
Abstract
Background
The relevance of the American College of Surgeons Oncology Group (ACOSOG) Z0011 trial in patients with high-risk breast cancer has been questioned. We hypothesize that Z0011 applies to women with HER2-positive disease (HER2+), triple-negative breast cancer (TNBC), and/or age <50 years at diagnosis (YA).
Methods
Women with node-positive HER2+, TNBC, or YA were identified from a prospectively maintained database. Patients were grouped based on Z0011 trial eligibility criteria into those meeting criteria (eligible) and those who did not (ineligible). Patient and tumor characteristics were compared; survival of those meeting Z0011 criteria was determined.
Results
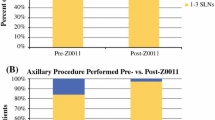
We identified 186 node-positive women undergoing lumpectomy/radiation for high-risk breast cancer: 57 of 186 (31 %) HER2+, 55 of 186 (30 %) TNBC, 74 of 186 (40 %) YA. Overall, 125 of 186 (67 %) met Z0011 criteria. HER2-positivity was associated with the lowest rate of ineligibility compared with TNBC and YA (16 vs. 53 and 31 %, respectively, p < 0.01). Larger tumor size, high grade, extranodal extension, and high Ki67 were associated with Z0011 ineligibility. Among those who were eligible, 105 of 125 (84 %) had ALND and 48 of 125 (38 %) had involvement of nonsentinel nodes (NSLN); median number of NSLNs involved was one (range 1–3). With median follow-up of 5.5 years, there was no difference in survival between those who had ALND and those who did not. After patients with clinically palpable nodes were excluded, 125 of 149 (84 %) met criteria.
Conclusions
The Z0011 trial eligibility requirements apply to a significant proportion of patients with HER2+, TNBC, and YA. ALND can be avoided in 67 % node-positive cases and in 84 % of those with clinically negative nodes.
Similar content being viewed by others


References
Giuliano AE, McCall L, Beitsch P, et al. Locoregional recurrence after sentinel lymph node dissection with or without axillary dissection in patients with sentinel lymph node metastases: the American College of Surgeons Oncology Group Z0011 randomized trial. Ann Surg. 2010;252:426–32; discussion 432–3.
Giuliano AE, Hunt KK, Ballman KV, et al. Axillary dissection vs no axillary dissection in women with invasive breast cancer and sentinel node metastasis: a randomized clinical trial. JAMA. 2011;305:569–75.
Lyman GH, Temin S, Edge SB, et al. Sentinel lymph node biopsy for patients with early-stage breast cancer: American Society of Clinical Oncology Clinical Practice Guideline Update. J Clin Oncol. 2014;32(13):1365–85.
Network NCC. Practice guidelines in oncology: breast, version 1.2012. Fort Washington: NCCN 2012.
Giuliano AE, Morrow M, Duggal S, Julian TB. Should ACOSOG Z0011 change practice with respect to axillary lymph node dissection for a positive sentinel lymph node biopsy in breast cancer? Clin Exp Metastasis. 2012;29:687–92.
Shah-Khan M, Boughey JC. Evolution of axillary nodal staging in breast cancer: clinical implications of the ACOSOG Z0011 trial. Cancer Control. 2012;19:267–76.
Guth U, Myrick ME, Viehl CT, et al. The post ACOSOG Z0011 era: does our new understanding of breast cancer really change clinical practice? Eur J Surg Oncol. 2012;38:645–50.
Gatzemeier W, Mann GB. Which sentinel lymph-node (SLN) positive breast cancer patient needs an axillary lymph-node dissection (ALND)–ACOSOG Z0011 results and beyond. Breast. 2013;22:211–6.
Anderson BO, Gralow JR. Axillary vs. sentinel lymph node dissection for invasive breast cancer. JAMA. 2011;305:2290; author reply 2290–1.
Fayda M, Chen R. Axillary vs. sentinel lymph node dissection for invasive breast cancer. JAMA. 2011;305:2289; author reply 2290–1.
Vuthaluru S, Srivastava A. Axillary vs. sentinel lymph node dissection for invasive breast cancer. JAMA. 2011;305:2290; author reply 2290–1.
Krishnan MS, Recht A, Bellon JR, Punglia RS. Trade-offs associated with axillary lymph node dissection with breast irradiation versus breast irradiation alone in patients with a positive sentinel node in relation to the risk of non-sentinel node involvement: implications of ACOSOG Z0011. Breast Cancer Res Treat. 2013;138:205–13.
Chen JJ, Wu J. Management strategy of early-stage breast cancer patients with a positive sentinel lymph node: With or without axillary lymph node dissection. Crit Rev Oncol Hematol. 2011;79:293–301.
Barry JM, Weber WP, Sacchini V. The evolving role of axillary lymph node dissection in the modern era of breast cancer management. Surg Oncol. 2012; 21: 143–145.
Yi M, Kuerer HM, Mittendorf EA, et al. Impact of the American College of Surgeons Oncology Group Z0011 criteria applied to a contemporary patient population. J Am Coll Surg. 2013;216:105–13.
Dengel LT, Van Zee KJ, King TA, et al. Axillary dissection can be avoided in the majority of clinically node-negative patients undergoing breast-conserving therapy. Ann Surg Oncol. 2014;21:22–7.
Van Zee KJ, Manasseh DM, Bevilacqua JL, et al. A nomogram for predicting the likelihood of additional nodal metastases in breast cancer patients with a positive sentinel node biopsy. Ann Surg Oncol. 2003;10:1140–51.
Hwang RF, Krishnamurthy S, Hunt KK, et al. Clinicopathologic factors predicting involvement of nonsentinel axillary nodes in women with breast cancer. Ann Surg Oncol. 2003;10:248–54.
Barranger E, Coutant C, Flahault A, et al. An axilla scoring system to predict non-sentinel lymph node status in breast cancer patients with sentinel lymph node involvement. Breast Cancer Res Treat. 2005;91:113–9.
Pal A, Provenzano E, Duffy SW, et al. A model for predicting non-sentinel lymph node metastatic disease when the sentinel lymph node is positive. Br J Surg. 2008;95:302–9.
Kohrt HE, Olshen RA, Bermas HR, et al. New models and online calculator for predicting non-sentinel lymph node status in sentinel lymph node positive breast cancer patients. BMC Cancer. 2008;8:66.
Gill G. Sentinel-lymph-node-based management or routine axillary clearance? One-year outcomes of sentinel node biopsy versus axillary clearance (SNAC): a randomized controlled surgical trial. Ann Surg Oncol. 2009;16:266–75.
Veronesi U, Paganelli G, Viale G, et al. Sentinel lymph node biopsy and axillary dissection in breast cancer: results in a large series. J Natl Cancer Inst. 1999;91:368–73.
Krag DN, Anderson SJ, Julian TB, et al. Sentinel-lymph-node resection compared with conventional axillary-lymph-node dissection in clinically node-negative patients with breast cancer: overall survival findings from the NSABP B-32 randomised phase 3 trial. Lancet Oncol. 2010;11:927–33.
Canavese G, Catturich A, Vecchio C, et al. Sentinel node biopsy compared with complete axillary dissection for staging early breast cancer with clinically negative lymph nodes: results of randomized trial. Ann Oncol. 2009;20:1001–7.
Disclosure
The authors have no financial or commercial interests to disclose.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article

Cite this article
Chung, A., Gangi, A., Mirocha, J. et al. Applicability of the ACOSOG Z0011 Criteria in Women with High-Risk Node-Positive Breast Cancer Undergoing Breast Conserving Surgery. Ann Surg Oncol 22, 1128–1132 (2015). https://doi.org/10.1245/s10434-014-4090-y
Received:
Published:
Issue Date:
DOI: https://doi.org/10.1245/s10434-014-4090-y