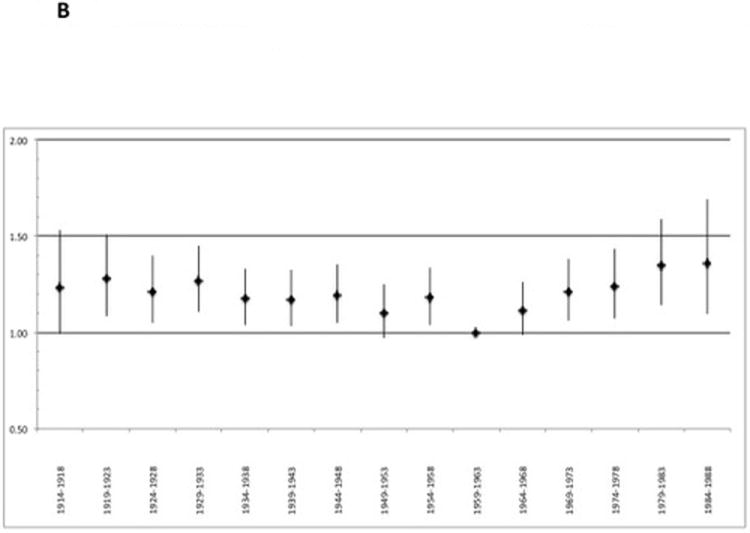
Cohort effects differed by sex. In men, there were no statistically significant cohort differences in abdominal obesity (see Figure 3A). In contrast, cohort effects were pronounced in women (see Figure 3B): Most synthetic 5-year cohorts of the Silent Generation and Generation X were statistically more likely than the referent cohort to experience abdominal obesity, given the same age and secular influences. Analyses stratified by both sex and race/ethnicity were not statistically stable enough to draw strong inferences.
Figure 3.
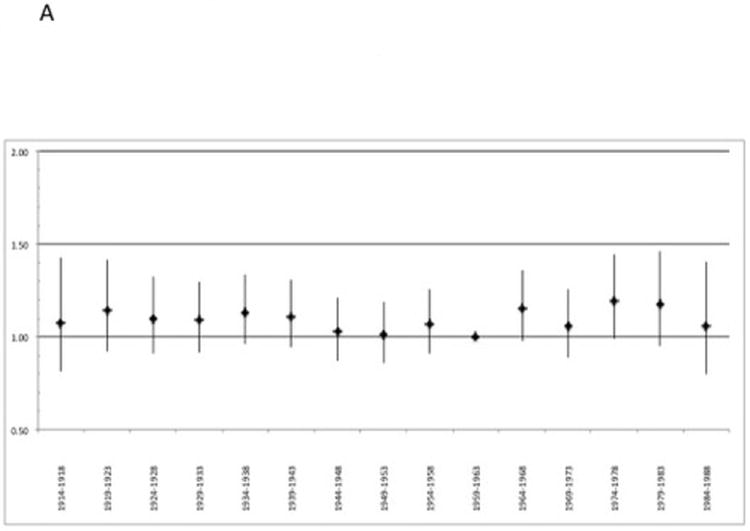
A. Birth cohort effects on obesity prevalence in males, U.S.-born NHANES respondents, 1988-2008
B. Birth cohort effects on obesity prevalence in females, U.S. born NHANES respondents, 1988-2008
Supplemental analyses of overall BMI-assessed obesity
Cohort effects on overall obesity assessed by BMI were similar to the effects on abdominal obesity. The only notable difference was for the cohort born during the first years of the Great Depression (1929-1933). In analysis of BMI-assessed obesity, this cohort showed greater cohort-specific risk than the cohorts preceding and following it.
Examining cohort effects for obesity assessed by BMI allowed us to address one limitation of the analysis of abdominal obesity: the limited range of years under study. Waist circumference data were not available in NHANES I (1971-1975) nor NHANES II (1976-1980), while BMI data were available earlier. To investigate how the range of survey years may have affected our results on abdominal obesity, we examined how results on overall obesity were affected by incorporating pre-1988 data from NHANES. Using data collected between 1971 and 2008, eight synthetic 5-year period categories were approximated. Because no NHANES data were available between 1981 and 1988, age-specific obesity prevalences for the synthetic period 1981-1985 were interpolated by averaging age-specific prevalence for the previous (1976-1980) and subsequent (1986-1990) periods.
In women, incorporating the additional years of data did not dramatically affect trends, except that the increased cohort effects for the Silent Generation were no longer statistically significant. Incorporating additional years had more dramatic effects in men than women. With the additional data, Silent Generation men born during the Great Depression had significantly higher cohort effects for overall obesity than the 1959-1963 cohort. The additional data appeared to reveal a generational divergence in obesity prevalence for male children of the Great Depression, especially those born in 1929-1933, versus male Baby Boomers.
CONCLUSIONS
This work presents a novel finding: evidence of birth cohort effects in prevalence of abdominal obesity in the U.S. The birth cohorts of the post-World War II Baby Boom appeared to have uniquely low cohort-specific risk for abdominal obesity. The birth cohorts preceding the Baby Boom, especially the cohort born in the first years of the Great Depression, appeared to show cohort-specific risks of increased prevalence of abdominal obesity. The birth cohorts immediately succeeding the Baby Boom also showed evidence of birth cohort effects that increased prevalence of abdominal obesity. These generational differences were more pronounced in women than in men.
There are several different ways of conceptualizing the underlying meaning of a cohort effect.25 This paper’s conceptualization is rooted in the potential outcomes counterfactual framework. 27-29 To understand this conceptualization heuristically, imagine a scenario in which a 16-year-old Baby Boom adolescent (born in 1962) travels in time from 1978 to 1993.29 If the adolescent stayed in her 1993 “future,” then over time, as she aged into her 20s, 30s, 40s, etc., she would be less likely to become obese than other people her age who were born in 1977.29 Thus, this hypothetical counterfactual intervention can be interpreted to mean that the Baby Boomer who traveled in time from 1978 was less sensitive to the obesogenic environment of the 1990s, 2000s, etc., than the same-age Generation X counterparts she was living with in the “future.” The negative cohort effect that we estimated for the Baby Boom, suggests that, in alternative environments, Baby Boomers might be less susceptible to the obesogenic environment due to factors intrinsic to being a member of the Baby Boom cohort that are independent of age and widespread environmental exposures that act the same on all age groups.
No previous studies have examined cohort effects on abdominal obesity. Examining cohort effects for abdominal obesity is important because large waist circumference is a better predictor of obesity-related diseases such as diabetes, metabolic syndrome, and cardiovascular disease than high BMI.1, 4, 30 Understanding cohort effects on abdominal obesity serves three important purposes. First, cohort effects help predict trends in metabolic health.12, 26, 31 These results indicate that, holding the secular environment constant, as members of Generation X age, they will be more sensitive to abdominal obesity, and therefore, metabolic diseases, than the Baby Boomers.
Second, estimating cohort effects on abdominal obesity aids evaluating hypotheses about the causes of population-level obesity trends.6 Komlos et al. have argued that monotonically increasing cohort effects would provide evidence that a root cause of the U.S. obesity epidemic is ever-expanding access to labor-saving technology, including radios and home refrigeration.6 In contrast, we find that the cohorts born during the economic and consumerist expansion of the post-World-War II era may have been uniquely protected from abdominal obesity, especially among women. This finding indicates that the generational increases in abdominal obesity could be caused by factors beyond technological innovation, expansion of access to technology, and economic growth.
Third, estimating cohort effects can illuminate the causes of individual-level susceptibility to abdominal obesity. In our analysis, period effects were consistently positive and strong. These period effects could be caused by many dynamic environmental features, including increases in use of some antibiotics, growing use of plastic bottles and ingestion of the chemical contained in them, and even secular trends in sleep deprivation. 32 However, environmental factors can also cause cohort effects through distinct mechanisms. In particular, characteristics of the early-life environment that affect obesity in an age-specific manner may have protected the Baby Boomers against obesogenic influences that they encountered later in life. For instance, hypotheses about the developmental origins of adult obesity posit that in utero and early-childhood exposures to obesogenic environments have latent biological or behavioral consequences that increase susceptibility to excess weight gain throughout adulthood.8, 33-35
While no previous analyses have examined cohort effects on abdominal obesity, three analyses of overall obesity in population-based datasets have also found lower cohort effects for Baby Boomers than the preceding or subsequent generations.26, 36, 37 In studies of French and Australian populations, cohort risk was lowest for those born between the mid-1940s and mid-1960s.36, 38 In the U.S., analysis of the National Health Interview Survey estimated that cohort effects were lowest for cohorts of the mid-1950s before rising sharply in the cohorts of the 1960s and early 1970s.37
One possible mechanism for cohort differences is early-life psychosocial and socioeconomic stress mechanisms, which may promote abdominal obesity.39, 40 The growing prosperity of the post-World-War II may have exposed the Baby Boom generation to lower levels of psychosocial and socioeconomic stress than previous or subsequent generations.41 Diouf et al. hypothesized that the cohort trends in the French post-World War II generation may be related to “the 30 glorious” years, a period from 1945 to 1973, in which there was a “marked improvement of living conditions that accompanied the economic boom in France.”36 They hypothesized that the improvement in living conditions caused the increase in obesity for cohorts born after 1965. An alternative interpretation is that the specific living conditions associated with a trajectory of increasing prosperity from 1945 to 1965 protected cohorts born after the war. In contrast, the nutritional deprivation and stress experienced by those born during the Great Depression may have predisposed these cohorts to obesity risk, while obesogenic social and economic trends in the mid-1960s and 1970s increased cohort risk.
There are other possible explanations for the observed cohort effects, especially the greater cohort-specific obesity prevalence in Generation X versus the Baby Boomers.32 For instance, cohort differences in sleep patterns could explain greater obesity in Generation X. Another possible mechanism for increased cohort effects for Generation X is endocrine disrupters, which may exert long-standing effects in infancy and childhood. Also, demographic changes could be associated with cohort trends in obesity. In our 2001-2004 sample of U.S.-born non-immigrants, the percentage of the population who were non-Hispanic Black or non-Hispanic White, groups that tend to have higher obesity prevalence than non-Hispanic Whites, increased across the birth cohorts. For instance, the weighted proportion of the sample who were non-Hispanic Black ranged from 7.0% for the 1929-1933 cohort to 16.1% for the 1979-1983 cohort. The share of the population who were non-Hispanic White population decreased from 85.7% for the 1929-1933 cohort to 70.4% for the 1979-1983 cohort.
Stratified analyses indicated more pronounced cohort differences among women than men. This sex difference was also seen in the age-period-cohort analyses of overall obesity described above.26, 36, 37 In Europe and the U.S., social conditions for women have changed dramatically throughout the 20th century. Patterns of fertility, work outside the home, physical activity, and economic autonomy have varied more dramatically for women than men in the cohorts examined.42 For instance, the U.S. Title IX law increased girls’ sports participation by 600% between 1972 and 1978, years when Baby Boomers were entering secondary school and college.43 Therefore, cohort effects that are caused or mediated by behavioral or social exposures would be expected to vary more in women than men.
Physiologically, stress mechanisms may also act in a sex-specific manner to influence abdominal obesity.39, 44 Previous studies have found evidence linking in utero maternal stress and malnutrition to sex-specific obesity risk, such as interference with sex hormone signaling; alteration of methylation patterns of genes, including insulin-like growth factor-2; and sex-specific effects on appetite and weight regulation.45-47 Maternal nutritional and psychological stress may be an especially important mechanism for understanding the higher cohort effects for the children of the Great Depression.
Despite its strengths and novelty, this analysis has limitations. The unit of analysis was the prevalence estimate, which was estimated from survey data with error that was not incorporated into our final confidence intervals. Therefore, the confidence intervals may overestimate the precision of the effect estimates. Additionally, these results only apply to non-institutionalized, U.S.-born Americans and not to immigrants, the imprisoned, or those in long-term care facilities.48, 49 Finally, the analyses did not assess data collected before the late 1980s. Additional analyses of obesity assessed by BMI indicated that extending the time period would not dramatically affect findings in women but might reveal more evidence of cohort effects in men. Perhaps results in men differed after including earlier data because obesity-related selective mortality obscured cohort effects in men in the more limited dataset. If obese men have higher rates of mortality or old-age institutionalization, then obese men from early birth cohorts would be underrepresented in our dataset. Further, excluding incarcerated men from the data may have caused overestimation of obesity prevalence for men of Generation X.49
In conclusion, controlling for age and secular influences on obesity prevalence, Baby Boomers appeared to experience lower cohort-specific risk of abdominal obesity than other birth cohorts. While secular forces in the 20th century may have introduced technological and cultural changes that increased obesity in the population, cohort-specific influences somewhat protected the Baby Boomers from these secular influences. Broad economic expansion does not necessarily lead to increased cohort-specific risk of abdominal obesity for those born during periods of economic growth. We hope that this work will spur further research into differences between the cohorts of the late 1950s and early 1960s versus other birth cohorts. By identifying factors associated with the Baby Boomers’ low cohort-specific sensitivity to the obesogenic environment, the obesity prevention community can identify early-life factors that can protect future generations from excess weight gain.
Acknowledgments
Dr. Yang is supported by NIA grant no. 1K01AG036745-01 and University Cancer Research Funds (UCRF) at the Lineberger Cancer Center at UNC-Chapel Hill.
Footnotes
CONFLICT OF INTEREST
Dr. Robinson would like to thank the National Cancer Institute (1K01CA172717-01) and University Cancer Research Funds at the Lineberger Cancer Center at UNC-Chapel Hill for their financial support. Dr. Keyes has no conflict of interest, and would like to thank Columbia University Department of Epidemiology and New York State Psychiatric Institute for its financial support. Dr. Utz has no conflict of interest, and would like to thank the University of Utah Department of Sociology and NCI P01-CA13837 for current financial support. Ms. Martin does not have any conflict of interest and would like to thank the University of North Carolina at Chapel Hill and grant no. 5-T32-HD052468-04 for current financial support.
References
- 1.Janssen I, Katzmarzyk PT, Ross R. Waist circumference and not body mass index explains obesity-related health risk. Am J Clin Nutr. 2004;79(3):379–84. doi: 10.1093/ajcn/79.3.379. [DOI] [PubMed] [Google Scholar]
- 2.Li C, Ford ES, McGuire LC, Mokdad AH. Increasing trends in waist circumference and abdominal obesity among US adults. Obesity (Silver Spring) 2007;15(1):216–24. doi: 10.1038/oby.2007.505. [DOI] [PubMed] [Google Scholar]
- 3.Bouchard C. BMI, fat mass, abdominal adiposity and visceral fat: where is the ‘beef’? International journal of obesity. 2007;31(10):1552–3. doi: 10.1038/sj.ijo.0803653. [DOI] [PubMed] [Google Scholar]
- 4.Relationship of body size and shape to the development of diabetes in the diabetes prevention program. Obesity (Silver Spring) 2006;14(11):2107–17. doi: 10.1038/oby.2006.246. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 5.Frey WH, Abresch B, Yeasting J. America by the Numbers: A Field Guide to the US Population. First edn. New Press; 2001. [Google Scholar]
- 6.Komlos J, Brabec M. The trend of mean BMI values of US adults, birth cohorts 1882-1986 indicates that the obesity epidemic began earlier than hitherto thought. Am J Hum Biol. 2010;22(5):631–8. doi: 10.1002/ajhb.21055. [DOI] [PubMed] [Google Scholar]
- 7.Komlos J, Brabec M. The trend of BMI values of US adults by deciles, birth cohorts 1882-1986 stratified by gender and ethnicity. Economics and human biology. 2011 doi: 10.1016/j.ehb.2011.03.005. [DOI] [PubMed] [Google Scholar]
- 8.Gluckman P, Hanson M. Developmental and epigenetic pathways to obesity: an evolutionary-developmental perspective. International Journal of Obesity. 2008;32:S62–S71. doi: 10.1038/ijo.2008.240. [DOI] [PubMed] [Google Scholar]
- 9.National Center for Health Statistics. Plan and operation of the health and nutrition examination survey. United states--1971-1973. Vital and Health Statistics. 1978:1–407. [PubMed] [Google Scholar]
- 10.National Center for Health Statistics. Plan and operation of the Third National Health and Nutrition Examination Survey, 1988-94. Series 1: programs and collection procedures. Vital and Health Statistics. 1994:1–46. [PubMed] [Google Scholar]
- 11.National Center for Health Statistics. Analytic and reporting guidelines: the national health and nutrition examination survey (NHANES) 2005 [Google Scholar]
- 12.Flegal KM, Carroll MD, Ogden CL, Curtin LR. Prevalence and Trends in Obesity Among US Adults, 1999-2008. JAMA. 2010 doi: 10.1001/jama.2009.2014. 2009.2014. [DOI] [PubMed] [Google Scholar]
- 13.National Institutes of Health NH, Lung, and Blood Institute. Clinical Guidelines on the Identification, Evaluation, and Treatment of Overweight and Obesity in Adults--The Evidence Report. Obes Res. 1998;6(Suppl 2):S51–209. [PubMed] [Google Scholar]
- 14.Yang Y, Land KC. A Mixed Models Approach to Age-Period-Cohort Analysis of Repeated Cross-Section Surveys: Trends in Verbal Test Scores. Sociological Methodology. 2006;36:75–97. [Google Scholar]
- 15.Eggebeen DJ, Lichter DT. Race, Family Structure, and Changing Poverty Among American Children. American Sociological Review. 1991;56(6):801–817. [Google Scholar]
- 16.Physical status: the use and interpretation of anthropometry. Report of a WHO Expert Committee. World Health Organization technical report series. 1995;854:1–452. [PubMed] [Google Scholar]
- 17.Ryder NB. The cohort as a concept in the study of social change. American Sociological Review. 1965;30(6):843–861. [PubMed] [Google Scholar]
- 18.Keyes KM, Li G. Age-period-cohort analysis in injury epidemiology. In: Li G, Baker SP, editors. Injury Research: Theories, Methods, Approaches. Springer; New York: 2011. [Google Scholar]
- 19.Keyes KM, Schulenberg JE, O’Malley PM, Johnston LD, Bachman JG, Li G, et al. The social norms of birth cohorts and adolescent marijuana use in the United States, 1976-2007. Addiction. 2011;106(10):1790–800. doi: 10.1111/j.1360-0443.2011.03485.x. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 20.Keyes KM, Li G. A multiphase method for estimating cohort effects in age-period contingency table data. Annals of epidemiology. 2010;20(10):779–85. doi: 10.1016/j.annepidem.2010.03.006. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 21.Yang Y. The Handbook of Aging and the Social Sciences. 7. Academic Press; London; Burlington, MA; San Diego, CA: 2010. Aging, Cohorts, and Methods; pp. 17–30. [Google Scholar]
- 22.Tu YK, Kramer N, Lee WC. Addressing the Identification Problem in Age-period-cohort Analysis: A Tutorial on the Use of Partial Least Squares and Principal Components Analysis. Epidemiology. 2012;23(4):583–93. doi: 10.1097/EDE.0b013e31824d57a9. [DOI] [PubMed] [Google Scholar]
- 23.Reither EN, Olshansky SJ, Yang Y. New Forecasting Methodology Indicates More Disease And Earlier Mortality Ahead For Today’s Younger Americans. Health Aff (Millwood) 2011 doi: 10.1377/hlthaff.2011.0092. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 24.Selvin S. Statistical analysis of epidemiologic data. 2. Oxford University Press; New York: 1996. [Google Scholar]
- 25.Keyes KM, Utz RL, Robinson W, Li G. What is a cohort effect? Comparison of three statistical methods for modeling cohort effects in obesity prevalence in the United States, 1971-2006. Soc Sci Med. 2010;70(7):1100–8. doi: 10.1016/j.socscimed.2009.12.018. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 26.Robinson WR, Keyes KM, Utz RL, Martin CL, Yang Y. Birth cohort effects among US-born adults born in the 1980s: foreshadowing future trends in US obesity prevalence. International journal of obesity. 2012 doi: 10.1038/ijo.2012.66. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 27.Hernan MA, Hernandez-Diaz S, Robins JM. A structural approach to selection bias. Epidemiology. 2004;15(5):615–25. doi: 10.1097/01.ede.0000135174.63482.43. [DOI] [PubMed] [Google Scholar]
- 28.Rubin DB. For Objective Causal Inference, Design Trumps Analysis. Annals of Applied Statistics. 2008;2(3):808–840. [Google Scholar]
- 29.Suzuki E. Time changes, so do people. Social Science & Medicine. 2012 doi: 10.1016/j.socscimed.2012.03.036. [DOI] [PubMed] [Google Scholar]
- 30.Brenner DR, Tepylo K, Eny KM, Cahill LE, El-Sohemy A. Comparison of body mass index and waist circumference as predictors of cardiometabolic health in a population of young Canadian adults. Diabetol Metab Syndr. 2010;2(1):28. doi: 10.1186/1758-5996-2-28. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 31.Faeh D, Bopp M. Increase in the prevalence of obesity in Switzerland 1982-2007: birth cohort analysis puts recent slowdown into perspective. Obesity (Silver Spring) 2010;18(3):644–6. doi: 10.1038/oby.2009.310. [DOI] [PubMed] [Google Scholar]
- 32.Keith SW, Redden DT, Katzmarzyk PT, Boggiano MM, Hanlon EC, Benca RM, et al. Putative contributors to the secular increase in obesity: exploring the roads less traveled. International journal of obesity. 2006;30(11):1585–94. doi: 10.1038/sj.ijo.0803326. [DOI] [PubMed] [Google Scholar]
- 33.Lawlor DA, Timpson NJ, Harbord RM, Leary S, Ness A, McCarthy MI, et al. Exploring the developmental overnutrition hypothesis using parental-offspring associations and FTO as an instrumental variable. PLoS Med. 2008;5(3):e33. doi: 10.1371/journal.pmed.0050033. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 34.Gluckman PD, Hanson MA. The developmental origins of the metabolic syndrome. Trends Endocrinol Metab. 2004;15(4):183–7. doi: 10.1016/j.tem.2004.03.002. [DOI] [PubMed] [Google Scholar]
- 35.Ravelli AC, van Der Meulen JH, Osmond C, Barker DJ, Bleker OP. Obesity at the age of 50 y in men and women exposed to famine prenatally. Am J Clin Nutr. 1999;70(5):811–6. doi: 10.1093/ajcn/70.5.811. [DOI] [PubMed] [Google Scholar]
- 36.Diouf I, Charles M, Ducimetière P, Basdevant A, Eschwege E, Heude B. Evolution of Obesity Prevalence in France: An Age-Period-Cohort Analysis. Epidemiology. 2010;21(3):360. doi: 10.1097/EDE.0b013e3181d5bff5. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 37.Reither EN, Hauser RM, Yang Y. Do birth cohorts matter? Age-period-cohort analyses of the obesity epidemic in the United States. Soc Sci Med. 2009;69(10):1439–48. doi: 10.1016/j.socscimed.2009.08.040. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 38.Allman-Farinelli MA, Chey T, Bauman AE, Gill T, James WP. Age, period and birth cohort effects on prevalence of overweight and obesity in Australian adults from 1990 to 2000. European journal of clinical nutrition. 2008;62(7):898–907. doi: 10.1038/sj.ejcn.1602769. [DOI] [PubMed] [Google Scholar]
- 39.Bjorntorp P. Do stress reactions cause abdominal obesity and comorbidities? Obesity reviews : an official journal of the International Association for the Study of Obesity. 2001;2(2):73–86. doi: 10.1046/j.1467-789x.2001.00027.x. [DOI] [PubMed] [Google Scholar]
- 40.Dallman MF, Pecoraro NC, la Fleur SE. Chronic stress and comfort foods: self-medication and abdominal obesity. Brain Behav Immun. 2005;19(4):275–80. doi: 10.1016/j.bbi.2004.11.004. [DOI] [PubMed] [Google Scholar]
- 41.Franzini L, Ribble JC, Keddie AM. Understanding the Hispanic paradox. Ethn Dis. 2001;11(3):496–518. [PubMed] [Google Scholar]
- 42.Federici N, Mason KO, Sogner S, editors. Women’s Position and Demographic Change. Clarendon Press; Oxford, UK: 1993. pp. 190–212. [Google Scholar]
- 43.Kaestner R, Xin X. Title IX, girls’ sports participation, and adult female physical activity and weight. Eval Rev. 2010;34(1):52–78. doi: 10.1177/0193841X09353539. [DOI] [PubMed] [Google Scholar]
- 44.Poore KR, Boullin JP, Cleal JK, Newman JP, Noakes DE, Hanson MA et al. Sex- and age-specific effects of nutrition in early gestation and early postnatal life on hypothalamo-pituitary-adrenal axis and sympathoadrenal function in adult sheep. J Physiol. 2010;588(Pt 12):2219–37. doi: 10.1113/jphysiol.2010.187682. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 45.Dunn GA, Morgan CP, Bale TL. Sex-specificity in transgenerational epigenetic programming. Hormones and behavior. 2011;59(3):290–5. doi: 10.1016/j.yhbeh.2010.05.004. [DOI] [PubMed] [Google Scholar]
- 46.Case A, Menendez A. Sex differences in obesity rates in poor countries: evidence from South Africa. Econ Hum Biol. 2009;7(3):271–82. doi: 10.1016/j.ehb.2009.07.002. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 47.Hult M, Tornhammar P, Ueda P, Chima C, Edstedt Bonamy AK, Ozumba B, et al. Hypertension, diabetes and overweight: looming legacies of the biafran famine. PLoS One. 5(10):e13582. doi: 10.1371/journal.pone.0013582. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 48.Park J, Myers D, Kao D, Min S. Immigrant obesity and unhealthy assimilation: alternative estimates of convergence or divergence, 1995-2005. Soc Sci Med. 2009;69(11):1625–33. doi: 10.1016/j.socscimed.2009.09.008. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 49.Houle B. Obesity disparities among disadvantaged men: national adult male inmate prevalence pooled with non-incarcerated estimates, United States, 2002-2004. Social science & medicine. 2011;72(10):1667–73. doi: 10.1016/j.socscimed.2011.03.039. [DOI] [PMC free article] [PubMed] [Google Scholar]