1. Vitamin D Synthesis
For the majority of the population the principle source of vitamin D is synthesis following exposure of the skin to UVB radiation [290-315 nm] [
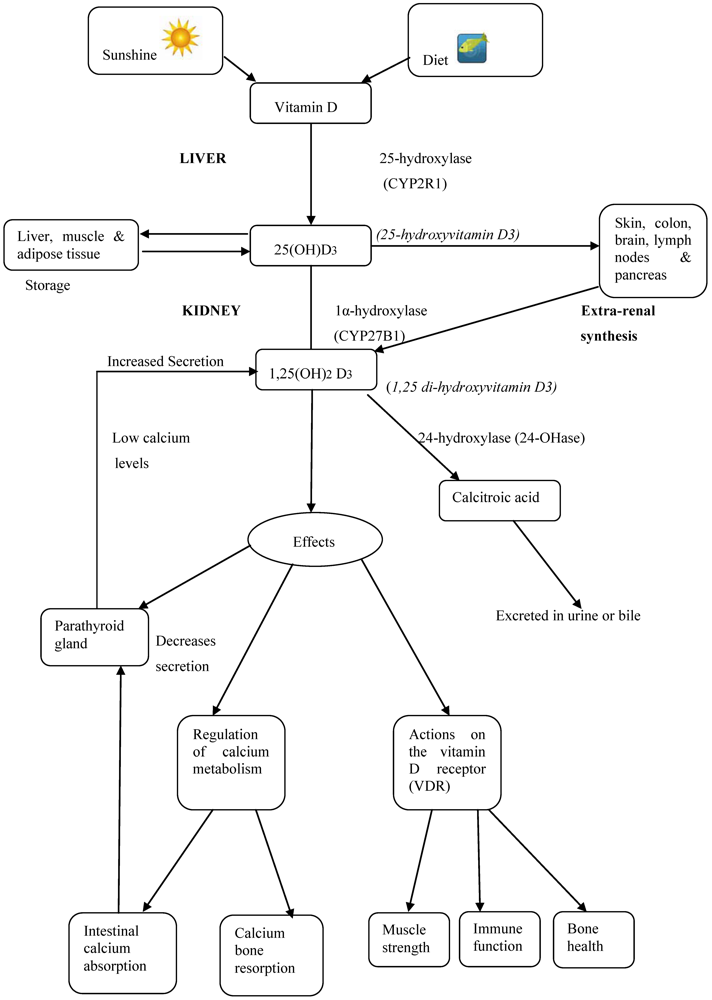
1]. UVB radiation acts in the upper epidermis of the skin with 7-dehydrocholestrol converted to pre-vitamin D3 by photolysis of the B ring structure followed by isomerisation [
1]. These structural modifications mean that the molecule no longer conforms within the plasma membrane and is ejected into the extra-cellular space and drawn into the capillary beds where it is bound by the vitamin D binding protein [DBP] and transported to the liver [
1]. Maximal production of vitamin D is reached after 10-15 minutes of sun exposure in summer [
2] depending on skin pigmentation [
3] and during this period one erythaema dose is achieved which is the equivalent to an intake of over 500µg of vitamin D3 [
4]. Further UVB exposure results in the formation of in-active photoproducts such as tachysterol and lumisterol that have negligible effects on calcium metabolism [
4] and prevent vitamin D toxicity from sun exposure.
Geographical location is a key determinant of the efficiency of vitamin D synthesis as production is dependent on the angle of sunlight or the solar zenith angle [
5]. As latitude increases, the amount of light within the wavelength range 290-315 nm to reach the earth’s surface decreases owing to an increased pathway of transversion and ozone absorption. Therefore, at locations above 35° latitude, the synthesis of vitamin D is seasonal with maximal amounts made during summer and little or no synthesis occurring during winter. Synthesis can also be affected by lifestyle, environmental, and physiological factors. Lifestyle factors such as the use of sun-screen, time spent outside and wearing of clothing significantly affect UVB exposure as do environmental factors such as pollution, cloud cover and ozone presence [
6,
7,
8]. For example a sun protective factor [SPF] sunscreen of 15, if correctly applied, would decrease vitamin D synthesis to 1/15th or about 7% [
6]. Also a recent cross-sectional study investigating the vitamin D status of 34 children [9-24 months old] living in a polluted area of Delhi reported that pollution reduced vitamin D serum concentrations by 50% [
9]. Physiological differences such as skin complexion and age also affect synthesis: darker skin has significantly higher melanin content and subsequently requires a higher UVB exposure time than paler skin to synthesize an equivalent amount of vitamin D [
10]. Increasing age is associated with a significant decrease in the amount of 7-dehydrocholesterol in the skin and thus, a reduction in vitamin D synthesis with studies reporting up to four times less cutaneous synthesis in adults aged over 70 years compared to a 20 year old adult [
11].
2. Dietary Sources
Vitamin D is also obtained to a limited extent from the diet, albeit few dietary sources naturally contain the vitamin in sufficient quantities to make a significant contribution to requirements. The two main vitamin D secosteroids within the diet are vitamin D2 [ergocalciferol] and vitamin D3 [cholecalciferol]. Vitamin D2 is derived from plant and fungi and is produced through the irradiation of ergosterol. Vitamin D3, as previously mentioned, is produced from 7-dehydrocholesterol and is obtained in the diet from animal products with oily fish, fish oils, eggs and dairy produce providing the best dietary sources. A recent double blind, placebo controlled study reported that there is no significant difference in the effectiveness of the two isomers [
12]; however it is more often reported that vitamin D3 is the more effective. This higher effectiveness of vitamin D3 over D2 is owing to a possible increased affinity for the vitamin D binding protein [DBP] [
13,
14] leading to a reduction in clearance of D3 and providing longer lasting concentrations of 25(OH)D in the blood than D2 [
14].
In relation to intakes, the composition of the habitual diet will impact on vitamin D status. For example, within Ireland the majority of vitamin D intakes are from sources such as meat and meat products [
15] which contain low concentrations of the vitamin. Rich food sources such as oily fish are consumed infrequently. Few vitamin D fortified foods, aside from margarine, are available within Western Europe possibly owing to early adverse advent incidents of infantile hypercalcaemia attributed to over-fortification of dried milk with vitamin D [
16]. Other countries, including the USA fortify foods; however, surveys have suggested significant differences between the actual and reported levels of fortification [
17,
18]. Vitamin D absorption occurs in the ileum and jejunum. It has been estimated that 75% is effectively absorbed [
19] but efficiency is dependent on bile salt and micelle formation and, therefore, the presence of malabsorptive disorders such as Coeliac [
20] or Crohn’s disease [
21] can significantly affect absorption and thus status [
22].
4. Vitamin D Intake and Status
Until recently, it was generally assumed that enough vitamin D was synthesized from sun exposure to meet requirements and no recommendations for dietary intakes for adults aged 18-65 yrs were set. However, research highlighting the effects of low vitamin D status [
26,
27] has indicated the importance of vitamin D in the diet. Within Ireland, the Food Safety Authority for Ireland [FSAI] has set a wide range of 0-10 μg/d (day) for adults [
28] while in the UK there is no reference nutrient intake [RNI] for adults [18-64 yrs], only for those over 65 yrs [10 μg/d] and pregnant and lactating women [10 μg/d] [29]. In the US, adequate intakes [AI] are set at 5 μg/d [19-50 yrs] and 10 μg/d [51-70 yrs] [
30] which also correspond with the WHO/FAO Expert Group recommended intakes [
31].
The difficulty in assigning a RNI for vitamin D intake is exacerbated by the current lack of agreement on optimal vitamin D status. While vitamin D deficiency is generally accepted as a 25[OH]D3 serum concentration <25 nmol/L [
32], the serum concentrations of 25[OH]D3 defining insufficiency, or optimal status are less clear. Insufficiency can be deemed as mild deficiency with a 25[OH]D3 serum concentration <50 nmol/L [
33,
34,
35]. Over extended periods of time, insufficiency has been associated with increased bone loss and secondary hyperparathyroidism leading to increased fracture risk [
36]. Sufficiency has been regarded as the point at which further intakes will have no additional beneficial effects on PTH and calcium metabolism in regard to bone health. However, the cut-off values for sufficiency are still under debate. Studies have demonstrated concentrations of >80 nmol/L [
37] or higher, 100-200 nmol/L [
35], as optimal.
As mentioned earlier, the dietary intake of vitamin D required to prevent vitamin D deficiency and ensure optimal vitamin D status will vary depending on sun exposure preferences. A recent study concluded that to maintain 25[OH]D >25 nmol/L in 97.5% of the population during wintertime the recommended dietary allowances [RDA] should be set at 8.7ug/d. However, the authors also calculated that a dietary intake of 12.1ug/d would be required to prevent deficiency among sun avoiders [
38]. Such intakes are considerably higher than estimated vitamin D intakes in Ireland [3.3 µg] [
39], the UK [4.2 µg] [
40], the US [8.12 µg] [
41] and other European countries [
42,
43,
44].
Vitamin D toxicity is rare [
45]. The symptoms include vomiting, nausea, constipation, weight loss, weakness and kidney stones with subsequent hypercalcaemia and ectopic calcification of soft tissue [
46]. However, as discussed earlier, the formation of vitamin D from sunlight is a self-limiting reaction; thus preventing toxicity from sun exposure. Reports of toxicity have arisen from excessive dietary intakes of the vitamin [
17,
47,
48,
49] with all such cases reporting serum 25[OH]D concentrations >200 nmol/L. However, severe adverse effects have only been reported with extreme intakes of vitamin D of 15,000 µg/d [
47,
48] or 42,000 µg/d [
49], well above any natural intakes from food or supplements from clinical trials.
5. Vitamin D and Bone Health
Peak bone mass is attained by the third decade of life [
50] with genetics, physical activity, nutrition and lifestyle factors [
51,
52] playing key roles in the accumulation and maintenance of bone. Age related bone loss occurs around the fourth decade [
53], resulting in a gradual decline of BMD though this process is accelerated in females during and up to 10 years post-menopause owing to possible oestrogen deficiency derived bone loss [
54]. The development of bone disease in later life is related to the attainment of maximum peak bone mass and the maintenance of bone mass in adulthood [
55]. In relation to vitamin D, research has shown that inadequate vitamin D intakes over long periods of time can lead to bone demineralization [
56]. Vitamin D deficiency leads to decreased calcium absorption and ultimately the release of calcium from the bones in order to maintain circulating calcium concentrations [
56]. Continuous bone turnover and resorption weakens the architecture of bones and increases fracture risk via secondary hyperparathyroidism [
56] ultimately leading to the development of osteomalacia and osteoporosis. Osteoporosis is clinically defined as a BMD 2.5 standard deviations below the mean of healthy young individuals [
57,
58].
There is a direct relationship between BMD and fracture risk [
59], with a decrease in bone strength and density associated with an increased incidence rate of fractures [
60].Fractures usually occur at the hip, spine and wrist [
61] and not only carry considerable health costs, but can also result in increased mortality and a decreased quality of life [
62,
63,
64]. Fracture incidence has been shown to increase with age [
65]; therefore it has been imperative to develop preventive strategies in order to minimize the development of this condition. Given the relationship between vitamin D and bone mineralization, optimal vitamin D status is essential for minimization of fracture risk.
6. Fracture Risk
A number of studies have investigated the effects of vitamin D or vitamin D in combination with calcium on fracture incidence (
Table 1,
Table 2,
Table 3). Three intervention trials of vitamin D alone [
66,
75,
77] have reported a significant reduction in fracture occurrence. For example, one study [
75] reported a 33% lower rate for fracture and a 22% lower rate for first fracture at any site compared to placebo in free-living individuals with 100,000 IU D3. While in another intervention [
66], which supplemented with 150,000-300,000 IU D2, an apparent significant fracture reduction from baseline was reported, especially in the upper limb both in free-living and institutionalized subjects [though this study had no placebo and was not blinded]. Furthermore, in a trial [
77] supplementing post-stroke elderly patients with 1000 IU D2, zero hip fractures were reported in the vitamin D arm (n = 48). These results are also supported by trials with vitamin D in combination with calcium. For example, in one study [
89], supplementation with 400 IU D3 and calcium resulted in a reduction in the fracture incidence rate of community dwelling individuals. Furthermore, another trial [
81] reported a significant reduction in hip fractures among institutionalized elderly females supplemented with calcium and vitamin D3 for two years. A subsequent analysis of the same cohort after 42 months supplementation indicated that hip fractures and non-vertebral fractures remained lower in the treatment group [
94]. However, not all trials of vitamin D or vitamin D in combination with calcium have reported significant effects. For example, Lyons
et al. [
79] in a double-blinded, placebo-controlled trial, supplemented nursing home residents with 100,000 I.U D2 quarterly for five years and reported no significant reduction in fractures. Moreover, in a much larger trial [
92] of 36,000 subjects with 400 IU D3 & 500 mg calciumno significant reduction in fractures was reported. The difference in outcomes between trials is difficult to explain, albeit there are a number of possible explanations for lack of reported effects. A large number of trials [
69,
71,
74,
76,
85,
87,
88,
91,
92,
93] have supplemented with between 300-800 IU vitamin D which may not be enough to exert a beneficial effect according to a recent meta-analysis [
95,
96]. In addition, studies which have documented significant fracture reductions have reported that effects may be more evident among institutionalized elderly people compared to free-living individuals.
These observations are supported by a number of meta-analyses. Bischoff-Ferrari (2005) conducted a meta-analysis [
97] of 7 RCTs and concluded vitamin D in the range of 700-800 IU/d reduced the risk of hip/non-vertebral fractures by 25% while a calcium intake of more than 700 mg/d was required for non-vertebral fracture prevention. In a separate analysis [
98], an 18% reduction in hip fracture risk and a significant reduction in non-vertebral fractures were achieved with vitamin D and calcium supplementation. It has also been reported that vitamin D and calcium intervention is more effective in reducing the risk of hip fracture in patients in institutionalized care compared to free living individuals in the community [
94,
95] with more than 800 IU vitamin D and more than 1200 mg calcium daily required respectively to exert a beneficial effect. In keeping with this finding of a threshold effect of vitamin D, a more recent analysis [
99] concluded that supplementation with 400 IU/d or less was ineffective while doses between 482-770 IU/d reduced fractures [hip 18%, non-vertebral 20%] with no further effect with additional calcium supplementation. Conversely, a recent Cochrane analysis concluded that vitamin D alone did not have a significant effect on fracture prevention and was only effective when combined with calcium in institutionalized individuals [
100]. This finding is supported by a recent pooled analysis of over 68,000 patients which reported that 400-800 IU/d of vitamin D alone was not effective but 400 IU/d combined with calcium reduced the rate of hip fracture by 16% and reduced overall fractures by 8% [
101]. Two meta-analyses to date [
99,
102] have looked at the effect of vitamin D analogues with one concluding that calcitriol & alfacalcidol were more effective at reducing fracture risk than D2 or D3 [
102]. The use of such analogues, however, is not widely advocated at present given the potential risks and cost implications associated with them [
99].
Taken together, the results from the meta-analyses support a cause and effect relationship between vitamin D in combination with calcium in the reduction of risk of vertebral and non-vertebral osteoporotic fractures. Several mechanisms may underlie this positive association between vitamin D and fracture risk including the well documented beneficial effects of vitamin D on bone mineral density.
Table 1.
Intervention with vitamin D on fracture prevention.
Table 1.
Intervention with vitamin D on fracture prevention.
| Study | Study design | n | Sex | Mean age [years] | Treatment | Length | Results |
|---|
| CT, controlled trial;OSD, open study design trial; F, female; M, male; D3, cholecalciferol; D2, ergocalciferol; Ca, calcium;/d, daily; mths, months; yrly, yearly; IU, International units |
| Heikinheimo et al. 1992 (66) | CT | 320 | M/F | 75-84 | 150,000-300,000 IUD2 yrly | 5 yrs | Groups with vitamin D had sig lower rate of fractures, |
| | | 479 | M/F | >85 | 150,000-300,000 IU D2 yrly | 5 yrs | particularly upper limb but not lower limb fractures |
| Lips et al. 1996 (69) | CT | 2578 | M/F | 80 | 400 IU D3/d | 3.5 yrs | No effect |
| Peacock et al. 2000 (71) | CT | 438 | M/F | 74 | 800 IU D3/d | 4 yrs | No effect |
| Meyer et al. 2002 (74) | CT | 1144 | M/F | 84 | 400 IU D3/d | 2 yrs | No effect |
| Trivedi et al. 2003 (75) | CT | 2686 | M/F | 75 | 100 000 IU D3 four monthly | 5 yrs | 33% lower rate for fracture at hip, forearm and vertebrae |
| Grant et al. 2005 (76) | CT | 2675 | M/F | 77 | 800 IU D3/d | 2 yrs | No effect |
| Sato et al. 2005(77) | CT | 96 | F | 74 | 1, 000 IU D2/d | 2 yrs | Reduction in hip fracture |
| Law et al. 2006 (78) | OSD | 3717 | M/F | 85 | 1,100 IU D2/d | 10 mths | No effect |
| Lyons et al. 2006 (79) | CT | 3440 | M/F | 84 | 100 000 IU D2 four monthly | 3 yrs | No effect |
| Smith et al. 2007 (80) | CT | 9440 | M/F | 79 | 300 000 IU D2/d | 3 yrs | No effect |
Table 2.
Interventionwith vitamin D plus calcium on fracture prevention.
Table 2.
Interventionwith vitamin D plus calcium on fracture prevention.
| Study | Study design | n | Sex | Mean age [years] | Treatment | Length | Results |
|---|
| CT, controlled trial;OSD, open study design trial; F, female; M, male; D3, cholecalciferol; D2, ergocalciferol; Ca, calcium;/d, daily; yr, year; yrs, years |
| Chapuy et al. 1992 (81) | CT | 3270 | F | 84 | 800 IU D3 & 1200 mg Ca/d | 2 yrs | Hip fractures 43% & non-vertebral fractures 32% lower |
| Dawson Hughes et al. 1997 (84) | CT | 389 | M/F | 71 | 700 IU D3 & 500 mg Ca/d | 3 yrs | Reduction in non-vertebral fractures |
| Komulainen et al. 1999 (85) | CT | 464 | F | 52 | 300 IU D3 (100 IU in last yr) & 93 mg Ca/d | 5 yrs | Noeffect |
| Chapuy et al. 2002 (87) | CT | 583 | F | 85 | 800 IU D3 & 1200 mg Ca/d | 2 yrs | No effect |
| Harwood et al. 2004 (88) | OSD | 76 | F | 82 | 800 IU D3 & 1000 mg Ca/d | 1 yr | No effect |
| Larsen et al. 2004 (89) | CT | 9605 | M/F | 74 | 400 IU D3 & 1000 mg Ca/d | 3 yrs | 16% reduction in fracture risk |
| Flicker et al. 2005 (90) | CT | 625 | M/F | 83 | 10,000 IU D2 wk to 1000 IU/d& 600 mg Ca/d | 2 yrs | No effect |
| Porthouse et al. 2005 (91) | OSD | 3314 | F | 70 | 800 IU D3 & 1000 mg Ca/d | 25 mths | No effect |
| Grant et al. 2005 (76) | CT | 2638 | M/F | 77 | 800 IU D3 & 1000 mg Ca/d | 2 yrs | No effect |
| Jackson et al. 2006 (92) | CT | 36282 | F | 62 | 400 IU D3 & 500 mg Ca/d | 7 yrs | No effect |
| Pfeifer et al. 2009 (93) | CT | 242 | M/F | 77 | 800 IU D3/1000 mg Ca/d | 2 yrs | No effect |
Table 3.
Intervention with vitamin D analogues (with / without calcium) on fracture incidence.
Table 3.
Intervention with vitamin D analogues (with / without calcium) on fracture incidence.
| Study | Study design | n | Sex | Mean age (years) | Treatment | Length | Results |
|---|
| CT, controlled trial; F, female; M, male; Cl, Calcitriol; Ac, Alfacalcidol; Ca, Calcium; /d, daily; wkly, weekly; yr, year;yrs, years |
| Vitamin D analogues | | | | | | | |
| Hayashi et al. 1992 (67) | CT | 740 | M/F | 75 | 40 IU Ac/d | 1 yr | Lower fracture incidence |
| Tyliard et al. 1992 (68) | CT | 622 | F | 63 | 20 IU Cl/d | 3 yrs | Reduction in vertebral fractures |
| Sato et al. 1999 (70) | CT | 86 | M/F | 70 | 40 IU Ac/d | 2 yrs | 17.5% lower fracture rate |
| Ebeling et al. 2001 (72) | CT | 41 | M | 57.5 | 20 IU Cl/d | 2 yrs | No effect |
| Gallagher et al. 2001 (73) | CT | 489 | F | 72 | 20 IU Cl/d | 2 yrs | No effect |
| Vitamin D analogues with calcium | | | | | | | |
| Orimo et al. 1994 (82) | CT | 80 | F | 70 | 40 IU Ac & 300mg Ca/d | 1 yr | Decreased vertebral fracture incidence |
| Shikari et al. 1996 (83) | CT | 113 | F | 70 | 30 IU Ac & 300mg Ca/d | 2 yrs | Decreased incidence of fractures |
| Stempfle et al. 1999 (86) | CT | 132 | M/F | 50 | 10 IU Cl & 1000mg Ca/d | 3 yrs | No effect |
7. Vitamin D and BMD
A number of cross-sectional studies have investigated the relationship between vitamin D status and BMD. For example, one study [
103] of middle aged women reported that serum concentrations of 25[OH]D were positively related to bone density of the lumbar spine, neck and trochanteric regions of the femur. In addition, a more recent study [
104] reported a positive association of vitamin D and BMD and suggested the effect may be even greater in the 90-100 nmol/L serum range of vitamin D. Given the observed relationship between vitamin D status and BMD, a large number of intervention studies have investigated the effects of vitamin D alone or vitamin D in combination with calcium on BMD (
Table 4,
Table 5,
Table 6).
Vitamin D alone and in combination with calcium appears to have a clear significant effect on BMD. For example, 5 out of 9 studies of vitamin D alone [
70,
73,
105,
106,
107], plus 16 of 22 studies [
81,
84,
88,
92,
94,
98,
110,
111,
112,
116,
117,
118,
120,
122] of vitamin D in combination with calcium have reported significant positive effects on BMD. For example, in supplementation with vitamin D alone, one study [
107] reported a significant benefit after only five weeks in participants with impaired vitamin D status and osteoporosis/osteopenia. Supplementation with 100 000 IU D2 resulted in rapid improvement in vitamin D status and significant improvement in spinal and the femoral neck BMD. The findings are supported by another trial [
106] of over 300 elderly mobile females in whom two years of vitamin D3 supplementation resulted in significant improvements in BMD. The improvements in BMD can also be seen in the trials with vitamin D and calcium. Over the last 20 years, 14 intervention studies examining the effect of vitamin D and calcium supplementation on BMD have been published. Overall, positive results have been reported, with doses more than 400 IU associated with significant effects on bone heath. However, the optimal dosage of vitamin D remains unclear. For example, two trials [
117,
120] which supplemented with 560 IU D3 & 1000 mg calcium/d [
117] or 560 IU D3 and 500 mg Ca/d [
120] reported increases in lumbar spine BMD while conversely; another trial [
115] supplementing with 500 IU D3 and 1000 mg calcium/d over the same intervention period reported no significant effect. Four trials have reported significant increases in BMD with 700 IU [
84,
112] to 800 IU [
81,
88] D3 and calcium [500-1,200 mg]; however, in a study that supplemented African-American females with 800 IU D3 and 1,200-1,500mg of calcium [
121] no significant effects were reported. The findings in African-American females could be explained, in part, by lower bone remodelling rates [
124] and enhanced skeletal resistance to the effects of PTH [
125] in this population group. Studies intervening with higher doses of vitamin D have also produced conflicting results.For example, one trial [
120], supplementing with 1428 IU D2 and 1000 mg calcium/d reported no effect while another [
123] supplementing 5000 IU D3/d with 320mg calcium reported significant effects. In the latter trial, 45 elderly participants were supplemented with vitamin D3 through bread fortification. An impressive 4% increase in spine and 23.4% in hip BMD were reported. Trials (
Table 5) supplementing with vitamin D analogues have also reported significant improvements in BMD. For example, in one trial [
73], 20 IU alone resulted in a significant increase in spine BMD. Trials [
98,
99,
111,
116,
118,
119] with vitamin D analogues and calcium have also reported consistent results with the majority reporting significant improvements in BMD [
70,
73,
98,
99,
111,
116,
118,
119].
Vitamin D alone and in combination with calcium appears to have a clear significant effect on BMD. For example, 5 out of 9 studies of vitamin D alone [
70,
73,
105,
106,
107], plus 16 of 22 studies [
81,
84,
88,
92,
94,
98,
110,
111,
112,
116,
117,
118,
120,
122] of vitamin D in combination with calcium have reported significant positive effects on BMD. For example, in supplementation with vitamin D alone, one study [
107] reported a significant benefit after only five weeks in participants with impaired vitamin D status and osteoporosis/osteopenia. Supplementation with 100 000 IU D2 resulted in rapid improvement in vitamin D status and significant improvement in spinal and the femoral neck BMD. The findings are supported by another trial [
106] of over 300 elderly mobile females in whom two years of vitamin D3 supplementation resulted in significant improvements in BMD. The improvements in BMD can also be seen in the trials with vitamin D and calcium. Over the last 20 years, 14 intervention studies examining the effect of vitamin D and calcium supplementation on BMD have been published. Overall, positive results have been reported, with doses more than 400 IU associated with significant effects on bone heath. However, the optimal dosage of vitamin D remains unclear. For example, two trials [
117,
120] which supplemented with 560 IU D3 & 1000 mg calcium/d [
117] or 560 IU D3 and 500 mg Ca/d [
120] reported increases in lumbar spine BMD while conversely; another trial [
115] supplementing with 500 IU D3 and 1000 mg calcium/d over the same intervention period reported no significant effect. Four trials have reported significant increases in BMD with 700 IU [
84,
112] to 800 IU [
81,
88] D3 and calcium [500-1,200 mg]; however, in a study that supplemented African-American females with 800 IU D3 and 1,200-1,500mg of calcium [
121] no significant effects were reported. The findings in African-American females could be explained, in part, by lower bone remodelling rates [
124] and enhanced skeletal resistance to the effects of PTH [
125] in this population group. Studies intervening with higher doses of vitamin D have also produced conflicting results.For example, one trial [
120], supplementing with 1428 IU D2 and 1000 mg calcium/d reported no effect while another [
123] supplementing 5000 IU D3/d with 320mg calcium reported significant effects. In the latter trial, 45 elderly participants were supplemented with vitamin D3 through bread fortification. An impressive 4% increase in spine and 23.4% in hip BMD were reported. Trials (
Table 5) supplementing with vitamin D analogues have also reported significant improvements in BMD. For example, in one trial [
73], 20 IU alone resulted in a significant increase in spine BMD. Trials [
98,
99,
111,
116,
118,
119] with vitamin D analogues and calcium have also reported consistent results with the majority reporting significant improvements in BMD [
70,
73,
98,
99,
111,
116,
118,
119].
In summary, the majority of vitamin D supplementation trials demonstrate a positive effect of the vitamin on BMD and in de facto fracture incidence although further studies are required to confirm the optimal dose of vitamin D associated with these benefits. Moreover, although the potential benefits of vitamin D on fracture incidence may be at least partly attributed to beneficial effects on BMD, vitamin D may also impart advantages by reducing fracture occurrence through other mechanisms. One such mechanism is based on the potential of vitamin D to enhance muscle strength and thereby decrease the risk of falls.
8. Vitamin D and Muscle Strength
A recent review [
126] concluded that falls were the biggest contributor to fractures and observational studies have reported that vitamin D deficiency is associated with muscle weakness [
127] and an increased pre-disposition for falling [
128]. Such associations are not surprising given that research has shown that the VDR is expressed in both skeletal muscle [
129] and myoblast cells [
130].
In vitro evidence has demonstrated that vitamin D can increase protein synthesis and cellular growth in muscle cells with an increase in size and number of type 2 muscle fibres [
131] which are of particular importance as these are the first muscle fibres recruited when falling [
132]. In support of these findings, a recent observational study [
133] has reported vitamin D plasma concentrations in the range of 40-90nmol/L was associated with improved musculoskeletal function than serum concentrations <40nmol/L. Additionally, another study [
134] has suggested that impaired muscle function in vitamin D deficient subjects could be present even before indications of bone disease have been recognised. Such evidence clearly provides a mechanism to support an improvement in muscle strength and in defacto bone health following vitamin D supplementation.
A number of intervention trials have investigated the effects of vitamin D supplementation on muscle with contrasting results. One of the earliest supplementation studies reported that 40 IU alfacalcidol administered over a period of between 3 and 6 months increased the size and number of type 2 muscle fibres [
131]; however, a subsequent study using a lower dose [20 IU alfacalcidol] for three years reported no effect of supplementation on muscle strength [
135]. In the later study, baseline vitamin D status was reported at 60nmol/L, potentially reducing any likely beneficial effect of supplementation. Furthermore, a single 300,000 IU dose of vitamin D3 failed to exert a beneficial effect in frail elderly individuals, even in those deficient in vitamin D [
136]. In contrast, Sato
et al. [
77] reported that daily supplementation with 1000 IU vitamin D2 for two years produced a significant increase in type 2 muscle fibre diameter in hospitalized elderly females with post-stroke hemiplegia. More recently, two studies have reported significant associations with vitamin D and muscle strength [
137,
138] with one study reporting a significant association between vitamin D and lower extremity function. The observed beneficial effects of vitamin D on muscle could be explained by its modulating effects on PTH as hyperparathyroidism has been reported to induce muscle weakness and atrophy of type 2 muscle fibres in animal models [
139]. The observations, in turn, could be explained by the promoting effects of PTH on pro-inflammatory cytokines [
140], which are often considered co-factors for muscle wasting and disability, especially in older individuals [
141]. For example, PTH has been shown to increase production of IL-6
in vivo [
140], which has been linked with muscle weakness and bone resorption.
Table 4.
Intervention with vitamin D (with / without calcium) on bone mineral density (BMD).
Table 4.
Intervention with vitamin D (with / without calcium) on bone mineral density (BMD).
| Study | Study design | n | Sex | Mean age (years) | Treatment | Length | Results |
|---|
| CT, controlled trial; SAD, single arm den; OSD, open study design; F, female; M, male; D3, cholecalciferol; D2, ergocalciferol; Ca, calcium;/d, daily; wkly, weekly; mths, months; Inc., increase yr, year; yrs, years *added calcium supplements to ensure intakes were 1200-1500 mg/d |
| Vitamin D | | | | | | | |
| Nordin et al. 1985 (105) | CT | 109 | F | 65-74 | 15,000 IU D2 wkly | 2 yrs | Reduced rate of metacarpal cortical bone loss |
| Ooms et al. 1995 (106) | CT | 348 | F | 80 | 400 IU D3/d | 2 yrs | Inc. in BMD; femoral neck; 1.9% in left, 2.6% in right |
| Adams et al. 1999 (107) | IT | 12 | F | 60 | 100 000 IU D2/wkly | 5 weeks | Inc. in BMD; femoral neck (4.9%) & spine (4.1%) |
| Hunter et al. 2000 (108) | CT | 128 | F | 58.7 | 800 IU D3/d | 2 yrs | No effect |
| Peacock et al. 2000 (71) | CT | 438 | M/F | 74 | 800 IU D3/d | 4 yrs | No effect |
| Patel et al. 2001(109) | CT | 70 | F | 47.2 | 800 IU D3/d | 2 yrs | No effect |
| Vitamin D with calcium | | | | | | | |
| Dawson Hughes et al. 1991(110) | CT | 249 | F | 81 | 400 IU D3 & 377 mg Ca/d | 1 yr | Reduced winter time bone loss/improved BMD of spine |
| Chapuy et al. 1992 (81) | CT | 3270 | F | 84 | 800 IU D3 & 1200 mg Ca/d | 2 yrs | BMD of femur increased by 2.7% compared to placebo |
| Dawson Hughes et al. 1995 (112) | CT | 247 | F | 63 | 700 IU D3 & 500 mg Ca/d | 3 yrs | 1.5% inc. in BMD in femoral neck in 700 IU group only |
| Adachi et al. 1995 (113) | CT | 62 | M/F | 64 | 7142 IU D3 & 1000 mg Ca/d | 35mths | No effect |
| Bernstein et al. 1996 (114) | CT | 24 | M/F | 35 | 250 IU D3 & 1000 mg Ca/d | 1yr | No effect |
| Buckley et al. 1996 (115) | CT | 66 | M/F | 52 | 500 IU D3 & 1000 mg Ca/d | 2 yrs | No effect |
| DawsonHughes et al. 1997 (84) | CT | 389 | M/F | 71 | 700 IU D3 & 500 mg Ca/d | 3 yrs | Inc. in BMD |
| Baeksgaard et al. 1998(117) | CT | 240 | F | 62.5 | 560 IU D3 & 1000 mg Ca/d | 2 yrs | 1.6% inc. in lumbar spine BMD |
| Komulainen et al. 1999 (85) | RT | 464 | F | 52 | 300 IU C/c/d (100IU D3/d 5th year) & 93 mg Ca/d | 5 yrs | No effect |
| Cooper et al. 2003(120) | CT | 187 | F | 56 | 1,428 IU D2 & 1000 mg Ca/d | 2 yrs | No effect |
| Meier et al. 2004 (121) | OSD | 55 | M/F | 56 | 500 IU D3 & 500 mg Ca/d | 2 yrs | 0.8 % inc. in lumbar spine BMD |
| Harwood et al. 2004 (88) | OSD | 76 | F | 82 | 800IU D3 & 1000 mg Ca/d | 1 yr | Change in Hip BMD |
| Aloia et al. 2005 (122) | CT | 280 | F | 50-75 | 800 IU D3/d (2000IU after 2yrs) | 3 yrs | No effect |
| Jackson et al. 2006 (92) | CT | 36282 | F | 62 | 400 IU D3 & 500 mg Ca/d | 7 yrs | Change in Hip BMD (+1.06% compared to placebo) |
| Mocanu et al. 2009 (123) | SAD | 45 | M/F | 71 | 5000 IU D3/d & 320 mg Ca/d | 1 yr | 4% inc. lumbar spine & 23.4% inc. hip BMD |
Table 5.
Intervention with vitamin D analogues (with / without calcium) on BMD.
Table 5.
Intervention with vitamin D analogues (with / without calcium) on BMD.
| Study | Study design | n | Sex | Mean age (years) | Treatment | Length | Results |
|---|
| CT, controlled trial; F, female; M, male; Cl, Calcitriol; Ac, Alfacalcidol; Ca, Calcium;/d, daily; wkly, weekly;mths, months; yr, year; yrs, years |
| Vitamin D analogues | | | | | | | |
| Sato et al. 1999 (70) | CT | 86 | M/F | 70 | 40 IU Ac/d | 2 yrs | Decreased loss of BMD compared to placebo |
| Ebeling et al. 2001 (72) | CT | 41 | M | 57.5 | 20 IU Cl/d | 2 yrs | No effect |
| Gallagher et al. 2001 (73) | CT | 489 | F | 72 | 20 IU Cl/d | 2 yrs | Increase in spine BMD |
| Vitamin D analogues with calcium | | | | | | | |
| Sambrook et al. 1993 (111) | CT | 103 | M/F | 46 | 24 IU Cl & 1000 mg Ca/d | 1 yr | Reduced corticosteroid bone loss in the lumbar spine. |
| Orimo et al. 1994 (98) | CT | 80 | F | 70 | 40 IU Ac & 300 mg Ca/d | 1 yr | Increase in lumbar spine (L2-L4) BMD in 0.65% |
| Shikari et al. 1996 (99) | CT | 113 | F | 70 | 30 IU Ac & 300 mg Ca/d | 2 yrs | Increase in lumbar spine (L2-L4) BMD (1.81-2.32%) |
| Sato et al. 1997 (116) | CT | 64 | M/F | 68 | 40 IU Cl & 300 mg Ca/d | 6 mths | Improvement in BMD on intact side of stroke subjects |
| Lambrinoudaki et al. 1999 (118) | CT | 81 | F | 31 | 20 IU Cl & 1200 mg Ca/d | 2 yrs | Increase in BMD at lumbar spine |
| Stempfle et al. 1999 (86) | CT | 132 | M/F | 50 | 10 IU Cl & 1000 mg Ca/d | 3 yrs | No effect |
| Sambrook et al. 2000 (119) | CT | 65 | M/F | 46 | 20-30 IU Cc & 600 mg Ca/d | 2 yrs | Reduced bone loss in proximal femur |
Therefore, though studies to date have been conflicting, vitamin D supplementation has the potential to positively benefit muscle function which could subsequently lead to a decreased propensity to fall and fracture.
9. Falls and Vitamin D
Given the potential for vitamin D to modulate muscle strength, it is perhaps not surprising that a large number of studies which have investigated the effects of intervention with vitamin D alone or in combination with calcium on risk of falls [
Table 6,
Table 7]. Of six trials that have supplemented with vitamin D alone, two [
77,
143] have reported significant reductions in fall rate following supplementation with vitamin D at 1000 or 800IU of vitamin D2/d respectively. Importantly, however, seven out of nine studies [
89,
144,
145,
146,
147,
148,
149] that supplemented with vitamin D in combination with calcium have reported significant reductions in falls. Therefore, as with fracture prevention, vitamin D appears to be more effective in reducing the risk of falls when used in combination with calcium. Significantly, one meta-analysis of 5 RCTs [
150] concluded that vitamin D reduced the risk of falling by 22% while another more recent meta-analysis [
151] of eight RCTs concluded that supplementation with vitamin D in the region of 700-1,000 IU/d reduced falls by 19% with doses below this level ineffective. It has been suggested that vitamin D supplementation exerts greater effects on institutionalized
versus free-living individuals [
145], a finding which may be explained by a number of factors. Individuals in care typically have lower serum concentrations of vitamin D compared to free-living individuals [
152] leaving them pre-disposed to muscle weakness and increased risk of falling and also more likely to benefit from supplementation. Furthermore, compliance with the supplementations regimen may be better among institutionalised individuals where supplements are provided by caregivers. Nevertheless, not all trials of institutionalized individuals have produced significant findings [
78].
In summary, based on the evidence reported, vitamin D, particularly when supplemented with calcium, can have a beneficial effect on the prevention of falls and thus fractures.
Table 6.
Intervention with vitamin D or vitamin D analogues on falls.
Table 6.
Intervention with vitamin D or vitamin D analogues on falls.
| Study | Study design | n | Sex | Mean age (years) | Treatment | Duration | Results |
|---|
| CT, controlled trial; F, female; M, male; D3, cholecalciferol; D2, ergocalciferol;Ac, Alfacalcidol /d, daily; wkly, weekly; Ca, calcium; |
| Graafmans et al. 1996 (142) | CT | 354 | M/F | >70 | 400 IU D3/d (2 yrs) | 7 mths | No effect on falls |
| Sato et al. 1999 (70) | CT | 86 | M/F | 70 | 40 IU Ac/d | 2 yrs | No effect on falls |
| Latham et al. 2002 (136) | CT | 243 | M/F | 79 | 300,000 IU D3 once | 6 mths | No effect on falls |
| Trivedi et al. 2003 (75) | CT | 2686 | M/F | 75 | 100,000 IU D3 quartley | 5 yrs | No effect on falls |
| Sato et al. 2005 (77) | CT | 96 | F | 74 | 1,000 IU D2/d | 2 yrs | 59% reduction in falls and increase in size/number type 2 muscle |
| Law et al. 2006 (78) | OSD | 3717 | M/F | 85 | 1,100 IU D2/d | 10 mths | Noeffect |
| Broe et al. 2007 (143) | CT | 124 | M/F | 89 | 800 IU D2/d | 5 mths | 72% lower fall rate |
Table 7.
Intervention with vitamin D or vitamin D analogues (with / without calcium) on falls.
Table 7.
Intervention with vitamin D or vitamin D analogues (with / without calcium) on falls.
| Study | Study design | n | Sex | Mean age (years) | Treatment | Duration | Results |
|---|
| CT, controlled trial; F, female; M, male; D3, cholecalciferol; D2, ergocalciferol;Ac, Alfacalcidol /d, daily; wkly, weekly; Ca, calcium;*changed to 1000 IU D2 daily with 600 mg calcium |
| DawsonHughes et al. 1997 (84) | CT | 389 | M/F | >65 | 700 IU D3/ 500 mg Ca/d | 3 yrs | No effect on falls |
| Pfeifer et al. 2000(144) | CT | 148 | F | 70-86 | 800 IU D3/1,200 mg Ca/d | 2 mths | Reduced body sway (9%) and 1 yr follow up lower number of falls |
| Chapuy et al. 2002 (87) | CT | 583 | F | 85 | 800IU D3/1200 mg Ca/d | 2 yrs | No effects on falls |
| Larsen et al. 2002 (89) | IT | 5771 | F | 74 | 400 IU D3/1000 mg Ca/d | 3.5yrs | Reduced risk of severe falling by 12% |
| Bischoff et al. 2003 (145) | CT | 122 | F | >65 | 800IU D3/1200 mg Ca/d | 12 wks | 49% reduction in falling and improved muscoskeletal function |
| Dukas et al. 2004(146) | CT | 378 | M/F | 75 | 40 IU Ac/d | 9 mths | Reduction in falls only with Ca intake >512 mg/d in addition |
| Flicker et al. 2005 (147) | CT | 625 | M/F | 83 | 10,000 IU D2/wkly* | 2 yrs | Reduction in incidence ratio for falls |
| Bischoff et al. 2006 (148) | CT | 445 | M/F | >65 | 700 IU D3/500 mg Ca/d | 3 yrs | 46% reduction falls in womem (65% reduction in non-active women) |
| Pfeifer et al. 2009 (149) | CT | 242 | M/F | >70 | 800 IU D3/1000mg Ca/d | 18 mths | 27% reduction in falls & 28% decrease in body sway |
10. Bone Health, Vitamin D and Inflammation
Increasing age is not only associated with a decrease in BMD and muscle strength but is also associated with marked changes in immune and inflammatory responses. Studies conducted predominantly in individuals >70 y of age have demonstrated that, while the most striking age-related changes have been observed in the cell-mediated arm of the immune system, age-associated restructuring of the immune system is a consequence of alterations in virtually all of its components.These alterations result in the up-regulation of some components of the immune system as well as diminished function of others [
153,
154]. Changes include decreased mature lymphocyte function, decreased replication of hematopoietic cells [
153] and an up-regulation in the production of pro-inflammatory cytokines such as interleukin 6 [IL-6] and tumour necrosis factor-alpha [TNF-α] [
154].
Inflammation is considered a characteristic of osteoporosis [
155] and research has focused on the effects of cytokines on bone metabolism [
156]. The cytokines IL-1, IL-6 and TNF-α have been shown to regulate bone [
157] and evidence from animal models has suggested that these cytokines are associated with the development of osteoporosis [
154,
155] through stimulation of osteoclastogenesis and subsequent bone resorption [
158].
In vitro studies have indicated that TNF-α and IL-1 can stimulate human osteoclastic bone resorption [
159], possibly owing to increased RANKL expression in a synergistic relationship; with TNF-α depending on the presence of IL-1 for optimal osteoclast formation [
160].
To date, of the pro-inflammatory markers related to bone, the most studied is IL-6, the production of which can be stimulated by PTH [
161]. However, findings from
in vitro studies have been inconsistent, with reports that IL-6 stimulates both bone formation [
162] and resorption [
163]. Human studies have also produced inconsistent results on the relationship between IL-6 and bone health. A recent longitudinal study [
164], reported that baseline IL-6 and change in IL-6 over a period of 2.9 years were consistently associated with bone loss in elderly adults. These findings are supported by a similar study in post-menopausal women [
165]. Two other cross-sectional studies found no significant association between IL-6 and BMD [
166,
167] and another longitudinal study reported a positive association between IL-6 and bone loss in the lumbar spine [
168]. The associations between other cytokines and bone health have also been assessed; TNF-α is associated with bone resorption [
169], as is IL-17, which is reported to act synergistically with TNF-α to promote bone turnover in rheumatoid arthritis patients [
170]. Conversely, some animal studies have suggested that IL-17 is protective in oestrogen-derived bone loss which commonly occurs during the menopause [
171].
The relationship between polymorphisms in cytokine genes, which alter expression of the particular cytokine, and bone health has been investigated with varying results. Polymorphisms in the IL-1 receptor antagonist [IL-1ra] gene in post-menopausal women have been associated with lower BMD and increased fracture risk [
172,
173]; however, such associations with this polymorphism are not evident in all trials [
174]. Other polymorphisms that have been identified include the 174 GG polymorphism in IL-6; this polymorphism results in a higher expression of IL-6 protein and has been associated with increased bone resorption [
175]. This particular polymorphism has also been reported as a potential risk factor for hip fracture among late postmenopausal women without oestrogen replacement therapy and those with inadequate calcium intakes [
176]. Studies have also indicated that polymorphisms in the TNFRSF1B gene, which codes for a TNF receptor, also contain polymorphisms which show associations with BMD [
177,
178]. This relationship between bone and cytokines is further strengthened by another study which reported that a polymorphism in transforming growth factor [TGF]-β1 is associated with increased bone mass and is less common in individuals with osteoporotic fractures [
173].
Evidence from both epidemiological and observational studies has highlighted the immunoregulatory effects of vitamin D; research suggesting a potential role for the vitamin in the management of immunological disorders such as multiple sclerosis [
179] and rheumatoid arthritis [
180]. The VDR are located in of a variety of immune cells, including monocytes and macrophages [
181]. Following binding of 1,25 [OH]
2D to the VDR, monocyte and macrophage activity is up regulated enhancing the host defences and an immunosuppressive effect is observed in lymphocytes decreasing the activity of T and B cells [
182]. A number of studies have reported that vitamin D, in the form of 1,25[OH]
2D3, can down regulate cytokine production. For example,
in vitro studies have reported a significant decrease in IL-6 and TNF-α with vitamin D [
183,
184].
In vivo studies have also reported positive associations. For example, Zhu
et al [
185] investigated an animal model of inflammatory bowel disease and reported that vitamin D, in the form of 1,25[OH]
2D, downgraded the production of TNF-α. This finding is supported by other studies investigating clinical populations which have reported positive effects of vitamin D supplementation on cytokine profiles in patients with congestive heart failure [
186] and multiple sclerosis [
187]. Moreover, in relation to bone health, one study has investigated the potential of vitamin D to alter cytokine production in individuals at increased risk of fracture and concluded that 20 IU/day of calcitriol for 6 months decreased both IL-1 and TNF-α concentrations and increased BMD in post-menopausal women with osteoporosis [
188].
In summary, while not assessed in the majority of vitamin D intervention studies to date, it is possible given the immunoregulatory effects of vitamin D together with the reported inflammatory aetiology of osteoporosis, that the beneficial effects of vitamin D on fracture risk may be mediated, at least in part, by an effect of vitamin D on cytokine concentration. Clearly there is a need for more studies, both observational and intervention studies, to determine whether vitamin D status favourably modulates bone health through an effect on the immune and inflammatory systems.





{kind=link}