1. Introduction
Schizophrenia is a long-term mental illness associated with considerable mortality and morbidity [
1]. Suicide represents one of the leading causes of premature death in patients affected by schizophrenia and a critical global issue that has a major impact on public health [
2,
3]. For decades, suicide has remained one of the leading causes of preventable death worldwide [
4]. Moreover, patients diagnosed with schizophrenic disorder are a suicide risk group, especially during chronic relapses and the first months following hospital discharge [
5,
6,
7]. Hence, it appears to be imperative to adopt specific measures to reduce suicidal behaviors in patients with schizophrenia and related disorders.
Telemedicine helps increase access to services for at-risk populations and provides opportunities to augment mental health services [
8]. Telehealth has become more interactive, affordable and widely available to healthcare providers in addressing chronic medical conditions [
8]. These telecommunication-based interventions—which include videoconferencing, telephone contacts and internet-based programs [
9,
10]—provide a reliable approach to monitoring the risk of suicide in patients with schizophrenia spectrum disorders [
3].
A growing body of research is emerging on the effectiveness of telehealth interventions in patients admitted to the emergency department (ED) for suicidal behavior. Fleischmann et al. [
11] reported significantly fewer suicide attempts and differences in the number of suicide deaths in patients who received telephone contacts for 18 months in comparison to a control group. Vaiva et al. [
12] reported significantly fewer suicide attempts in participants receiving telephone contact one month after a suicide attempt; however, when subsequent telephone contact intervention three months post-attempt was compared to a control condition, there was no difference in the number of suicide reattempts between the groups. Other studies on tele-assistance with individuals at risk of suicide have found that monitoring interventions, and specifically telephone follow-up programs, provided promising results and could be considered as a new and useful instrument in the care of those at risk [
13,
14,
15,
16,
17]. In addition, these interventions incur a relatively low-cost burden to healthcare budgets and can thus be implemented in regions with limited resources.
While there is clearly a need for innovative strategies to treat people who have attempted suicide, patients with schizophrenia have obtained relatively less attention in this regard. The treatment of schizophrenia comprises psychosocial and pharmacological approaches that are generally only mildly effective [
18]. Access to care limitations among schizophrenia patients may result in non-adherence to treatment. Telehealth communication services may offer one way of enhancing the stability of treatment response. Digital and mobile applications are in their infancy; currently, they have only been tested in a few trials with marginal quality and inconclusive findings [
2].
According to a previous review article [
19], modalities including the telephone, Internet and videoconferencing seem to be feasible for schizophrenia patients. Furthermore, preliminary evidence indicates that such approaches appear to enhance patient outcomes [
19]. Although telephone follow-up offers a promising tool for increasing treatment adherence after discharge from the hospital, its effectiveness in doing so among this population remains unclear [
20].
The present review’s objective was to explore the effectiveness of telephone-delivered, non-pharmacological interventions among patients with schizophrenia and related disorders. To the best of the researchers’ knowledge, no systematic review has been reported that examines telephone-delivered treatments, especially those focused on suicide prevention and the assessment of suicide-specific outcomes, in the schizophrenia patient population.
2. Methods
The systematic review was performed in accordance with the Preferred Reporting Items for Systematic Review and Meta-Analysis (PRISMA) [
21,
22]. We addressed the following research question, constructed according to PICO criteria (Population, Intervention, Comparison and Outcomes) [
23]: In adults (≥17 years of age) with schizophrenic spectrum disorders that report prior suicidal behavior (P), what is the effectiveness of telephone-delivered treatments (I) in suicide prevention (O) compared to a control group (C), at any follow-up period?
The inclusion criteria were: (1) adults (≥17 years of age) with a diagnosis of schizophrenia spectrum disorder; (2) presence of suicidal ideation or prior suicidal behavior; and (3) telephone-based suicide prevention interventions (i.e., telephone call, hotline, or text message). The communication should include some, but not necessarily all, of the following elements: improving compliance with medication and follow-up appointments; addressing any problems, stressors, or risk factors; and reducing suicide re-attempts. No restriction was placed on the duration of the intervention.
The exclusion criteria were: (1) presence of non-suicidal self-harm; (2) no comparison condition; (3) non-original studies (e.g., editorials, guidelines, systematic reviews, meta-analyses, protocol); (4) no full-text available.
Literature searches were performed in the PubMed, PsycInfo, Scopus and Web of Science electronic databases. The search strategy yielded articles that contained combinations of the following key terms: (suicide OR self-harm OR self-injury OR self-destructive behavior) AND (schizophrenia OR “psychotic disorder” OR “psychotic symptom” OR “delusional disorder”) AND (telemedicine OR telepsychiatry OR telepsychology OR telephone OR hotline OR helpline). The search terms were selected in accordance with the Peer Review of Electronic Search Strategies guideline statement (PRESS) [
24]. The drafted electronic search strategy for each database is included in the
Supplementary Materials (
Table S1). The search was conducted on 5 September 2022, limited to English or Spanish language, with no restrictions on the publication period. The review methods were established before the review was performed.
The results of the searches were transferred to Mendeley (version 1.19.8). The duplicate articles were automatically removed by Mendeley and manually by the first reviewer (L.C.). The file was blind-screened by two reviewers (A.I.C. and L.C.) using Rayyan Systems Inc. [
25] based on titles, abstracts and keywords. The references selected were exported to a template developed by the review group and a blinded screening of the full text was performed to check the eligibility of the study. When necessary, a third reviewer (A.S.) was asked to review the selection process and to resolve discrepancies among the reviewers. The article selection process is described in a PRISMA flow diagram [
26].
Two independent authors (A.I.C. and L.C.) extracted data from the selected full-text articles by entering key information from each study into a standardized data extraction template. The general information extracted included the authors, title, research type, date and location of publication, sample size, participant details, intervention and control condition, outcome measures (i.e., instruments and moment of evaluation), feasibility and results.
The risk of bias (RoB) of the selected studies was evaluated employing the Cochrane Collaboration’s Risk of Bias Assessment Tool [
27]. We classified studies as high (considered high risk in at least one domain), some concerns (considered raising some concerns in at least one domain), or low risk of bias (considered low risk in all domains).
3. Results
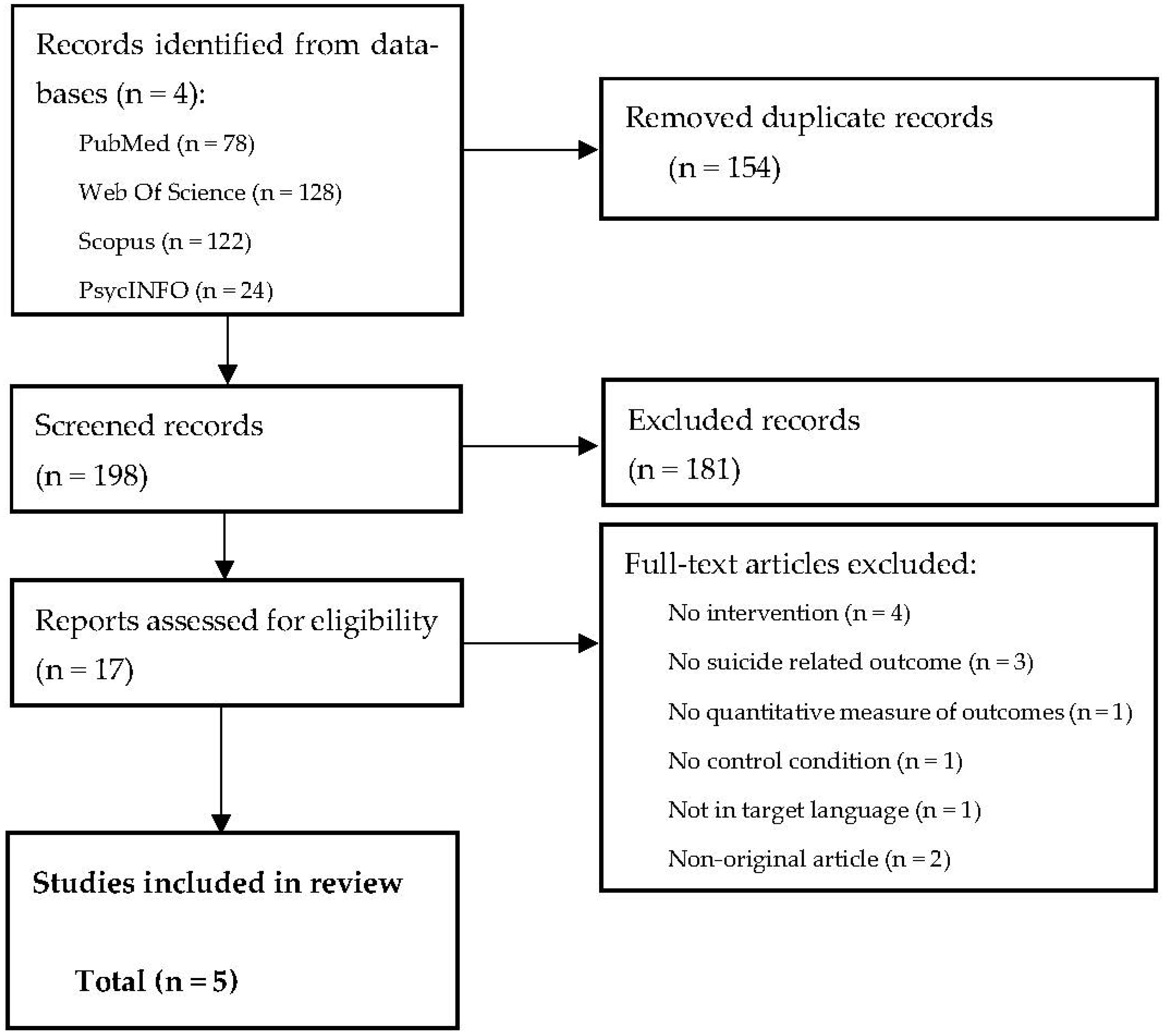
The initial search conducted in the four electronic databases revealed a total of 352 candidate publications. Once duplicates were removed, 198 titles, abstracts and keywords were examined, from which 17 studies were retained for full-text review. We excluded any studies that did not focus on the targeted intervention (n = 84), did not include a diagnosis of schizophrenia or related disorders (n = 30), did not report the presence of suicidal ideation or previous suicidal behavior (n = 22), or were not original studies (n = 45).
A total of 12 studies [
3,
7,
28,
29,
30,
31,
32,
33,
34,
35,
36,
37] were excluded after full-text screening (
Supplementary Materials Table S2). We excluded studies that did not refer to telephone-based interventions (
n = 4) or suicide-related outcomes (
n = 3). Articles were also ineligible if they did not include a quantitative measurement of suicide-related outcomes (
n = 1), a comparison condition (
n = 1), were not written in Spanish or English (
n = 1), or were not original studies (
n = 2). Finally, five articles were included in the review (
Figure 1). Reviewers 1 and 2 resolved the discrepancies detected and the third reviewer was only required to validate the resulting agreement.
Table 1 summarizes the characteristics of the eligible studies. The sample size oscillated between 7 and 120 in the intervention group (IG) and 6 and 117 in the control group (CG). The average age of the participants was 44.3 (SD = 13.96) and 42.48 (SD = 12.93) in IG and CG, respectively. The percentage of men in all studies was over 90%, both in the IG and CG. A total of three studies assessed veterans diagnosed with schizophrenia or schizoaffective disorder admitted to the healthcare system for suicidal behavior, one focused on patients diagnosed with schizophrenia hospitalized for escalation of suicidality and one considered patients with a primary diagnosis of schizophrenia. The included studies were conducted in two countries: the United States of America (USA;
n = 4) and China (
n = 1). All the included study designs are randomized control trials (RCT;
n = 5). Most of the studies used electronic text messages in addition to face-to-face assessment and telephone calls and only one study involved the participation of a non-specialist healthcare assistant and made use of an electronic platform to deliver text messages. Four studies (80%) implemented the intervention in an inpatient unit [
38,
39,
40,
41] and one research work employed a telehealth program in a community setting [
42]. The intervention condition was monitored by nursing professionals (
n = 4; 80%) [
38,
39,
40,
41], a non-specialist healthcare assistant (i.e., patient family member or community volunteer) and family physicians or psychiatrists (
n = 1; 20%) [
42]. All studies (
n = 5) assessed suicidal ideation, 80% (
n = 4) assessed depressive symptoms, 40% (
n = 2) assessed positive and negative symptoms and 20% (
n = 1) assessed treatment adherence. Additionally, four (80%) studies examined the feasibility of the telemonitoring program [
39,
40,
42]. The outcomes were measured with a variety of validated tools (
Table 1).
3.1. Characteristics of Telehealth Interventions
A total of four articles employed a text-message system as the intervention delivery strategy [
38,
39,
40,
41]. Kasckow et al. [
38] evaluated a telemonitoring intervention, called Health Buddy© (HB), in a population of US veterans with a diagnosis of schizophrenic disorder recently discharged for suicidal ideation. The HB provided daily monitoring via text-based questions that assisted with symptom evaluations and staff-patient communication. Daily reports were monitored by inpatients nursing staff twice per 8-h shift over a 24-h period. The Beck Scale for Suicidal Ideation (SSI), the Calgary Depression Rating Scale (CDRS), the Clinical Global Impressions and the Scale for Positive Symptoms were administered from baseline to months 1 and 2.
In addition, Kasckow et al. [
39] aimed to compare VA Usual Care (UC) with UC augmented with a daily HB program in an RCT. All the participants received a visit within two weeks of being discharged by their clinician and were periodically administered medication. Some participants received more intensive treatment, such as the VA’s Psychosocial Residential Rehabilitation Residential Treatment Program (PRRTP), as part of the intervention for veterans with substance use disorders. Assessment was conducted at baseline and follow-up (weeks 2, 4, 8 and 12) through the SSI and the CDRS.
The same research team, Kasckow et al. [
40], investigated whether augmented Intensive Case Monitoring (ICM) with the HB program could produce a significant reduction in suicidal ideation compared to an ICM-only group. The telehealth device connected with participants to ask them questions each day for 10–15 min. The responses were transferred electronically to a secure website and were read by healthcare staff every four hours, seven days a week. The telehealth device targeted the follow-up of symptoms of suicide, depression, psychosis, medication compliance and substance use. The dialogues provided participants with the crisis line phone number in case of escalation in suicidal ideation. To assess the outcomes, the authors used the SSI, the CDRS, the Hamilton Depression Rating Scale (HAMD) and the Positive and Negative Symptoms Scale (PANSS). The study also evaluated the impact of deploying a specialized telehealth case management system employing the HB to reduce suicide among patients with schizophrenia.
More recently, Flaherty et al. [
41] hypothesized that adding telehealth to ICM would decrease the number of veterans with schizophrenia or schizoaffective disorder admitted to hospital for psychiatric care in response to suicidal behavior. The telehealth and ICM groups were compared on (1) baseline measures; (2) the number and total days of medical and psychiatric hospitalization 90 days after treatment and (3) the number of ED visits.
Another study performed by Xu et al. [
42] examined the impact of adding mobile text messaging to enhance schizophrenia care in a community-based, low-resource setting compared with a community-based free medicine program. The participants in the intervention group received the 686 Program, a national treatment program in which psychiatrists travel twice monthly to the healthcare institution to offer patient consultations and no-cost medication, in addition to LEAN (Lay health supporters, E-platform, Award and iNtegration), a program that included the participation of a non-specialist healthcare assistant and medication reminders, healthcare information and follow-up for relapse with text messaging. The intervention often involved designating a member of the family to supervise the patient’s medication, adverse effects, risk of relapse and requirement for emergency care. While the primary outcomes were treatment adherence, other variables were also measured, including patient symptoms, re-hospitalization and suicide.
Overall, the studies addressing risk management focused on a telehealth monitoring protocol [
38,
39,
40,
41]. When participants reported suicidal plans or intent, the nurse contacted a physician, which provided a prompt response. In addition, staff immediately contacted participants when they answered affirmatively to a question about suicidal behavior. If this occurred, healthcare members assessed the situation and determined whether: (1) the participant needed no action; (2) the participant required a consultation with their clinician; or (3) the participant needed to attend the emergency room (ER).
Furthermore, the dialogues assisted patients in determining when to contact their physician in the event of worsening psychotic or depressive symptoms. Patients were also encouraged to adopt recovery-centered behavior, for example, by turning to reliable people in the event of distress. If participants did not upload responses within 24 h, personnel contacted them to confirm their safety and encourage them to continue using the device. The dialogues used were provided by employing patient-centered design methods developed through a panel of consumers and academic experts in suicidality and schizophrenia.
3.2. Effectiveness of Telephone-Delivered Interventions for Patients with Diagnosis of Schizophrenia Spectrum Disorders on Suicide Prevention
The telehealth follow-up interventions for suicidal behavior were effective in reducing endpoint suicidal ideation scores compared with baseline in individuals with schizophrenia spectrum disorders relative to a controlled condition [
38,
39,
40].
Kasckow et al. [
38] presented results showing a reduction in suicide ideation (
p = 0.04) along with positive symptoms (
p = 0.02) in HB patients relative to CG. The preliminary results illustrate that patients reported relatively elevated levels of adherence to HB system; furthermore, telehealth monitoring was associated with earlier remission of suicidal ideation among schizophrenia patients discharged from hospital for suicide treatment.
Consistent with these findings, Kasckow et al. [
39] reported significant improvements in SSI scores in HB participants. Overall improvement was shown by both groups in the first 4 weeks. However, mean SSI scores of the HB group patients decreased as time progressed, while for CG patients, these scores decreased initially and then increased after 4 weeks. A significant interaction between time and intervention (F(1, 68) = 5.2;
p < 0.05) suggests that the HB condition showed a greater enhancement in SSI scores than the CG condition during the 12-week study period. Mean CDRS scores for participants in HB and CG decreased initially and increased over time. No differences were found between HB and CG in depressive symptoms.
Kasckow et al. [
40] reported that there were reductions in SSI scores at endpoint compared to baseline in both IG and CG. The SSI scores of the HB group were decreased from 9.8 (SD = 6.15) at baseline to 2.44 (SD = 5.52) at endpoint, while the CG score was decreased from 10.7 (SD = 8.24) at baseline to 2.88 (SD = 6.71) at endpoint. There were no group differences with survival analysis using remission (i.e., SSI score = 0) as the outcome. Nevertheless, for a subgroup with a history of attempted suicide, there was a tendency toward a greater remission at 3 months for those in the HB group (16/18) compared with the CG group (14/19; log rank = 2.82;
df = 1;
p = 0.09).
In the study by Flaherty et al. [
41], comparisons of treatment conditions disclosed significant differences in hospitalizations. Patients in the telehealth arm had a significantly lower probability than patients in the CG arm of suffering at least one hospitalization (5.0% vs. 32.0%;
p < 0.05). Moreover, the telehealth condition showed a significantly lower mean number of medical readmissions (0.10 ± 0.45 vs. 0.60 ± 1.19, Mann–Whitney’s U = 4.67;
df = 1;
p < 0.05) and number of days of hospitalization (0.70 ± 3.13 vs. 2.56 ± 6.11, Mann–Whitney’s U = 4.59;
df = 1;
p < 0.05). No significant group differences were reported in terms of numbers of psychiatric hospitalizations (0.65 ± 1.04 vs. 0.52 ± 0.77) and ED visits (0.60 ± 1.23 vs. 0.92 ± 1.19).
In a community-based study, Xu et al. [
42] observed a decline in the risk of relapse (26/120 (21.7%) IG participants vs. 40/117 (34.2%) CG participants; relative risk 0.63 (95% CI 0.42 to 0.97)) and re-hospitalization (9/123 (7.3%) IG participants vs. 25/122 (20.5%) CG participants; relative risk 0.36 (95% CI 0.17 to 0.73)). The program yielded no statistical difference in the other outcomes evaluated, including suicide.
3.3. Feasibility
The studies reported that telehealth implementation for the study population appears to be feasible, with adherence and participant evaluation of the intervention as indicators of applicability [
39,
40]. The application in rural areas, where hospitals did not have specialized services, was also acceptable [
42]. Kasckow et al. [
38] presented preliminary results revealing relatively favorable adherence to HB use, ranging from 87–100% in the first month to 78–100% in the second month.
Kasckow et al. [
39] concluded that telehealth monitoring for patients with schizophrenia discharged from ED for recent suicidal ideation and/or suicide attempt appears to be feasible. The adherence rates for daily use of the HB program were as follows: month
1 = 86.9% (
n = 14); month
2 = 86.3% (
n = 12); and month
3 = 84.1% (
n = 11).
More recently, Kasckow et al. [
40] reported monthly adherence for telehealth participants of >80%. Specifically, the monthly adherence rates were as follows: month
1 = 83% (
n = 20); month
2 = 92% (
n = 19); and month
3 = 89% (
n = 15). Post-hoc review of the face-to-face interviews data disclosed that associated factors with mild adherence included: the accentuation of depression (
n = 2), technical issues (
n = 4), or distressing home environment (
n = 2). In addition, 14 of the IG patients answered open-ended questions designed to evaluate the telehealth intervention. For individuals with negative reports, concerns about telehealth monitoring centered on the perceived limitations of the program in treating symptoms, along with its non-personal nature. Concerning positive statements, participants described the intervention as effective in decreasing their suicidal thoughts, improving adherence to medication and reducing anxiety and depressive symptoms.
Along similar lines, Xu et al. [
42] reported that the intervention program was generally well-accepted by participants and their family members, while also achieving a good level of participant satisfaction, reporting only 4.3% attrition in comparison to an overall rate of 20% (95% CI 17% to 24%) in other schizophrenia intervention trials [
42].
In addition, individual studies pointed out the need to facilitate guidance about how the device was to be used [
40,
42]. This entailed standard procedures to ensure that participants could use basic phone functions, were able to read/return text messages and understood how information was sent to healthcare professionals.
3.4. Strengths and Limitations
Four of the five studies [
38,
39,
40,
41] reported that approximately 20% of IG participants never initiated the intervention for the following reasons: technological problems (i.e., lack of mobile device or phone company debt), cognitive difficulties, transportation issues and relapse to substance use.
Focusing on the analysis of the qualitative data, negative reports suggested that patients sometimes experienced frustration when communicating with a machine rather than a human [
40]. Despite these negative statements, evaluation of the qualitative data revealed that most of the patients gave positive responses. These favorable statements indicated that the program assisted in instilling hope and that it was useful and easy to use [
40].
A further benefit of telehealth monitoring is increased access to care. Enhancing the patient–provider connection via telehealth could improve adherence to treatment. The use of daily monitoring text messages represents another telehealth system approach in the telephone-based intervention spectrum. Individuals with schizophrenia are known to have elevated rates of cognitive impairments and thus a simple and easy-to-use device, as presented in the included studies, could be most appropriate for telemonitoring in this population [
39,
43,
44]. The technology presented allows for ease and efficiency of communication between patients and clinical staff. Therefore, the implementation of a clinical telehealth system shows promise in efforts to address suicide risk among patients at increased risk of recidivism.
Consistent with these findings, Xu et al. [
42] reported that the program was found to be reasonably easy to implement and use, incurring only marginal additional costs to patients and their families. The study emphasized the need for adequate training of patients on how to receive, read and respond to text messages, since despite the instructions provided, 28.8% of the participants were still unable to read the messages at the endpoint. To overcome this concern, the researchers delivered voice messages to some participants and, at the same time, sent text messages to the nonprofessional healthcare collaborators. Their experiences warn against the use of smartphones or more complicated applications among individuals with a diagnosis of schizophrenia and a low educational level. Finally, the potential adverse impacts of text messaging on participants and their families deserves further investigation, since 4 (6.3%) patients and 10 (10.7%) non-specialist healthcare assistants indicated that text messaging was bothersome.
3.5. Quality of the Studies
Table 2 shows the RoB for each included study. All the studies were randomized trials with a control group, corresponding to the usual mental healthcare provided at the research site (e.g., ICM, 686 Program, or UC plus PRRTP). A methodological concern is that studies relied on convenience samples. Selection bias (i.e., selection of the most compliant participants only) was probably high and compliance rates may have been altered because patients were disposed to consent to the trial, which could have compromised external validity. Therefore, interpretations must be made with care, as the results may not be generalizable to other conditions (i.e., other populations).
4. Discussion
The present review is, to our knowledge, the first to summarize studies employing telephone-based interventions for suicide prevention in individuals with schizophrenia. The results of the review suggest that augmenting telehealth is associated with decreased numbers and durations of hospitalizations, appears to be feasible and is associated with the remission of suicidal thoughts among patients with schizophrenia admitted to the hospital for suicide treatment [
38,
39,
40,
41]. In rural and resource-poor communities, the delivery of text messages effectively dealt with low compliance rates at marginal cost [
30,
42]. The interventions were found to be mostly well-accepted by participants and their relatives and were reasonably simple to administer and use. These results could have consequences for the future formulation of clinical policies for the prevention of repeated suicidal behaviors in patients diagnosed with schizophrenia.
A limited number of studies examining the use of telehealth technologies for suicide prevention in patients with schizophrenia or schizoaffective disorder are available. Preliminary research exploring telephone-based modalities have demonstrated that this method appears to be achievable. Furthermore, these preliminary investigations have reported that telehealth monitoring seems to improve outcomes, particularly concerning suicidal ideation, positive symptoms of schizophrenia, treatment adherence, ER visits and medical hospitalization rates [
38,
39,
40,
41,
42]. Moreover, telephone-based interventions appear to be well-accepted by patients and families [
42].
Significant heterogeneity was observed between the included studies, such as year of publication and differences in sample size, in addition to a limited range of languages and nationalities. The article by Kasckow et al. [
38] was published in 2009; therefore, it might have a different perspective on telemedicine than the other studies, which were all conducted after 2015. However, the telemedicine program used in the latter studies (Health Buddy©) was comparable.
In addition, the role of the risk of bias assessment in the interpretation of the results should be emphasized. There were several areas of high potential for bias across these studies. The potential for detection bias was high for three studies (60%) [
38,
39,
40], where research staff performing the assessments were not masked. One study (20%) [
40] was also judged at high potential for selective reporting bias, largely due to the lack of prior registration of the trial protocol. In summary, the research appears to be at a preliminary stage and improvements in design, sample size and preregistration would be beneficial.
While multiple systematic reviews have been published previously, the participants were not restricted to patients showing suicidal behavior. For example, Kasckow et al. [
19] were optimistic about the role of telepsychiatry for the monitoring of patients with schizophrenia. In addition, preliminary evidence suggests that these modalities appear to be feasible and improve patient outcomes, although additional research should focus on further developing interventions and replicating promising results. Gire et al. [
45] also conducted a systematic review to evaluate research on mHealth interventions for psychosis. The results hold potential promise for reducing the global gap in mental health treatment by enabling individuals into treatment via their cell phones, particularly those living in remote or rural areas and for those from resource-poor environments. Bright [
20] carried out another systematic review of telephone-based interventions in individuals with severe mental illness and concluded that cell phone contact is a potentially beneficial tool for improving medication adherence post-discharge, although their efficacy remains unclear.
While our findings are consistent with previous results, the present report also provides a new perspective that examines telephone interventions implemented in patients with schizophrenia and prior suicidal behaviors. Recently, a pilot trial has been published that evaluated a suicide prevention protocol tailored to patients with psychotic disorders [
37]. Shirvastava et al. [
7] conducted a community-based study on a crisis helpline targeted at suicide prevention. They reported that the existence of crisis helplines can significantly reduce the delay in treatment and facilitate early and easy access to diagnosis and treatment. Kasckow et al. [
35], in a qualitative analysis of the construction of telehealth conversations for the monitoring of suicidal patients with schizophrenia, identified four main issues to be considered when delivering text messages: (1) some themes elicited a high emotional response; (2) there were confidentiality concerns; (3) certain messages were too generalized; and (4) some vocabulary and wording were problematic.
The implementation of a clinical telehealth program offers promise for efforts aimed at addressing suicide risk. The present review adds to the evidence supporting the notion that follow-up is an important element in the management of the disease. Preliminary results indicate that the deployment of the telehealth program is feasible in the follow-up of suicide risk after discharge in patients diagnosed with schizophrenia or schizoaffective disorder. This is relevant for a population that is deemed to be at risk for noncompliance with appointments [
46]. Strengthening patient–provider connections through telehealth could increase treatment adherence, help improve access to services for at-risk populations in remote areas and provide opportunities for improving mental health services.
4.1. Limitations
Our review has several limitations. A major limitation of the article is the lack of external validity, since the results and conclusions can only be valid in contexts similar to those of the studied research. We identified a limited number of studies conducted to date. In addition, most studies used a small and therefore underpowered sample size, often selecting veterans from a single urban location in the eastern U.S. [
38,
39,
40,
41]. The intensive nature of the CG (i.e., two calls and one face-to-face visit from the nurse per week) may have resulted in a marked treatment effect in patients assigned to the control group, which may have obscured any potential improvement from using telehealth as an adjunctive treatment. Moreover, the pursuit of simplicity reduced the capacity to personalize the content, frequency and duration of the messages to patients. While individual adjustment is perceived to be more effective [
47], it could also have considerably expanded the complexity and cost of the program. It should be noted that the elevated compliance rates could have been due to selection bias since participants were prepared to consent to the trial, an issue that could have affected external validity [
40].
4.2. Implication for Research
Evidence for the effectiveness of telephone-based interventions for suicide prevention in patients with schizophrenia spectrum disorders is limited. More RCTs based on clinically representative samples are required, not only to assess compliance, but also to demonstrate maintenance of clinical benefits for participants with schizophrenia, particularly the prevention of suicide reattempts. The selected studies highlighted the need for further research to replicate and amplify the findings, especially considering that the current research used small sample sizes. In addition, the control condition consisted of a considerably more intensive level of intervention than usually offered in outpatient mental health services. The latter is a common problem with studies involving suicidal patients, i.e., achieving the right balance between maintaining sufficient scientific rigor versus keeping high standards of ethics to maximize safety in a high-risk population [
40,
48]. Determining the adequate CG will be critical in future studies involving telehealth and suicide-risk populations. Further research should also examine the influence of outcomes other than psychopathological measures in facilitating adherence to pharmacological and non-pharmacological treatment.
5. Conclusions
Telehealth follow-up for individuals with schizophrenia and suicidal behavior appears to be feasible. The preliminary findings suggest that, in patients with schizophrenia and related disorders, telehealth monitoring drives a larger decrease in suicidal ideation, but not in depressive symptoms, compared to TAU. For the outcome of suicidal deaths, no results were reported to support the presence of a beneficial effect of the intervention since the number of suicide deaths was very low, even in the high-risk ED population. Furthermore, the treatment has not been proven to have a long-term effect. More research is required to expand our knowledge regarding the ways in which telehealth can be used effectively to enhance care for patients with schizophrenic disorders.
The development of telehealth interventions for people with suicidal behavior and schizophrenic disorders is still under construction. The current data provide early indications of the effectiveness of non-pharmacological interventions targeting emotions and cognitive symptoms. Telephone text messaging has proven helpful for strengthening community and family care given its availability, reliability and usability [
42]. The telehealth monitoring system further enhanced UC by addressing poor adherence rates at marginal cost. Nevertheless, there is no clear evidence to suggest that texting improves certain clinical symptoms, medication adherence and functioning in patients with schizophrenia [
42].
Author Contributions
Conceptualization, A.I.C. and L.C.; methodology, A.I.C., L.C. and A.S.; software, L.C.; validation, A.I.C.; formal analysis, A.I.C. and L.C.; investigation, A.I.C., L.C. and A.S.; resources, L.C.; data curation, L.C.; writing—original draft preparation, L.C.; writing—review and editing, A.I.C., A.S., V.P. and D.P.; visualization, L.C.; supervision, A.I.C.; project administration, D.P.; funding acquisition, A.I.C. and V.P. All authors have read and agreed to the published version of the manuscript.
Funding
This research was funded by Instituto de Salud Carlos III, Subdirección General de Evaluación y Fomento de la Investigación (ISCIII) and Fondo Europeo de Desarrollo Regional (FEDER), grant number PI19/01484—Prevención e Intervención en Suicidio (SURVIVE): Estudio de cohorte y ensayos clínicos controlados anidados de programas de prevención secundaria para intentos de suicidio—Fundación Parc Taulí. The APC was funded by Instituto de Salud Carlos III, Subdirección General de Evaluación y Fomento de la Investigación (ISCIII) and Fondo Europeo de Desarrollo Regional (FEDER). D.P thanks the support of Spanish Ministry of Science and Innovation/ISCIII/FEDER (PI21/01148); the Secretaria d’Universitats i Recerca del Departament d’Economia i Coneixement of the Generalitat de Catalunya (2021 SGR 01431); the CERCA program of the I3PT; the Instituto de Salud Carlos III; and the CIBER of Mental Health (CIBERSAM).
Institutional Review Board Statement
Not applicable.
Informed Consent Statement
Not applicable.
Data Availability Statement
The data presented in this review are available upon request from the corresponding author.
Conflicts of Interest
D.P. has received grants and also served as consultant or advisor for Rovi, Angelini, Janssen, Lundbeck and Servier. The other authors declare no conflict of interest. The funders had no role in the design of the study; in the collection, analyses, or interpretation of data; in the writing of the manuscript; or in the decision to publish the results.
References
- Hodo, D.W. Kaplan and Sadock’s comprehensive textbook of psychiatry. Am. J. Psychiatry 2006, 163, 1458. [Google Scholar] [CrossRef]
- Curto, M.; Fazio, F.; Ulivieri, M.; Navari, S.; Lionetto, L.; Baldessarini, R.J. Improving adherence to pharmacological treatment for schizophrenia: A systematic assessment. Expert Opin. Pharmacother. 2021, 22, 1143–1155. [Google Scholar] [CrossRef] [PubMed]
- Kasckow, J.; Gurklis, J.; Haas, G. A telehealth intervention for suicidal patients with schizophrenia. Schizophr. Bull. 2011, 37, 308–330. [Google Scholar]
- World Health Organization. Suicide Worldwide in 2019. Available online: https://www.who.int/publications-detail-redirect/9789240026643 (accessed on 1 October 2022).
- Olfson, M.; Wall, M.; Wang, S.; Crystal, S.; Gerhard, T.; Blanco, C. Suicide following deliberate self-harm. Am. J. Psychiatry 2017, 174, 765–774. [Google Scholar] [CrossRef]
- Shand, F.; Vogl, L.; Robinson, J. Improving patient care after a suicide attempt. Australas. Psychiatry 2018, 26, 145–148. [Google Scholar] [CrossRef]
- Shrivastava, A.K.; Johnston, M.E.; Stitt, L.; Thakar, M.; Sakel, G.; Iyer, S.; Shah, N.; Bureau, Y. Reducing treatment delay for early intervention: Evaluation of a community based crisis helpline. Ann. Gen. Psychiatry 2012, 11, 20. [Google Scholar] [CrossRef]
- Lin, T.; Stone, S.J.; Heckman, T.G.; Anderson, T. Zoom-in to zone-out: Therapists report less therapeutic skill in telepsychology versus face-to-face therapy during the COVID-19 pandemic. Psychotherapy 2021, 58, 449. [Google Scholar] [CrossRef]
- Inagaki, M.; Kawashima, Y.; Kawanishi, C.; Yonemoto, N.; Sugimoto, T.; Furuno, T.; Ikeshita, K.; Eto, N.; Tachikawa, H.; Shiraishi, Y.; et al. Interventions to prevent repeat suicidal behavior in patients admitted to an emergency department for a suicide attempt: A meta-analysis. J. Affect. Disord. 2015, 175, 66–78. [Google Scholar] [CrossRef]
- Zalsman, G.; Hawton, K.; Wasserman, D.; van Heeringen, K.; Arensman, E.; Sarchiapone, M.; Carli, V.; Höschl, C.; Barzilay, R.; Balazs, J.; et al. Suicide prevention strategies revisited: 10-year systematic review. Lancet Psychiatry 2016, 3, 646–659. [Google Scholar] [CrossRef]
- Fleischmann, A.; Bertolote, J.M.; Wasserman, D.; De Leo, D.; Bolhari, J.; Botega, N.J.; De Silva, D.; Phillips, M.; Vijayakumar, L.; Värnik, A.; et al. Effectiveness of brief intervention and contact for suicide attempters: A randomized controlled trial in five countries. Bull. World Health Organ. 2008, 86, 703–709. [Google Scholar] [CrossRef]
- Vaiva, G.; Ducrocq, F.; Meyer, P.; Mathieu, D.; Philippe, A.; Libersa, C.; Goudemand, M. Effect of telephone contact on further suicide attempts in patients discharged from an emergency department: Randomised controlled study. BMJ 2006, 332, 1241–1245. [Google Scholar] [CrossRef] [Green Version]
- Cebrià, A.I.; Parra, I.; Pàmias, M.; Escayola, A.; García-Parés, G.; Puntí, J.; Laredo, A.; Vallès, V.; Cavero, M.; Oliva, J.C.; et al. Effectiveness of a telephone management programme for patients discharged from an emergency department after a suicide attempt: Controlled study in a Spanish population. J. Affect. Disord. 2013, 147, 269–276. [Google Scholar] [CrossRef]
- Comtois, K.A.; Kerbrat, A.H.; DeCou, C.R.; Atkins, D.C.; Majeres, J.J.; Baker, J.C.; Ries, R.K. Effect of Augmenting Standard Care for Military Personnel With Brief Caring Text Messages for Suicide Prevention: A Randomized Clinical Trial. JAMA Psychiatry 2019, 76, 474–483. [Google Scholar] [CrossRef]
- Exbrayat, S.; Coudrot, C.; Gourdon, X.; Gay, A.; Sevos, J.; Pellet, J.; Trombert-Paviot, B.; Massoubre, C. Effect of telephone follow-up on repeated suicide attempt in patients discharged from an emergency psychiatry department: A controlled study. BMC Psychiatry 2017, 17, 96. [Google Scholar] [CrossRef]
- Mousavi, S.; Zohreh, R.; Sharbafchi, M.; Ebrahimi, A.; Maracy, M. The efficacy of telephonic follow up in prevention of suicidal reattempt in patients with suicide attempt history. Adv. Biomed. Res. 2014, 3, 198. [Google Scholar] [CrossRef] [PubMed]
- Plancke, L.; Amariei, A.; Danel, T.; Debien, C.; Duhem, S.; Notredame, C.E.; Wathelet, M.; Vaiva, G. Effectiveness of a French Program to Prevent Suicide Reattempt (VigilanS). Arch. Suicide Res. 2021, 25, 570–581. [Google Scholar] [CrossRef]
- Patel, K.R.; Cherian, J.; Gohil, K.; Atkinson, D. Schizophrenia: Overview and treatment options. Pharm. Ther. 2014, 39, 638–645. [Google Scholar]
- Kasckow, J.; Felmet, K.; Appelt, C.; Thompson, R.; Rotondi, A.; Haas, G. Telepsychiatry in the assessment and treatment of schizophrenia. Clin. Schizophr. Relat. Psychoses 2014, 8, 21–27A. [Google Scholar] [CrossRef]
- Bright, C.E. Integrative Review of Mobile Phone Contacts and Medication Adherence in Severe Mental Illness. J. Am. Psychiatr. Nurses Assoc. 2018, 24, 209–222. [Google Scholar] [CrossRef]
- Moher, D.; Shamseer, L.; Clarke, M.; Ghersi, D.; Liberati, A.; Petticrew, M.; Shekelle, P.; Stewart, L.A. Preferred reporting items for systematic review and meta-analysis protocols (PRISMA-P) 2015 statement. Syst. Rev. 2015, 4, 1. [Google Scholar] [CrossRef]
- Shamseer, L.; Moher, D.; Clarke, M.; Ghersi, D.; Liberati, A.; Petticrew, M.; Shekelle, P.; Stewart, L.A. Preferred reporting items for systematic review and meta-analysis protocols (PRISMA-P) 2015: Elaboration and explanation. BMJ 2015, 349, g7647. [Google Scholar] [CrossRef] [PubMed]
- Saimbert, M. Developing clinical questions for a systematic review. In Comprehensive Systematic Review for Advanced Practice Nursing, 3rd ed.; Holly, C., Salmond, S., Saimbert, M., Eds.; Springer: New York, NY, USA, 2021; pp. 85–101. [Google Scholar]
- McGowan, J.; Sampson, M.; Salzwedel, D.M.; Cogo, E.; Foerster, V.; Lefebvre, C. PRESS Peer Review of Electronic Search Strategies: 2015 Guideline Statement. J. Clin. Epidemiol. 2016, 75, 40–46. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ouzzani, M.; Hammady, H.; Fedorowicz, Z.; Elmagarmid, A. Rayyan—A web and mobile app for systematic reviews. Syst. Rev. 2016, 5, 210. [Google Scholar] [CrossRef]
- Moher, D.; Liberati, A.; Tetzlaff, J.; Altman, D.G. Preferred reporting items for systematic reviews and meta-analyses: The PRISMA statement. Int. J. Surg. 2010, 8, 336–341. [Google Scholar] [CrossRef]
- Sterne, A.C.; Savović, J.; Page, M.J.; Elbers, R.G.; Blencowe, N.S.; Boutron, I.; Cates, C.J.; Cheng, H.Y.; Corbett, M.S.; Eldridge, S.M.; et al. RoB 2: A revised tool for assessing risk of bias in randomised trials. BMJ 2019, 366, l4898. [Google Scholar] [CrossRef]
- Palmier-Claus, J.E.; Ainsworth, J.; Machin, M.; Dunn, G.; Barkus, E.; Barrowclough, C.; Rogers, A.; Lewis, S.W. Affective instability prior to and after thoughts about self-injury in individuals with and at-risk of psychosis: A mobile phone based study. Arch. Suicide Res. 2013, 17, 275–287. [Google Scholar] [CrossRef]
- Henson, P.; Torous, J. Feasibility and correlations of smartphone meta-data toward dynamic understanding of depression and suicide risk in schizophrenia. Int. J. Methods Psychiatr. Res. 2020, 29, e1825. [Google Scholar] [CrossRef]
- Cai, Y.; Gong, W.; He, H.; Hughes, J.P.; Simoni, J.; Xiao, S.; Gloyd, S.; Lin, M.; Deng, X.; Liang, Z.; et al. Mobile Texting and Lay Health Supporters to Improve Schizophrenia Care in a Resource-Poor Community in Rural China (LEAN Trial): Randomized Controlled Trial Extended Implementation. J. Med. Internet Res. 2020, 22, e22631. [Google Scholar] [CrossRef]
- Palmier-Claus, J.E.; Taylor, P.J.; Ainsworth, J.; Machin, M.; Dunn, G.; Lewis, S.W. The temporal association between self-injurious thoughts and psychotic symptoms: A mobile phone assessment study. Suicide Life Threat. Behav. 2014, 44, 101–110. [Google Scholar] [CrossRef]
- Arevian, A.C.; Bone, D.; Malandrakis, N.; Martinez, V.R.; Wells, K.B.; Miklowitz, D.J.; Narayanan, S. Clinical state tracking in serious mental illness through computational analysis of speech. PLoS ONE 2020, 15, e0225695. [Google Scholar] [CrossRef]
- Dausch, B.M.; Miklowitz, D.J.; Nagamoto, H.T.; Adler, L.E.; Shore, J.H. Family-focused therapy via videoconferencing. J. Telemed. Telecare 2009, 15, 211–214. [Google Scholar] [CrossRef] [PubMed]
- Smelror, R.E.; Bless, J.J.; Hugdahl, K.; Agartz, I. Feasibility and Acceptability of Using a Mobile Phone App for Characterizing Auditory Verbal Hallucinations in Adolescents With Early-Onset Psychosis: Exploratory Study. JMIR Form. Res. 2019, 3, e13882. [Google Scholar] [CrossRef] [PubMed]
- Kasckow, J.; Zickmund, S.; Rotondi, A.; Mrkva, A.; Gurklis, J.; Chinman, M.; Fox, L.; Loganathan, M.; Hanusa, B.; Haas, G. Development of telehealth dialogues for monitoring suicidal patients with schizophrenia: Consumer feedback. Community Ment. Health J. 2014, 50, 339–342. [Google Scholar] [CrossRef] [PubMed]
- Böcker, F.M. Soziale Integration und Kontakte zu Bezugspersonen des gewohnten sozialen Umfeldes während stationärer Behandlung im psychiatrischen Krankenhaus. Eine prospektive katamnestische Untersuchung an erstmals aufgenommenen Patienten mit schizophrenen und cyclothymen Psychosen. Eur. Arch. Psychiatry Neurol. Sci. 1984, 234, 250–257. [Google Scholar] [CrossRef] [PubMed]
- Depp, C.; Ehret, B.; Villa, J.; Perivoliotis, D.; Granholm, E.A. Brief Mobile-Augmented Suicide Prevention Intervention for People With Psychotic Disorders in Transition From Acute to Ongoing Care: Protocol for a Pilot Trial. JMIR Res. Protoc. 2021, 10, e14378. [Google Scholar] [CrossRef]
- Kasckow, J.; Gurklis, J.; Thompson, R.; Crofutt, R.; Murray, T.; Richmond, I.; Haas, G.A. Telehealth intervention for suicidal patients with schizophrenia. Schizophr. Bull. 2009, 35, 374. [Google Scholar]
- Kasckow, J.; Gao, S.; Hanusa, B.; Rotondi, A.; Chinman, M.; Zickmund, S.; Gurklis, J.; Fox, L.; Cornelius, J.; Richmond, I.; et al. Telehealth Monitoring of Patients with Schizophrenia and Suicidal Ideation. Suicide Life Threat. Behav. 2015, 45, 600–611. [Google Scholar] [CrossRef]
- Kasckow, J.; Zickmund, S.; Gurklis, J.; Luther, J.; Fox, L.; Taylor, M.; Richmond, I.; Haas, G.L. Using telehealth to augment an intensive case monitoring program in veterans with schizophrenia and suicidal ideation: A pilot trial. Psychiatry Res. 2016, 239, 111–116. [Google Scholar] [CrossRef]
- Flaherty, L.R.; Daniels, K.; Luther, J.; Haas, G.L.; Kasckow, J. Reduction of medical hospitalizations in veterans with schizophrenia using home telehealth. Psychiatry Res. 2017, 255, 153–155. [Google Scholar] [CrossRef]
- Xu, D.; Xiao, S.; He, H.; Caine, E.D.; Gloyd, S.; Simoni, J.; Hughes, J.P.; Nie, J.; Lin, M.; He, W.; et al. Lay health supporters aided by mobile text messaging to improve adherence, symptoms, and functioning among people with schizophrenia in a resource-poor community in rural China (LEAN): A randomized controlled trial. PLoS Med. 2019, 16, e1002785. [Google Scholar] [CrossRef]
- Priebe, S.; Kelley, L.; Omer, S.; Golden, E.; Walsh, S.; Khanom, H.; Kingdon, D.; Rutterford, C.; McCrone, P.; McCabe, R. The Effectiveness of a Patient-Centred Assessment with a Solution-Focused Approach (DIALOG+) for Patients with Psychosis: A Pragmatic Cluster-Randomised Controlled Trial in Community Care. Psychother. Psychosom. 2015, 84, 304–313. [Google Scholar] [CrossRef]
- Rotondi, A.J.; Eack, S.M.; Hanusa, B.H.; Spring, M.B.; Haas, G.L. Critical design elements of e-health applications for users with severe mental illness: Singular focus, simple architecture, prominent contents, explicit navigation, and inclusive hyperlinks. Schizophr. Bull. 2015, 41, 440–448. [Google Scholar] [CrossRef]
- Gire, N.; Farooq, S.; Naeem, F.; Duxbury, J.; McKeown, M.; Kundi, P.S.; Chaudhry, I.B.; Husain, N. mHealth based interventions for the assessment and treatment of psychotic disorders: A systematic review. Mhealth 2017, 14, 33. [Google Scholar] [CrossRef] [Green Version]
- Daniels, K.; Loganathan, M.; Wilson, R.; Kasckow, J. Appointment attendance in patients with schizophrenia. Clin. Pract. 2014, 11, 467–482. [Google Scholar] [CrossRef]
- Berrouiguet, S.; Baca-García, E.; Brandt, S.; Walter, M.; Courtet, P. Fundamentals for Future Mobile-Health (mHealth): A Systematic Review of Mobile Phone and Web-Based Text Messaging in Mental Health. J. Med. Internet Res. 2016, 18, e135. [Google Scholar] [CrossRef]
- Charles, F.R.; Howard, D.; Parker, L.S.; Schulberg, H.C.; Mulsant, B.H.; Post, E.; Rollman, B. Treatment as usual (TAU) control practices in the PROSPECT Study: Managing the interaction and tension between research design and ethics. Int. J. Geriatr. Psychiatry 2001, 16, 602–608. [Google Scholar] [CrossRef]
| Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).


 ,
, 



{kind=link}