

In recent years, treatment of severe acute pancreatitis has shifted away from early surgical treatment to aggressive intensive care. While the treatment is conservative in the early phase, surgery might be considered in the later phase of the disease. Surgical debridement is still the “gold standard” for treatment of infected pancreatic and peripancreatic necrosis. Advances in radiological imaging, new developments in interventional radiology, and other minimal access interventions have revolutionised the management of many surgical conditions over the past decades. Several interventional therapy regimens, including endoscopic retrograde cholangiopancreatography (ERCP) and sphincterotomy, fine needle aspiration for bacteriology (FNAB), percutaneous or endoscopic drainage of peripancreatic fluid collections, pseudocysts, and late abscesses, as well as selective angiography and catheter directed embolisation of acute pancreatitis associated bleeding complications have been well established as diagnostic and therapeutic standards in the management of acute pancreatitis. Secondary to recent technical improvements in interventional therapy and minimally invasive surgery, even infected pancreatic necrosis has successfully been treated in selected patients. However, technical feasibility does not obviate sound clinical judgement. We must be cautious in the application of new technologies in the absence of well designed clinical trials. Thus minimally invasive surgery and interventional therapy for infected necrosis should be limited to clinical trials and specific indications in patients who are critically ill and otherwise unfit for conventional surgery.
INTRODUCTION
The management of acute pancreatitis has been controversial over the past decades, varying between a conservative medical approach on the one hand and an aggressive surgical approach on the other. There has been great improvement in knowledge of the natural course and pathophysiology of acute pancreatitis over the past decade.1–4 The clinical course of acute pancreatitis varies from a mild transitory form to a severe necrotising disease. Most episodes of acute pancreatitis (80%) are mild and self limiting, subsiding spontaneously within 3–5 days. Patients with mild pancreatitis respond well to medical treatment, requiring little more than intravenous fluid resuscitation and analgesia.5 In contrast, severe pancreatitis is defined as pancreatitis associated with organ failure and/or local complications such as necrosis, abscess formation, or pseudocysts. Severe pancreatitis can be observed in 15–20% of all cases.6,7
In general, severe pancreatitis develops in two phases. The first two weeks after onset of symptoms are characterised by the systemic inflammatory response syndrome (SIRS). Release of proinflammatory mediators is thought to contribute to the pathogenesis of SIRS associated pulmonary, cardiovascular, and renal insufficiency.8–10 In parallel, pancreatic necrosis develops within the first four days after the onset of symptoms to its full extent.11 Although SIRS in the early phase of severe pancreatitis may be found in the absence of significant pancreatic necrosis, the majority of patients with severe early organ dysfunction will have pancreatic necrosis on computed tomography (CT) scan.3,12 Late deterioration of organ dysfunction occurs most commonly in the second to third week after admission,11 and is usually the result of secondary infection of pancreatic or peripancreatic necrosis. Today, infection of pancreatic necrosis is still the major risk factor of sepsis related multiple organ failure and the main life threatening complication of severe acute pancreatitis.4,13,14 Infection of pancreatic necrosis can be observed in 40–70% of patients with necrotising disease.11 The risk of infection increases with the extent of intra- and extrapancreatic necrosis.14 Management of acute pancreatitis in the two phases of the disease is different. In recent years, treatment of severe acute pancreatitis has shifted away from early surgical debridement/necrosectomy to aggressive intensive medical care.6,15–17 While the treatment is conservative in the earlier phase of the disease, surgery must be considered in the second phase.
Advances in radiological imaging, new developments in interventional radiology, and other minimal access interventions have revolutionised the management of many surgical conditions over the past decades. Today, it is recommended that severe acute pancreatitis be treated in specialist units with multidisciplinary expertise available on site, including intensive care specialists, interventional endoscopists, diagnostic and interventional radiologists, and surgeons.5,6,15 Considering recent improvements in interventional therapy regimens, this article reviews the present role of surgery and interventional intensive care in the management of severe acute pancreatitis.
MANAGEMENT OF SEVERE PANCREATITIS
The most significant change in the clinical course of acute pancreatitis over the past decade has been the decrease in overall mortality to approximately 5% and for severe cases to 10–20%.13,17–20 Despite the reduction in overall mortality in severe pancreatitis, the percentage of early mortality from the disease differs from less than 10% to 85% between various centres and countries.3,8,12,13,21 This wide variation in early mortality may partially be explained by differences in health systems, socioeconomic issues, patient selection, or referral patterns to specialised units.
There are two primary objectives in the initial treatment of patients with acute pancreatitis. The first is to provide supportive therapy and to treat specific complications which may occur. The second is to limit both the severity of pancreatic inflammation and necrosis and the systemic inflammatory response by specifically interrupting their pathogenesis. Due to its high mortality, early surgical intervention has no role in these patients.22
It is generally accepted that all patients with signs of moderate to severe acute pancreatitis should be admitted to an intensive care unit and referred to specialised centres for maximum supportive care.5,6,15 As complications may develop at any time, frequent reassessment and continuous monitoring is necessary. The most important supportive therapy is adequate and prompt fluid resuscitation with intravenous fluids and supplemental oxygen, with a liberal indication for assisted or controlled ventilation to guarantee optimal oxygen transport.6,15,23,24
Infection in pancreatitis is a secondary event. Evidence indicates that bacteria from the gastrointestinal tract translocate into necrotic tissues. As the development of necrosis is currently not preventable, the rationale for the use of prophylactic antibiotics in severe pancreatitis is to prevent infection of pancreatic necrosis.6,15,25 Evidence for the effectiveness of prophylactic antibiotics in the reduction of septic complications and mortality of necrotising pancreatitis has been demonstrated in several randomised controlled trials.26,27 To date, inhibition of any known pathogenetic step (that is, octreotide, gabexate mesilate, lexipafant) has not effectively reduced mortality or increased long term survival in severe acute pancreatitis.8,28–30 Thus treatment of acute pancreatitis is still symptomatic, with no specific medication being currently available.
However, a causative therapy exists for severe gall stone pancreatitis with an impacted stone, biliary sepsis, or obstructive jaundice.6,15 Although there is no clear consensus on all indications for endoscopic retrograde cholangiopancreatography (ERCP) and endoscopic sphincterotomy (ES),31–33 it is generally accepted and well established that they are indicated for acute cholangitis and/or obstructive jaundice. Under these conditions ERCP and ES ameliorate symptoms and progression of the disease when applied early.6,15 In contrast, open cholecystectomy with supraduodenal bile duct exploration and insertion of a T tube is an unacceptable emergency procedure in patients with severe gall stone associated pancreatitis.34 While comorbidity is a major predeterminant of outcome from cholecystectomy, this factor does not apply to the use of ERCP and ES.35
“Surgery has little use in the early management of acute pancreatitis. Interventional endoscopy with sphincterotomy is indicated for acute cholangitis and/or obstructive jaundice in gall stone associated acute pancreatitis”
PANCREATIC INFECTION
Today, more patients survive the first phase of severe acute pancreatitis due to improvements in intensive care medicine, thus increasing the risk of later sepsis.13,36,37 There is no doubt that pancreatic infection is the major risk factor in necrotising pancreatitis with regard to morbidity and mortality in the second phase of the disease. The mortality rate for patients with infected pancreatic necrosis is higher than 20%, and up to 80% of fatal outcomes in acute pancreatitis are due to septic complications.6,11,38 In contrast, mortality for sterile necrosis is low and can usually be successfully treated by a conservative approach, although surgery might be required for late complications or persistent severe pancreatitis (table 1 ▶).6,13,19,39 Although reports have shown that some selected cases of acute pancreatitis with positive fine needle aspirates can be treated without surgery, conservative management of patients with infected necrosis and multiple organ failure is associated with mortality rates of up to 100%.40 There is general consensus that infected necrosis is an indication for surgical treatment or interventional drainage (table 1 ▶).6,15
Table 1.
Indications for surgical treatment of acute necrotising pancreatitis
| (1) Infected pancreatic necrosis |
| (2) Sterile pancreatic necrosis: |
| (a) persistent necrotising pancreatitis |
| (b) “fulminant acute pancreatitis” |
| (3) Complications of acute pancreatitis: |
| For example, bowel perforation, bleeding |
“Infected pancreatic necrosis is an indication for surgery or interventional drainage”
DIAGNOSIS OF INFECTED NECROSIS
Differentiation between sterile and infected necrosis is essential for the management of acute pancreatitis. It requires direct CT evidence of retroperitoneal gas or a positive fine needle aspiration for bacteriology (FNAB) of pancreatic or peripancreatic necrosis.6,15,41,42 The latter has been established as an accurate, safe, and reliable technique for the identification of infected necrosis.41–44 It can be guided by either CT or ultrasonography and is indicated in patients with CT proven necrosis and clinical signs of sepsis.6,15
“Fine needle aspiration for bacteriology (FNAB) is indicated in patients with necrotising pancreatitis and sepsis syndrome to differentiate between sterile and infected necrosis”
MANAGEMENT OF INFECTED NECROSIS
With surgical treatment, the mortality rate for patients with infected pancreatic necrosis could be decreased to approximately 20% in various specialised centres.13,18–20 Thus once infection develops, the therapeutic approach must be directed towards mechanical removal of infected necrotic tissue. In recent years, several alternatives to the traditional open surgical approaches have been investigated and the absolute requirement for surgical intervention in infected necrosis has been challenged.
TIMING OF NECROSECTOMY
Patients with severe necrotising pancreatitis can progress to a critical condition within a few hours or days after the onset of symptoms. Years ago, early surgical intervention was favoured when systemic organ complications were present. Mortality rates of up to 65% have been described with early surgery in severe pancreatitis, questioning the benefit of surgical intervention within the first days after onset of symptoms.17,22,45 In the only prospective randomised trial comparing early (within 72 hours of symptoms) with late (at least 12 days after onset) pancreatic resection/debridement in patients with severe pancreatitis, mortality rates were 56% and 27%, respectively.22 The trial was terminated because of concern about the very high mortality of early surgery. Today, there is general agreement that surgery in severe pancreatitis should be performed as late as possible.6,15 The third to fourth week after the onset of disease is agreed as providing optimal operative conditions with well demarcated necrotic tissue present, thus limiting the extent of surgery to pure debridement and to only one single intervention. This approach decreases the risk of bleeding, minimises the surgery related loss of vital tissue, and thus reduces endocrine and exocrine pancreatic insufficiency. Only in the case of proven infected necrosis or in the presence of rare complications, such as massive bleeding or bowel perforation, must early surgery be performed.6
“Surgical necrosectomy should be postponed to the third or fourth week after the onset of acute pancreatitis”
TECHNIQUES OF NECROSECTOMY
Standard surgical treatment
The aim is to control the focus so that further complications are avoided by stopping the progress of infection and the release of proinflammatory mediators. A generally agreed principle of surgical management includes the organ preserving approach which involves debridement and maximisation of postoperative removal of retroperitoneal debris and exudate. Four principal methods have been advocated: (1) necrosectomy combined with open packing46; (2) planned staged re-laparotomies with repeated lavage47; (3) closed continuous lavage of the lesser sac and retroperitoneum48,49; and (4) closed packing.19
Necrosectomy has traditionally been undertaken by an open route. Technical details are described elsewhere.16 Adequate debridement can usually be achieved with a single visit to the operating theatre. While necrosectomy is performed in a more or less identical fashion, the four techniques differ in the way they provide exit channels for further slough and infected debris. In the hands of experienced surgeons, mortality rates below 15% have been described for all four techniques: (1) open packing18,46,50,51; (2) repeated laparotomies20,47; (3) closed packing19; (4) closed continuous lavage13,48,49,51,52 (table 2 ▶).
Table 2.
Outcome of different techniques for open necrosectomy
| Technique | Patients &;(n) | Patients with &;infected necrosis | Mortality | Re-laparotomy &;(n) |
| “Open packing” | ||||
| Bradley 19937 | 71 | 71 (100%) | 15% | 1–5/pt |
| Branum 199818 | 50 | 42 (84%) | 6 (12%) | 2–13/pt |
| Bosscha 199850 | 28 | 28 (100%) | 11 (39%) | 17 (mean)/pt |
| Nieuwenhuijs 200351 | 38 | – | 18 (47%) | |
| “Planned re-laparotomies” | ||||
| Sarr 199147 | 23 | 18 (75%) | 4 (17%) | 2–>5/pt |
| Tsiotos 199820 | 72 | 57 (79%) | 18 (25%) | 1–7/pt |
| “Closed packing” | ||||
| Fernandez-del C 199819 | 64 | 36 (56%) | 4 (6%) | 11 (17%) |
| “Closed continuous lavage” | ||||
| Beger 198848 | 95 | 37 (39%) | 8 (8%) | 26 (27%) |
| Farkas 199652 | 123 | 123 (100%) | 9 (7%) | |
| Büchler 200013 | 29 | 27 (93%) | 7 (24%) | 6 (22%) |
| Büchler 2001 | 42 | 39 (93%) | 9 (21%) | 7 (17%) |
| Nieuwenhuijs 200351 | 21 | – | 7 (33%) |
The first two methods, the “open packing”18,46,50 and “planned staged re-laparotomies”20,47 have in common that they mandate several re-laparotomies before final closure of the abdomen. Although the incidence of recurrent intra-abdominal sepsis decreased significantly compared with single necrosectomy, postoperative morbidity remained high. There is a positive correlation between repeated surgical interventions and morbidity, including gastrointestinal fistula, stomach outlet stenosis, incisional hernia, and local bleeding. Thus these two procedures should only be considered in the rare case when early debridement is indicated. The other two techniques, necrosectomy and subsequent closed continuous lavage of the lesser sac13,52 and “closed packing”,19 have implicit a postoperative method to continuously remove residual pancreatic necrosis. Consequently, re-laparotomies are frequently not necessary. Thus postoperative morbidity, especially the percentage of gastrointestinal fistula and incisional hernias, is reduced (table 3 ▶). The results of the latter two surgical strategies with regard to morbidity, re-laparotomies, and mortality are comparable and thus dependent on the preference of the surgeon. The most commonly adopted approach is that of closed lavage of the debrided cavity, first described by Beger et al in 1982 (figs 1 ▶, 2 ▶).49
Table 3.
Complications of different techniques for open necrosectomy
| Technique | Patients &;(n) | Fistulas &;(pancreatic/enteric) | Haemorrhage |
| “Open packing” | |||
| Bradley 19937 | 71 | 46% | 7% |
| Branum 199818 | 50 | 88% (72%/16%) | – |
| Bosscha 199850 | 28 | 25% | 50% |
| “Planned re-laparotomies” | |||
| Sarr 199147 | 23 | (26%/52%) | 26% |
| Tsiotos 199820 | 72 | (19%/27%) | 18% |
| “Closed packing” | |||
| Fernandez-del C 199819 | 64 | (53%/16%) | 3% |
| “Closed Continuous Lavage” | |||
| Farkas 199652 | 123 | (13%/1%) | 2% |
| Büchler 2001 | 42 | 19% | 5% |
Figure 1.

Closed lavage of the debrided cavity. The lesser sac is opened and the greater omentum divided close to the gastroepiploic vessels. Four catheters are inserted (two from each side) for postoperative continuous lavage of the lesser sac. The tip of the catheters are placed at the tail of the pancreas and behind the descending colon, as well as at the head of the gland and behind the ascending colon.
Figure 2.

Closed lavage of the debrided cavity. The lesser sac is closed by suturing the greater omentum to the transverse colon for closed postoperative lavage.
The differing success reported by groups using apparently similar approaches illustrates the difficulties in comparing different or evolving techniques performed around the world. Most techniques have an average mortality of 15–25%. However, mortality in patients with established multiple organ failure is even higher.50 In the absence of randomised trials, it is impossible to determine the hidden effects of factors such as referral pattern, patient selection, comorbidity of patients, presurgical percutaneous management, and indication for surgery within the literature.
“Organ preserving necrosectomy is the surgical technique of choice for treatment of infected pancreatic and peripancreatic necrosis. Morbidity is low in techniques which provide postoperative exit channels for further slough and infected debris (continuous postoperative lavage, closed packing)”
Minimally invasive procedures for debridement of infected necrosis
The high mortality in infected pancreatic necrosis despite surgery has led to the development of several minimally invasive techniques, including radiological, endoscopic, and minimally invasive surgery, as alternative procedures. The rationale is to minimise peri- and postoperative stress in critically ill septic patients suffering from multiorgan failure. By this, the indication for intervention may be extended to patients who are otherwise unfit for surgery, although this has not been evaluated in systematic comparisons. Additionally, these techniques may be used to initially control sepsis and to delay surgery for better demarcation of necrotic tissue.
Percutaneous drainage
Interventional techniques have become increasingly important in recent years due to the now ubiquitous availability of CT scanning and ultrasonography. In 1998, Freeny et al reported for the first time a series of patients with infected acute necrotising pancreatitis who were exclusively drained by CT guided percutaneous catheter drainage.53 Earlier reports covered other infectious complications of acute pancreatitis,54 including infected pancreatic fluid collections, pseudocysts, or abscesses, as classified by the International Symposium on Acute Pancreatitis in Atlanta.7
Freeny and colleagues53 developed a technique of percutaneous drainage which not only drained infected necrosis passively but included necrosectomy by adding aggressive irrigation through large bore percutaneous catheters (28 F). Thirty four patients with necrotising pancreatitis and uncontrolled sepsis were treated. An average of three separate catheter sites per patient and four catheter exchanges per patient were necessary for the removal of necrotic material. Pancreatic surgery was avoided in 16 patients (47%), and sepsis was controlled in 25 patients (74%). Although nine of the latter group needed elective surgery, the surgical procedure could be avoided successfully in critically ill patients until stabilisation. Percutaneous drainage was ineffective in nine patients who needed surgery to control sepsis or bleeding (26%). The overall mortality was 12%. These four patients all were critically ill with multiorgan failure, bleeding, or shock. The recipe of success in this series was the commitment of the interventional radiologists (with often daily catheter interventions: 146 catheter exchanges, long duration of drainage of 25–152 days, no complications) and the improvement of the technique which enabled percutaneous necrosectomy. However, patients with central gland necrosis, who often present with disruption of the midsection of the main pancreatic duct resulting in a fistula, responded poorly to percutaneous drainage in the series from Seattle (cure in 4/14 (28%) and control of sepsis in 50%).
The radiological approach was taken to its limits by Gmeinwieser and colleagues.55 They combined percutaneous retroperitoneal necrosectomy, fragmentation of necrotic pancreatic and peripancreatic tissue with a snare catheter and Dormia baskets, continuous lavage of the cavity, and repeated bronchoscopic visualisation of the cavity with percutaneous blockade of a pancreatic duct disruption to successfully treat and avoid surgery in a young man with infected necrosis who strictly declined the surgical procedure recommended.
The same group created a technique to treat patients suffering from infected necrosis, primarily percutaneously, when signs of sepsis were present and intensive care treatment was unsuccessful. Large bore 20–28 F catheters were placed under CT and fluoroscopy guidance, routinely with a retroperitoneal approach from the left side (fig 3 ▶). Under fluoroscopy control, necrotic and solid material was fragmented and removed actively with aspiration, snares, and forceps, using peel away sheets (fig 4 ▶). Continuous lavage was performed using up to 12 litres of NaCl solution per day and additionally manual aspiration of solid material was performed on a daily basis.56 Twenty five of 29 patients treated by this method were successfully cured of sepsis and only three needed further elective surgery at a later time.57 Moreover, the intervention related complication rate was very low (table 4 ▶). Nine patients treated by this technique of percutaneous necrosectomy were re-evaluated after a median follow up period of 30 months with respect to quality of life, morphology, as well as endocrine and exocrine pancreatic function.58 All patients were in good general condition with respect to quality of life. Only 2/9 (22%) patients had moderate to marked changes in morphology, as observed on CT. There was mild to moderate exocrine dysfunction in 5/8 (63%) patients, and severe restriction of exocrine pancreatic function in 2/8 (25%). The oral glucose tolerance test was normal in 3/6 (50%) patients tested. One patient with diabetes in the oral glucose tolerance test had pre-existing type II diabetes requiring insulin therapy since the onset of acute pancreatitis. In 3/9 (33%) patients an oral glucose tolerance test was not performed due to known pre-existing diabetes.
Figure 3.

(A–D) Percutaneous necrosectomy in a 50 year old male with necrotising pancreatitis based on alcohol abuse. (A) Computed tomography (CT) scan before therapy revealed an acute necrotising pancreatitis showing typical findings such as peripancreatic fluid collections and pancreatic necrosis. (B) After CT guided placement of three 16 F catheters, contrast media was applied: filling defects represent solid necrotic tissue. In addition, there was a fistula between the necrotic cavity and the stomach, as indicated by contrast media within the stomach. (C) After percutaneous removal of necrotic tissue, the cavity decreased in size and demonstrated only a few small filling defects. (D) CT scan three years after necrosectomy: normal appearance of the pancreatic head. The pancreatic body and tail cannot be delineated, resulting in an anatomical situation such as after left sided surgical pancreatectomy.
Figure 4.
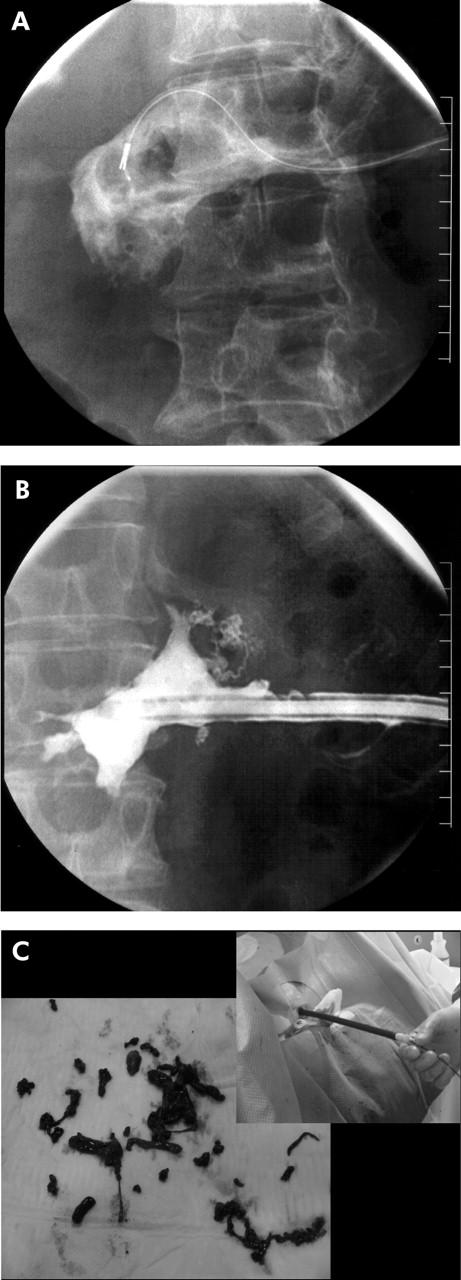
(A–C) Necrosis of the pancreatic body and tail: After installation of a 20 F peel away sheet, a snare catheter and a Dormia basket were inserted for necrosectomy (A). After necrosectomy, the necrotic cavity was reduced without any filling defects, which would represent residual necrosis (B). Macroscopic necrotic tissue was removed using the percutaneous technique of necrosectomy (C) described by Mann and colleagues.56
Table 4.
Outcome of percutaneous or endoscopic drainage
| Series | Patients (n) | Infected (%) | Mortality | Successful | Sepsis↓ | Complications |
| Percutaneous drainage | ||||||
| Gmeinwieser 199757 | 29 | 100% | 8 (27%) | 20 (69%) | 25 (86%) | Fistula 7% |
| Freeny 199853 | 34 | 100% | 4 (12%) | 16 (47%) | 25 (74%) | None |
| Echenique 199859 | 20 | 100% | 0 | 20 (100%) | – | Fistula 50% |
| Gouzi 199960 | 32 | 81% | 5 (15%) | 21 (65%) | Fistula 52% | |
| Szentkereszty 200161 | 24 | ? | 3 (12.5%) | 3 (12.5%) | 11 (45%) | None |
| Endoscopic drainage | ||||||
| Baron 199665 | 11 | 27% | 0 | 9 (81%) | Bleeding 9% | |
| Infection 36% |
Another series of catheter directed debridement of infected necrosis with a slightly different technique was published by Echenique and colleagues.59 The catheters used were smaller (14–16 F) but stone retrieval baskets and floppy tipped guidewires were used to break debris into smaller peaces. All 20 patients with infected necrosis were treated successfully with regard to clinical course and lesion appearance. Surgery was avoided, and no death occurred. Seven to 32 (average 17) episodes of debridement were necessary which were started on an inpatient basis and continued on an outpatient basis. Fistulas developed in 10 (50%; three to the bowel, seven to the pancreatic duct). However, all patients included in this trial were haemodynamically stable despite the presence of infected necrosis. Several other series have been published since, reporting different success rates (table 4 ▶).60–62 Again, it is almost impossible to compare these results with available data on surgical results secondary to the inhomogenity of the patient selection in the different series. Considering the publication bias for so called “negative studies”, it has to be concluded that percutaneous drainage of infected pancreatic necrosis is an option that works in the hands of some very dedicated specialists but is probably not a technique which can be recommended for routine use everywhere. Thus “can do” must be separated from “should do”. It may have a role as a temporary measure to bridge the critical early time after the onset of acute pancreatitis to a later optimal time point for definite intervention.61,63,64
Endoscopic therapy
Successful endoscopic drainage of symptomatic sterile or infected pancreatic necrosis was reported by Baron et al as early as 1996.65 The technique applied was originally described for uncomplicated pseudocysts. Several transgastric or transduodenal drainage catheters (10 F) and a nasopancreatic irrigation tube were endoscopically inserted into the retroperitoneum to perform necrosectomy. Lavage was continued until resolution of the collection. In this first report, 2–4 procedures were required for resolution and the mean duration of catheter placement was 19 days. Successful removal of necrosis was achieved in over 80% with no mortality. However, the majority of patients treated had no infected necrosis but residual fluid collections with debris. Almost 40% were iatrogenically infected secondarily by endoscopy. Moreover, there were serious complications in 45% of patients, including serious bleeding and gastric perforation (table 4 ▶). Additionally, it is worthy of note that up to 60% of those patients successfully drained developed further collections in the subsequent two years.66 Thus this series confirmed that in the presence of necrosis, drainage must be combined with some form of surgical removal of necrotic material. In 1999, Baron and Morgan described successful placement of percutaneous endoscopic jejunostomy tubes through a PEG tube and subsequently through a transgastric track into the necrotic pancreatic collections for irrigations in two cases.67 The theoretical advantages of this technique are that on the one hand it avoids the need for uncomfortable nasopancreatic catheters and on the other does not produce the side effects observed after percutaneous drainage, including skin irritation and external pancreatic fistulas.67
Although endoscopic drainage might be applicable in some patients with necrotising pancreatitis, only a few centres have used this technique. The results in infected necrosis are only anecdotal, experience with this method is limited, and no interdisciplinary comparative data exist.
Minimally invasive procedures
Advances in laparoscopic technology and instrumentation allow the utilisation of minimally invasive techniques for management in pancreatic disease, and theoretically lessen the surgical stress in the already compromised patient.
As early as 1996, Gagner described laparoscopic debridement and necrosectomy for the treatment of necrotising pancreatitis with three different minimally invasive approaches: (1) transgastric drainage, (2) retrogastric retrocolic debridement, and (3) a full retroperitoneoscopic technique.68 Since then, many different techniques have been applied by several groups in the search for the easiest access to the necrotic masses in the retroperitoneum.
The laparoscopic assisted transgastric approach is similar to the endoscopic approach and somehow identical to the approach using a PEG to access the stomach.67 Several case reports exist which describe successful laparoscopic transgastric pancreatic necrosectomy for infected necrosis, suggesting effective debridement and internal drainage in selected patients with this minimally invasive approach.69 However, no larger series have been reported.
Others have approached the infected necrosis with standard laparoscopy, combining necrosectomy with splenectomy and cholecystectomy.70 Zhu et al published their experience of the laparoscopic approach in 10 patients. Despite the fact that they included patients with acute haemorrhagic and necrotising pancreatitis without infection which do not need surgical intervention at all, their mortality was 10%.71 As almost every procedure can be performed laparoscopically, this approach has not been evaluated in any larger study or in prospective randomised trials. A theoretical risk is the spread of infection into the abdominal cavity, further intraoperative difficulties in case of reoperations, and enhanced risk of erosions of the intestinal tract.
In the late 1980s, the open retroperitoneal approach with lumbotomy was used to avoid these drawbacks.72–74 This open approach allowed exploration of the pancreas and manual removal of infected necrosis. Although the mortality rates for this retroperitoneal approach compared favourably with historical controls in the same hospitals, the technique has not gained popularity because of its high complication rates. In three series, mortality varied between 20% and 33%, and local complications, mainly enteric fistulas and bleeding, were observed in 20–50%. Fagniez et al reported major morbidity, including enteric fistula (45%), haemorrhage (40%), and colonic necrosis (15%). Thus the main drawback of this open retroperitoneal approach is its narrowness and blindness about the risk of damage to visceral organs and vessels. However, the improvement in CT in recent years with its exact information about the location of necrotic tissue eases the direct retroperitoneal approach. In fact, Nakasaki et al reported successful treatment of infected necrosis by retroperitoneal laparotomy even in patients who needed reoperations after laparotomy (table 5 ▶).75
Table 5.
Outcome of retroperitoneal laparostomy (open surgery)
In recent years, minimally invasive techniques using the theoretical advantages of retroperitoneal access have been developed.68,76 Most groups which apply minimally invasive surgery for infected necrosis today use this retroperitoneal approach.76–81 Despite small variations in the different techniques applied, they have in common that the infected necrosis of the retroperitoneum is accessed under endoscopic visualisation with subsequent necrosectomy and lavage. The techniques involve either intraoperative dilatation of a percutaneous drain tract which was applied by ultrasound or CT guidance preoperatively, or a direct approach of the infection with a retroperitoneoscope. Depending on the localisation of the infectious tissue, access can be gained from the left or right flank, and over one or more routes. While at first the technique was used in patients after laparotomy as a reoperation, it is now even advocated as a primary approach in some patients.77,79,80
Several reports show that the technique is applicable and that it can successfully treat some patients with infected necrosis. The results with regard to mortality and morbidity of the larger series published to date are presented in table 6 ▶. Morbidity ranges between 30% and 60%, the success rate for complete necrosectomy between 60% and 100%, and the mortality in these series between 0% and 27%. Although this seems to support the view that laparoscopic assisted necrosectomy is a safe alternative to open necrosectomy, the data have to be interpreted with caution. At first it is obvious that a careful case selection was performed in all trials and it is evident that the patients cannot be compared with those treated in series with open surgery. In the largest series published so far,80 only 24 of 45 patients were treated by minimally invasive retroperitoneal pancreatic necrosectomy. In the others, open surgery was performed for the following reasons: lack of a safe retroperitoneal guidewire access route, presence of an additional intra-abdominal complication, extensive paracolic necrotic extension, or multifocal necrotic foci. Moreover, three of the 24 attempted minimally invasive procedures could not be undertaken for technical reasons and another five required open surgery secondary to sepsis or bleeding after the initial minimally invasive approach. Thus only 35% (16 of 45) of all patients treated with necrosectomy were the right candidates for the retroperitoneoscopic technique. Although the proportion of patients undergoing minimally invasive necrosectomy increases over time with experience in the centres,77,80 many patients will not be treated successfully with this method. An additional disadvantage is the need for repeated procedures and subsequently an increase in the length of hospital stay with the minimally invasive procedures.76,80 This contrasts with the results of the open techniques which imply a postoperative method to continuously remove residual pancreatic necrosis to achieve complete removal of the infected necrosis with a single operation in the majority of cases. During laparoscopic assisted necrosectomy there is significant potential for major injury to intra-abdominal organs or vascular structures. Indeed, all reports show quite a high incidence of serious complications, including fistula (20%–60%) and bleeding (15%), despite the preselection of patients.
Table 6.
Outcome of minimally invasive surgery for necrosectomy
| Series | Patients &;(n) | Infected | Mortality | Successful | Morbidity |
| Laparoscopy | |||||
| Zhu 200171 | 10 | 0% | 10% | 90% | |
| Retroperitoneoscopy | |||||
| Gambiez 199876 | 20 | 65% | 10% | 75% | 60% |
| Carter 200077 | 10 | 100% | 20% | 80% | 28% |
| Horvath 200178 | 6 | 100% | 0 | 66% | 33% |
| Castellanos 200279 | 15 | 100% | 27% | – | 40% |
| Connor 200380 | 24 | 58% | 25% | 67% | 54% |
| Connor 2003 abstr81 | 36 | 76% | 22% | 69% | – |
Proponents of minimally invasive technologies in this clinical setting cite a desire to minimise the physiological insult in patients who are already critically ill. Although some investigators77,80 believe that a reduction in the deterioration in organ function and the need for postoperative intensive care management can be observed in patients treated with the minimally invasive techniques, no data exist to clearly demonstrate that minimally invasive procedures are less prone to morbidity than open surgery.
In conclusion, techniques for laparoscopic necrosectomy are still evolving. Safe retroperitoneal access and necrosectomy is possible in patients with infected necrosis but not all patients, depending on size and localisation of the infectious foci, can be treated successfully. No randomised studies exist comparing one management technique with another. All studies reported involved small numbers of patients, were analysed retrospectively, and comprised selected patients with great variation in comorbidities and disease severity. Consequently, it is not possible to draw any conclusions from the literature with regard to the best interventional or surgical approach for infected necrosis. However, in the absence of well designed clinical trials, we must be cautious in the application of new technologies. Technical feasibility does not obviate the need for scientific rigor and sound clinical judgement. Thus today, outside clinical trials, minimally invasive surgery should be limited to specific indications and to those patients who are critically ill and otherwise unfit for conventional surgery.
“Minimally invasive procedures, including percutaneous drainage, endoscopic drainage, or minimally invasive surgery (that is, retroperitoneoscopy) for infected pancreatic necrosis may play a role as a temporary measure to bridge the critical early time after onset of acute pancreatitis to a later optimal time point for definite intervention. Otherwise, they should be limited to specific indications in patients who are critically ill and unfit for conventional surgery or clinical trials”
MANAGEMENT OF COMPLICATIONS IN ACUTE PANCREATITIS
While surgery is still the “gold standard” for the treatment of infected necrosis, interventional intensive care is already established for the management of several complications of severe acute pancreatitis, including pancreatic fluid collections, pseudocysts, abscesses, as well as pancreatic fistulas, biliary leakages, and haemorrhage.
Pancreatic abscess
The most common complication requiring intervention after necrosectomy is a residual or recurrent infection, mostly pancreatic abscesses. These are probably a consequence of limited necrosis with subsequent liquefaction and secondary infection. In general, pancreatic abscesses develop later in the course of disease (usually after five weeks). Due to their less aggressive behaviour and circumscribed localisation, minimally invasive treatment strategies can be easily performed successfully in most of these cases.82,83 Percutaneous drainage is the treatment of choice for pancreatic abscesses and it is widely applied.13,19,20
Pancreatic pseudocysts and fistula
Disruption of the pancreatic duct secondary to pancreatic necrosis leads to an accumulation of pancreatic secretion, defined as pancreatic ascites or pseudocyst, or if it is drained, as a pancreatocutaneous fistula. While almost all peripheral leaks will seal in time, central defects will not resolve that easily, especially if there is no internal drainage via the pancreatic duct system into the duodenum. It is estimated that 50% of acute pseudocysts can be managed without any form of intervention, especially small (<6 cm) and asymptomatic lesions.84,85 If leaks do not resolve, the anatomy should be diagnosed with ERCP, magnetic resonance imaging, and fistulography. Today, surgery is rarely indicated but leaks from the tail may need resection while fistulas in the head or body of the pancreas, or those which are embedded in inflammatory mass, should be internalised with an anastomosis to a Roux-en-Y jejunal loop.85 However, endoscopic stenting or percutaneous drainage have to be recommended in the majority of cases.56,86–88 If communication with the ductal system is present, internal drainage is more effective; if communication is not present percutaneous drainage is indicated.85,89–91 Although the interventional methods are already established for these indications, these alternatives have not been compared with surgery in clinical trials.
Haemorrhage
Life threatening haemorrhage into the gastrointestinal tract, retroperitoneum, or peritoneal cavity complicates acute pancreatitis in only 1–3% of patients.92 Initiation of early and definitive therapy is the cornerstone of successful management. Pseudoaneurysms occur as a result of necrotic changes in the arterial wall secondary to contact with proteolytic enzymes and other products of pancreatic suppuration. Arterial proximity to a septic or inflammatory focus appears to be the only prerequisite to their formation. Selective angiography is the diagnostic “gold standard” for localising active bleeding due to vascular necrosis. While management of vascular complications had to be managed by surgical means in the past, the angiographic approach by catheter directed embolisation can be life saving.93 Haemorrhage is a rare complication of acute pancreatitis and includes bleeding pseodoaneurysms, diffuse bleeding from necrosis, and haemorrhagic pseudocysts.94 Several reports from recent years demonstrated that mesenteric angiography can detect the bleeding site in approximately 80% of cases95 and arterial embolisation can achieve definite haemostasis in 35–50%, and helps stabilise critically ill patients to permit elective surgery in another 10–20%.94,95 However, failure to correct the frequently associated infected pancreatic necrosis will lead to a high rate of recurrent haemorrhage.96 When emergency surgical intervention for haemorrhage is necessary, surgical ligation is sometimes impossible, and packing of the wound cavity may be necessary.93
“Interventional treatment is well established as the standard treatment for complications of acute pancreatitis, including peripancreatic fluid collections, pseudocysts, and late abscesses, as well as selective angiography and catheter directed embolisation of acute pancreatitis associated bleeding complications”
PROPHYLAXIS OF RECURRENT PANCREATITIS
Recurrence of acute pancreatitis in patients with gall stones has been reported in 29–63% of cases if the patient is discharged from hospital without additional treatment. The rationale for cholecystectomy and clearance of the main bile duct in these patients is to prevent potentially avoidable recurrent attacks. Today, laparoscopic cholecystectomy is recommended during the same hospital stay for mild disease and should be delayed until sufficient resolution of the inflammatory response and clinical recovery in severe pancreatitis.6,97,98 In patients who are unfit to undergo surgery, elective endoscopic sphincterotomy is an established and effective alternative to cholecystectomy to lower the risk of recurrent acute pancreatitis.6,15,99
“While laparoscopic cholecystectomy is the “gold standard” to avoid recurrence in patients with gall stone associated pancreatitis, ERCP and sphincterotomy are accepted alternatives in patients who are unfit for surgery”
Conflict of interest: None declared.
REFERENCES
- 1.Isenmann R, Beger H. Natural history of acute pancreatoitis and the role of infection. Baillieres Best Pract Res Clin Gastroenterol 1999;13:291–301. [DOI] [PubMed] [Google Scholar]
- 2.Klar E, Werner J. New pathophysiological findings in acute pancreatitis. Chirurgia 2000;71:253–64. [Google Scholar]
- 3.Buter A, Imrie C, Carter C, et al. Dynamic nature of early organ dysfunction determines outcome in acute pancreatitis. Br J Surg 2002;89:298–302. [DOI] [PubMed] [Google Scholar]
- 4.Gloor B, Muller CA, Worni M, et al. Pancreatic infection in severe pancreatitis: The role of fungus and multiresistent organisms. Arch Surg 2001;36:592–6. [DOI] [PubMed] [Google Scholar]
- 5.Dervenis C, Johnson CD, Bassi C, et al. Diagnosis, objective assessment of severity, and management of acute pancreatitis. Int J Pancreatol 1999;25:195–200. [DOI] [PubMed] [Google Scholar]
- 6.Uhl W, Warshaw A, Imrie C, et al. IAP Guidelines for the surgical management of acute pancreatitis. Pancreatology 2002;2:565–73. [DOI] [PubMed] [Google Scholar]
- 7.Bradley ELD. A clinically based classification system for acute pancreatitis. Summary of the International Symposium on Acute Pancreatitis, Atlanta, Ga, September 11–13, 1992. Arch Surg 1993;128:586–90. [DOI] [PubMed] [Google Scholar]
- 8.Johnson C, Kingsnorth A, Imrie C, et al. Double blind, randomised, placebo controlled study of a platelet activating factor antagonist, lexipafant, in the treatment and prevention of organ failure in predicted severe acute pancreatitis. Gut 2001;48:62–9. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 9.Norman J . The role of cytokines in the pathogenesis of acute pancreatitis. Am J Surg 1998;175:76–83. [DOI] [PubMed] [Google Scholar]
- 10.Werner J, Z’Graggen K, Fernandez-del Castillo C, et al. Specific therapy for local and systemic complications of acute pancreatitis with monoclonal antibodies against ICAM-1. Ann Surg 1999;229:834–40. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 11.Beger HG, Bittner R, Block S, et al. Bacterial contamination of pancreatic necrosis—a prospective clinical study. Gastroenterology 1986;91:433–41. [DOI] [PubMed] [Google Scholar]
- 12.Tenner S, Sica G, Hughes M, et al. Relationship of necrosis to organ failure in severe acute pancreatitis. Gastroenterology 1997;113:899–903. [DOI] [PubMed] [Google Scholar]
- 13.Buchler MW, Gloor B, Müller CA, et al. Acute necrotizing pancreatitis: treatment strategy according to the status of infection. Ann Surg 2000;232:619–26. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 14.Isenmann R, Rau B, Beger H. Bacterial infection and extent of necrosis are determinants of organ failure in patients with acute necrotizing pancreatitis. Br J Surg 1999;86:1020–4. [DOI] [PubMed] [Google Scholar]
- 15.United Kingdom guidelines for the management of acute pancreatitis. Gut 1998;42:1–13. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 16.Werner J, Uhl W, Büchler M. Surgical treatment of acute pancreatitis. Curr Treat Options Gastroenterol 2003;6:359–68. [DOI] [PubMed] [Google Scholar]
- 17.Hartwig W, Maksan S, Foitzik T, et al. Reduction in mortality with delayed surgical therapy of severe pancreatitis. J Gastrointest Surg 2002;6:481–7. [DOI] [PubMed] [Google Scholar]
- 18.Branum G, Galloway J, Hirchowitz W, et al. Pancreatic necrosis: results of necrosectomy, packing, and ultimate closure over drains. Ann Surg 1998;227:870–7. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 19.Fernandez-del Castillo C, Rattner DW, Makary MA, et al. Debridement and closed packing for the treatment of necrotizing pancreatitis. Ann Surg 1998;228:676–84. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 20.Tsiotos GG, Luque-de Leon E, Sarr MG. Long-term outcome of necrotizing pancreatitis treated by necrosectomy. Br J Surg 1998;85:1650–3. [DOI] [PubMed] [Google Scholar]
- 21.Banks S . Clinical course of acute pancreatitis: what has chamged in recent years? In: Buchler M, Uhl W, Friess H, et al, eds. Acute pancreatitis, novel concepts in biology and treatment. Berlin-Vienna: Blackwell Science, 1999:163–9.
- 22.Mier J, Leon E, Castillo A, et al. Early versus late necrosectomy in severe necrotzing pancreatitis. Am J Surg 1997;173:71–5. [DOI] [PubMed] [Google Scholar]
- 23.Sigurdson G . Acute pancreatitis: therapeutic options in multiple organ failure. In: Büchler M, Uhl W, Friess H, et al, eds. Acute pancreatitis: novel concepts in biology and therapy. Oxford: Blackwell Science Ltd, 1999:395–410.
- 24.Werner J, Klar E. Effective treatment regimens in the management of acute pancreatitis. Chir Gastroenterol 1999;15:328–33. [Google Scholar]
- 25.Buchler M, Malfertheiner P, Friess H, et al. The penetration of antibiotics into human pancreas. Infection 1989;17:20–5. [DOI] [PubMed] [Google Scholar]
- 26.Golub R, Siddiqi F, Pohl D. Role of antibiotics in acute pancreatitis: a meta-analysis. J Gastrointest Surg 1998;2:496–503. [DOI] [PubMed] [Google Scholar]
- 27.Sharma VK, Howden CW. Prophylactic antibiotic sepsis and mortality in acute necrotizing pancreatitis: a meta-analysis. Pancreas 2001;22:28–31. [DOI] [PubMed] [Google Scholar]
- 28.Buchler MW, Binder M, Friess H, et al. Potential role of somatostatin and octreotide in the management of acute pancreatitis. Digestion 1994;55 (suppl 1) :16–19. [DOI] [PubMed] [Google Scholar]
- 29.Uhl W, Büchler M, Malfertheiner P, et al. A randomised, double blind, multicentre trial of octreotide in moderate to severe acute pancreatitis. Gut 1999;45:97–104. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 30.Imrie C, Benjamin I, Ferguson J, et al. A single center double blind trial of Trasylol therapy in primary acute pancreatitis. Br J Surg 1978;65:337–41. [DOI] [PubMed] [Google Scholar]
- 31.Fan ST, Lai EC, Mok FP, et al. Early treatment of acute biliary pancreatitis by endoscopic papillotomy. N Engl J Med 1993;328:228–32. [DOI] [PubMed] [Google Scholar]
- 32.Fölsch UR, Nitsche R, Ludtke R, et al. Early ERCP and papillotomy compared with conservative treatment for acute biliary pancreatitis. The German Study Group on Acute Biliary Pancreatitis. N Engl J Med 1997;336:237–42. [DOI] [PubMed] [Google Scholar]
- 33.Neoptolemos JP, Carr-Locke DL, London N, et al. ERCP findings and the role of endoscopic sphincterotomy in acute gallstone pancreatitis. Br J Surg 1988;75:954–60. [DOI] [PubMed] [Google Scholar]
- 34.Kelly T, Wagner D. Gallstone pancreatitis: a prospective randomized trial of the timing of surgery. Surgery 1988;104:600–5. [PubMed] [Google Scholar]
- 35.Neoptolemos J, Shaw D, Carr-Locke D. A multivariate analysis of preoperative risk factors in patients with common bile duct stones. Implication for treatment. Ann Surg 1989;209:157–61. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 36.Heath D, Alexander D, Wilson C, et al. Which complications of acute pancreatitis are most lethal? A prospective multicenter clinical study of 719 episodes. Gut 1995;36:478. [Google Scholar]
- 37.Neoptolemos JP, Raraty M, Finch M, et al. Acute pancreatitis: the substantial human and financial cases. Gut 1998;42:886–91. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 38.Gloor B, Müller C, Worni M, et al. Late mortality in patients with severe acute pancreatitis. Br J Surg 2001;88:975–9. [DOI] [PubMed] [Google Scholar]
- 39.Bradley A, Allen K. A prospective longitudinal study of observation versus surgical intervention in the management of necrotizing pancreatitis. Am J Surg 1991;161:19–24. [DOI] [PubMed] [Google Scholar]
- 40.Widdison AL, Karanjia ND. Pancreatic infection complicating acute pancreatitis. Br J Surg 1993;80:148–54. [DOI] [PubMed] [Google Scholar]
- 41.Gerzof SG, Banks PA, Robbins AH, et al. Early diagnosis of pancreatic infection by computed tomography-guided aspiration. Gastroenterology 1987;93:1315–20. [DOI] [PubMed] [Google Scholar]
- 42.Banks P, Gerzof S, Langevin R, et al. CT-guided aspiration of suspected pancreatic infection: bacteriology and clinical outcome. Int J Pancreatol 1995;18:265–70. [DOI] [PubMed] [Google Scholar]
- 43.Hiatt J, Fink A, King W, et al. Percutaneous aspiration of peripancreatic fluid collections: a safe method to detect infection. Surgery 1987;101:523–30. [PubMed] [Google Scholar]
- 44.Rau B, Pralle U, Mayer J, et al. Role of ultrasonographically guided fine-needle aspiration cytology in the diagnosis of infected pancreatic necrosis. Br J Surg 1998;85:179–84. [DOI] [PubMed] [Google Scholar]
- 45.Kivilaakso E, FRaki O, Nikki P .et al. Resection of the pancreas for fulminant pancreatitis. Surg Gynecol Obstet 1981;152:493–8. [PubMed] [Google Scholar]
- 46.Bradley ELd. Management of infected pancreatic necrosis by open drainage. Ann Surg 1987;206:542–50. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 47.Sarr MG, Nagorney DM, Mucha P Jr, et al. Acute necrotizing pancreatitis: management by planned, staged pancreatic necrosectomy/debridement and delayed primary wound closure over drains. Br J Surg 1991;78:576–81. [DOI] [PubMed] [Google Scholar]
- 48.Beger HG, Buchler M, Bittner R, et al. Necrosectomy and postoperative local lavage in necrotizing pancreatitis. Br J Surg 1988;75:207–12. [DOI] [PubMed] [Google Scholar]
- 49.Beger H, Krautzberger W, Bittner R, et al. Necrotizing pancreatitis. Indications for operation and results in 118 patients. Chirurg 1982;53:870–7. [PubMed] [Google Scholar]
- 50.Bosscha K, Hulstaert P, Hennipman A, et al. Fulminant acute pancreatitis and infected necrosis; results of open management of the abdomen and “planned” reoperations. J Am Coll Surg 1998;187:255–62. [DOI] [PubMed] [Google Scholar]
- 51.Nieuwenhuijs V, Besselink M, van Minnen L, et al. Surgical management of acute necrotizing pancreatitis: a 13-year experience and a systematic review. Scand J Gastroenterol 2003;239:111–16. [DOI] [PubMed] [Google Scholar]
- 52.Farkas G, Marton J, MAndi Y .et al. Surgical treatment and management of infected pancreatic necrosis. Br J Surg 1996;83:890–3. [DOI] [PubMed] [Google Scholar]
- 53.Freeny P, Hauptmann E, Althaus S, et al. Percutaneous CT-guided catheter drainage of infected acute necrotizing pancreatitis: techniques and results. Am J Roentgenol 1998;170:969–75. [DOI] [PubMed] [Google Scholar]
- 54.Gerzof S, Robbins A, Johnson W, et al. Percutaneous catheter drainage of abdominal abscesses. N Engl J Med 1981;305:653–7. [DOI] [PubMed] [Google Scholar]
- 55.Gmeinwieser J, Holstege A, Zirngibl H, et al. Successful percutaneous treatment of infected necrosis of the body of the pancreas associated with segmental disruption of the main pancreatic duct. Gastrointest Endosc 2000;52:413–15. [DOI] [PubMed] [Google Scholar]
- 56.Mann S, Gmeinwieser J, Schmidt J, et al. Possibilities and borderlines of interventional therapy in necrotizing pancreatitis. Zentralbl Chir 2001;126:15–22. [DOI] [PubMed] [Google Scholar]
- 57.Gmeinwieser J, Feuerbach S, Zirngibl H, et al. Percutaneous treatment of infected necrotizing pancreatitis. Eur IHPBA 1997;23:575–8. [Google Scholar]
- 58.Endlicher E, Völk M, Feuerbach S, et al. Long-term follow-up of patients with necrotizing pancreatitis treated by percutaneous necrosectomy. Hepatogastroenterology 2003;50:2225–2228. [PubMed] [Google Scholar]
- 59.Echenique A, Sleeman D, Yrizarry J, et al. Percutaneous catheter-directed debridement of infected pancreatic necrosis: results in 20 patients. J Vasc Intervent Radiol 1998;9:565–71. [DOI] [PubMed] [Google Scholar]
- 60.Gouzi J, Bloom E, Julio C, et al. Percutaneous drainage of infected pancreatic necrosis: an alternative to surgery. Chirurgie 1999;124:31–7. [DOI] [PubMed] [Google Scholar]
- 61.Szentkereszty Z, Kerekes L, Hallay J, et al. CT guided percutaneous drainage in the treatment of acute necrotizing pancreatitis. Magyar Sebeszet 2001;54:11–14. [PubMed] [Google Scholar]
- 62.Kam A, Markson G, Wong K, et al. Inappropiate use of percutaneous drainage in the management of pancreatic necrosis. J Gastroenterol Hepatol 1999;14:699–704. [DOI] [PubMed] [Google Scholar]
- 63.Rattner DW, Legermate DA, Lee MJ, et al. Early surgical debridement of symptomatic pancreatic necrosis is beneficial irrespective of infection. Am J Surg 1992;163:105–9. [DOI] [PubMed] [Google Scholar]
- 64.Müller P . Percutaneous drainage of pancreatic necrosis. AJRAm J Roentgenol 1998;170:976–7. [DOI] [PubMed]
- 65.Baron T, Thaggard W, Morgan D, et al. Endoscopic therapy for organized pancreatic necrosis. Gastroenterology 1996;111:755–64. [DOI] [PubMed] [Google Scholar]
- 66.Adkinson K, Morgan D, Baron TH. Long term outcome following successful endoscopic drainage of organized pancreatic necrosis. Gastrointest Endosc 1997;45:514. [Google Scholar]
- 67.Baron T, Morgan D. Endoscopic transgastric irrigation tube placement via PEG fordebridement of organized pancreatic necrosis. Gastrointest Endosc 1999;50:574–7. [DOI] [PubMed] [Google Scholar]
- 68.Gagner M . Laparoscopic treatment of acute necrotizing pancreatitis. Semin Laparosc Surg 1996;3:21–8. [DOI] [PubMed] [Google Scholar]
- 69.Ammori B . Laparoscopic transgastric pancreatic necrosectomy for infected pancreatic necrosis. Surg Endosc 2002;16:1362–5. [DOI] [PubMed] [Google Scholar]
- 70.Hamad G, Broderick T. Laparoscopic pancreatic necrosectomy. J Laparoendosc Adv Surg Tech 2000;10:115–18. [DOI] [PubMed] [Google Scholar]
- 71.Zhu J, Fan X, Zhang X. Laparoscopic treatment of severe acute pancreatitis. Surg Endosc 2001;15:146–8. [DOI] [PubMed] [Google Scholar]
- 72.Fagniez P, Rotman N, Kracht M. Direct retroperitoneal approach to necrosis in severe acute pancreatitis. Br J Surg 1989;76:264–7. [DOI] [PubMed] [Google Scholar]
- 73.Villazon A, Villazon O, Terrazas F, et al. Retroperitoneal drainage in the management of the septic phase of severe acute pancreatitis. World J Surg 1991;15:103–8. [DOI] [PubMed] [Google Scholar]
- 74.Van Vyve E, Reynaert M, Lengele B, et al. Retroperitoneal laparostomy: a surgical treatment of pancreatic abscess after an acute necrotizing pancreatitis. Surgery 1993;111:369–75. [PubMed] [Google Scholar]
- 75.Nakasaki H, Tajimi T, Fujii K, et al. A surgical treatment of infected pancreatic necrosis: retroperitoneal laparotomy. Dig Surg 1999;16:506–11. [DOI] [PubMed] [Google Scholar]
- 76.Gambiez L, Denimal F, Porte H, et al. Retroperitoneal approach and endoscopic management of peripancreatic necrosis collections. Arch Surg 1998;133:66–72. [DOI] [PubMed] [Google Scholar]
- 77.Carter C, McKay CJ, Imrie C. Percutaneous necrosectomy and sinus tract endoscopy in the management of infected pacreatic necrosis: an initial experience. Ann Surg 2000;232:175–80. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 78.Horvath K, Kao L, Ali A, et al. Laparoscopic assisted percutaneous drainage of infected pancreatic necrosis. Surg Endosc 2001;15:677–82. [DOI] [PubMed] [Google Scholar]
- 79.Castellanos G, Pinero A, Serrano A, et al. Infected pancreatic necrosis: translumbar approach and management with retroperitoneoscopy. Arch Surg 2002;137:1060–2. [DOI] [PubMed] [Google Scholar]
- 80.Connor S, Ghaneh P, Raraty M, et al. Minimally invasive retroperitoneal pancreatic necrosectomy. Dig Surg 2003;20:270–7. [DOI] [PubMed] [Google Scholar]
- 81.Connor S, Ghaneh P, Raraty M, et al. Is minimally invasive retroperitoneal pancreatic necrosectomy better than open necrosectomy? Pancreas 2003;27:374 (abstract). [DOI] [PubMed] [Google Scholar]
- 82.Van Sonnenberg E, Wittich G, Chon K, et al. Percutaneous radiologic drainage of pancreatic abscesses. AJR Am J Roentgenol 1997;168:979–84. [DOI] [PubMed] [Google Scholar]
- 83.Mithofer K, Mueller PR, Warshaw AL. Interventional and surgical treatment of pancreatic abscess. World J Surg 1997;21:162–8. [DOI] [PubMed] [Google Scholar]
- 84.Yeo CJ, Bastidas JA, Lynch-Nyhan A, et al. The natural history of pancreatic pseudocysts documented by computed tomography. Surg Gynecol Obstet 1990;170:411–17. [PubMed] [Google Scholar]
- 85.Werner J, Warshaw A. Cystic disease of the pancreas: Pseudocysts, postinflammatory cystic fluid collections, and other non-neoplastic cysts. In: Trede M, Carter D, eds. Surgery of the pancreas. New York: Churchill Livingstone, 1997:405–15.
- 86.VanSonnenberg E, Wittich G, Casola G. Percutaneous drainage of infected and noninfected pancreaticpseudocysts: experience in 101 cases. Radiology 1989;170:757–61. [DOI] [PubMed] [Google Scholar]
- 87.Naoum E, Zavos A, Goudis K, et al. Pancreatic pseudocysts: 10 years of experience. J Hepatobiliary Pancreat Surg 2003;10:373–6. [DOI] [PubMed] [Google Scholar]
- 88.Ferrucci J, Müller P. Interventional approach to pancreatic fluid collections. Radiol Clin North Am 2003;41:1217–226. [DOI] [PubMed] [Google Scholar]
- 89.Tsiotos C, Sarr M. Management of fluid collections and necrosis in acute pancreatitis. Curr Gastroenterol Rep 1999;1:139–44. [DOI] [PubMed] [Google Scholar]
- 90.Zein C, Baron T, Morgan D. Endoscopic pancreaticoduodenostomy for treatment of pancreatic duct disconnection because of severe acute pancreatitis. Gastrointest Endosc 2003;58:130–4. [DOI] [PubMed] [Google Scholar]
- 91.Nealon W, Walser E. Main pancreatic duct anatomy can direct choice of modality for treating pancreatic pseudocysts. Ann Surg 2002;235:751–8. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 92.Stroud W, Cullom J, Anderson M. Hemorrhagic complications of severe pancreatitis. Surgery 1981;90:658–64. [PubMed] [Google Scholar]
- 93.Bradley E . Complications of acute pancreatitis and their management. In: Trede M, Carter D, eds. Surgery of the pancreas. New York: Churchill Livingstone, 1997:275–88.
- 94.Balthazar E, Fisher L. Hemorrhagic complications of pancreatitis: radiologic evaluation with emphasis on CT imaging. Pancreatology 2001;1:306–13. [DOI] [PubMed] [Google Scholar]
- 95.Beattie G, Hardman J, Redhead D, et al. Evidence for central role of selective mesenteric angiography in the management of the major vascular complications of pancreatitis. Am J Surg 2003;185:96–102. [DOI] [PubMed] [Google Scholar]
- 96.Waltman A, Luers P, Athanasoulis C, et al. Massive arterial hemorrhage in patients with acute pancreatitis: complementary roles of surgery and transcatheter occlusive techniques. Arch Surg 1986;121:439–47. [DOI] [PubMed] [Google Scholar]
- 97.Uhl W, Mueller C, Krahenbuhl L, et al. Acute gallstone-pancreatitis: timing of laparoscopic cholecystectomy in mild and severe disease. Surg Endosc 1999;13:1070–6. [DOI] [PubMed] [Google Scholar]
- 98.Tang E, Stain S, Tang G, et al. Timing of laparoscopic surgery in gallstone pancreatitis. Arch Surg 1995;130:496–9. [DOI] [PubMed] [Google Scholar]
- 99.Uomo G, Manes G, Laccetti M, et al. Endoscopic sphincterotomy and recurrence of acute pancreatitis in gallstone patients considered unfit for surgery. Pancreas 1997;14:28–31. [DOI] [PubMed] [Google Scholar]