
Abstract
Several groups have reported association between large CAG/CTG repeats in the genome and BP disorder using the Repeat Expansion Detection (RED) method. Molecular interpretation studies demonstrated that around 90% of the large CAG/CTG repeats detected by RED can by explained by repeat size at either the CTG18.1 or ERDA-1 locus. In this study we report the findings on a large European BP case-control sample analysed for these two frequently expanded repeats. The frequency of expanded alleles (>40 repeats) at the CTG18.1 locus was significantly higher in the subgroup of patients with a more severe phenotype BPI and a positive first degree family history than in a group of matched controls (9% vs 5%). No difference in ERDA-1 expansion frequency was seen between BP cases and matched controls. We conclude that the ERDA-1 locus is not related to the BP phenotype while expanded alleles at the CTG18.1 locus cannot be excluded as a vulnerability factor for BP disorder.
Similar content being viewed by others


Introduction
Bipolar (BP) disorder is a severe psychiatric condition affecting about 1% of the population and is characterised by disturbances in mood, ranging from an extreme state of mania to a severe state of depression. BP illness type I (BPI) is characterised by major depressive episodes alternated with phases of mania, and type II (BPII) is characterised by major depressive episodes alternating with phases of hypomania. Relatives of BP probands have an increased risk for BP spectrum disorders, comprising of BP and unipolar disorder, cyclothymia and schizoaffective disorders.
Anticipation – an increase in disease severity in successive generations – has been described in BP disorder1,2,3,4,5 and gained renewed attention with the demonstration of a causal relationship between anticipation and triplet repeat expansions in several neurodegenerative diseases.6 A number of groups have tested this hypothesis using the Repeat Expansion Detection (RED) method, which identifies the size of the largest trinucleotide repeat present in the genome of an individual.7 Of eight independent studies four reported an association between expanded RED products and BP disorder5,6,7,8,9,10 while another four did not find a significant association.11,12,13,14 Unfortunately, the RED method cannot identify the specific repeat(s) responsible for these findings. Recently it was shown that about 90% of the large CAG/CTG repeats (repeat size ⩾40 units) detected by RED can be explained by two loci.15,16,17,18 The first locus is CTG18.1, which maps to 18q21.1 and is located in the third intron of the SEF2-1 gene. SEF2-1 encodes one of a family of basic helix–loop–helix proteins that bind to promoter sequences to regulate transcription of genes.19 The CTG18.1 locus is also of particular interest for bipolar disorder since linkage has been reported in the immediate genetic vicinity.20,21 The second locus is called ERDA-1, also known as Dir-I and maps to 17q21.3.22,23 Although this repeat may be transcribed, its function, if any, remains unknown. 23
Previously, we reported association between expanded RED CAG/CTG products and bipolar disorder in a sample of 51 unrelated BP patients and 99 matched controls of Belgian ancestry.8 In the same study, a Swedish BP sample showed similar results. The association was strongest in BPI patients with a familial history of affective disorders. Our group also replicated this finding in a BP case-control sample from Croatia.10 Subsequent analysis of both the Belgian and Swedish case-control samples with the two known CAG/CTG repeat loci showed a significant association between expanded ERDA1 alleles and BP disorder (P=0.04) in a Belgian sample and between CTG18.1 alleles and BP disorder (P<0.03) in the Swedish sample.16,18 These data suggest that the associations between BP disorder and large CAG/CTG RED products may be explained at least in part by a specific association between BP disorder and CTG18.1 and/or ERDA-1. To test this hypothesis we determined the frequency of the CTG18.1 and ERDA-1 alleles in a large combined European case-control sample composed of BP subjects and age, gender and ethnicity matched controls from Belgium, Croatia, Denmark, Scotland and Sweden.
Material and methods
Subjects
The patient and control subjects for this study were consecutively recruited in the five participating centres.24 Whole venous blood was used for the extraction of DNA by standard methods. Clinical evaluation of all patients was performed by a semi-structured interview using the Schedule for Affective Disorders and Schizophrenia–Lifetime Version (SADS–LA). Diagnosis of BP was made according to the Research Diagnostic Criteria (RDC). Control subjects were drawn from the respective populations and matched for age and gender. The Belgian sample in this study contains an overlap of 33 patients and 25 control individuals with a previous study.16
Genotyping
CTG18.1 and ERDA-1 primer sequences and the respective PCR conditions were as described18 and were used in all participating laboratories.
Genotyping of the Croatian, Belgian and Swedish samples was performed by a two-stage procedure. First, PCR was carried out for each locus with one of the primers labelled with a fluorescent dye. One microlitre of the PCR product was denaturated, run on a 6% denaturing polyacrylamide gel and analysed on an ABI 377 DNA sequencer using the Genescan and Genotyper 2.0 software. Second, all PCR products were reanalysed to allow detection of expanded alleles that might not be identified during the fluorescent analysis. Ten μl of the PCR product was separated on a 2% agarose gel, blotted to Hybond N+ membranes, fixed and hybridised at 58°C for at least 2 h with a γ-32P-ATP end-labelled (CAG)10 oligonucleotide. Membranes were washed and autoradiographed for 0.5 to 4 h.
Genotyping of the Scottish and Danish sample was performed by a one-stage procedure. PCR products were heat denatured and subsequently separated on a 6% denaturing polyacrylamide gel. DNA from the polyacrylamide gel was blotted to Hybond N+ membranes, fixed and hybridised at 58°C for at least 2 h with a γ-32P-ATP end-labelled (CAG)10 oligonucleotide. Membranes were washed and autoradiographed for 0.5 to 12 h.
Two raters performed sizing of the alleles independently and blind with respect to case/control status. An error checking procedure was implemented to insure standardisation of genotyping. For this purpose, each analysis included 3 CEPH individuals to correct for inter-gel variation and five random samples from each participating group were analysed and scored by the reference laboratory in Antwerp.
Statistical analysis
Statistical analysis (allelic and genotypic) was performed by dichotomous analysis, classifying the alleles at each locus in a group of ‘long’ alleles in the case the repeat number was ⩾40 and a group of ‘short’ alleles if the number of repeats was less than 40. This classification has no biological validity but is based upon the RED method, which yields a lower allele size of 40 repeats. The hypothesis of association between BP disorder and expansion at the ERDA-1 or CTG18.1 locus was tested by a χ2 analysis. Secondary analyses were performed after stratification for family history of affective disorder in first-degree relatives and/or severity of the disease reflected by BPI diagnosis. In case stratification was used, the significance level of allelic and genotypic association was adjusted according to the number of comparisons used (Bonferroni approach). The significance level after stratification for disease severity was set at 0.025 (i.e. 0.05/2) while the significance level after stratification for disease severity and family history was set at 0.017 (i.e. 0.05/3).
Results
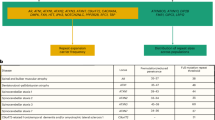
The total sample consisted of 889 subjects, 403 BP patients and 486 controls. A total of 889 CTG18.1 and 884 ERDA-1 typings were generated for analysis (Table 1). Statistical analysis of expanded allele frequencies between the respective control groups showed no deviation from Hardy–Weinberg equilibrium among the five control groups. The dichotomized frequencies for the individual as well as combined control populations and affected populations are shown in Table 2.
In the individual samples the two repeat loci ERDA-1 and CTG18.1 showed no significant difference at either locus, in the frequency of large alleles in the BP group compared with the controls under the dichotomous model (Table 2). However, a borderline statistical significant difference was observed for the CTG18.1 locus in the Croatian sample after stratification for first-degree family history and BPI (χ2=4.42, P=0.04). Analysis of the combined BP sample did not show a significant difference at either of the two CAG/CTG repeat loci. After stratification for first-degree family history and disease severity (BPI), a borderline significant difference was found (χ2=4.54, P=0.03).
Genotypic analysis of the two repeat loci in the individual samples showed no significant difference at either locus nor in the combined sample (all P-values >0.1). However, a borderline statistical significant difference was observed for the CTG18.1 locus in the combined sample after stratification for first-degree family history and BPI (χ2=6.33, P=0.02). For BPI familial cases, the relative risk of the CTG18.1 homozygous expanded genotype is 2.43 (95% CI: 1.37–4.33).
Discussion
We genotyped a large combined BP case-control sample of individuals derived from populations of European descent with two frequently expanded CAG/CTG containing loci in normal individuals: ERDA-1 and CTG18.1. In the controls we observed expansion frequencies of 26% (range 20–32%) for ERDA-1 and 5% (range 3–7%) for CTG18.1 (Table 2), which is in agreement with previously published repeat frequencies.16,18,19,22,23,25
Dichotomous analysis of the combined sample for ERDA-1 does not support the involvement of this repeat locus in BP disorder, except for a borderline effect in the Belgian familial BPI cases (P=0.07). In a previous study by our group,18 we found a larger proportion of BP patients carrying an expanded ERDA-1 allele than controls (P=0.03). This was not replicated in other studies.14,16
Statistical analysis of the genotypes from the CTG18.1 locus showed a higher frequency of expanded CTG18.1 repeats in BP individuals as compared to controls, after stratification for first degree family history and BPI in the Croatian sample (P=0.04). The results from the Croatian sample are in agreement with a previous study by our group, which showed that expanded RED products are associated with familial BPI subjects.10
There is no difference in the distribution of expanded alleles in the BP cases versus controls in the overall sample, which is in agreement with the data reported by McInnes et al.25 However, a difference in frequencies of expanded CTG18.1 alleles is present between BPI cases with a first degree family history and controls (P=0.03). These findings support those of Lindblad et al.16 who reported an association with enlarged alleles at the CTG18.1 locus in a sample of BP disorder (P<0.03). The replication of this finding in the present study which is much larger (403 BP cases) than the Lindblad et al.16 study (60 BP cases), renders further support to the specific hypothesis that SEF2-1 cannot be excluded as a susceptibility gene for bipolar disorder. Moreover, genotypic analyses showed that there is a relative risk of 2.4 of developing BP disorder in BPI familial cases homozygous for the expanded allele.
Our finding is of particular interest since at least two studies showed linkage in the immediate vicinity of CTG18.1.20,21 CTG18.1 was of particular interest in the Belgian BP family MAD31, since this family was previously shown to segregate with markers from chromosome 18q21.3–18q23.21 However, CTG18.1 is not expanded in family MAD3118 and we recently located CTG18.1 outside the BP candidate region defined in MAD31.17 Nevertheless, the possibility exists that CTG18.1 is in linkage disequilibrium with a causal gene for BP disorder.
Also, CTG18.1 is located within the third intron of the SEF2-1 gene, coding for a transcription factor that is widely expressed, including in brain.19 Altered expression of the SEF2-1 gene as a direct consequence of the presence of expanded CTG18.1 alleles can have profound effects on cellular processes in cells expressing the SEF2-1 gene. Furthermore, the repeat is transcribed into a prepro-mRNA CTG sequence and could potentially play a role similar to that of the untranslated CTG repeat in myotonic dystrophy.26
In summary, we have shown in a large combined BP case-control sample of European origin that CTG18.1 expansions are over-represented in familial BPI cases as compared to age, gender and ethnicity matched controls. The exact nature of this finding is not clear at this time but indicates that the expanded CTG18.1 repeats may predispose to affective disorder.
References
McInnis MG, McMahon FJ, Chase G, Simpson SG, Ross CA, DePaulo JR . Anticipation in Bipolar Affective Disorder Am J Hum Genet 1993 53: 385–390
Nylander PO, Engstrom C, Chotai J, Wahlstrom J, Adolfsson R . Anticipation in Swedish families with bipolar affective disorder J Med Genet 1994 31: 686–689
Engstrom C, Thornlund AS, Johansson EL et al. Anticipation in unipolar affective disorder J Affect Dis 1995 35: 31–40
Grigoroiu-Serbanescu M, Wickramaratne PJ, Hodge SE, Milea S, Mihailescu R . Genetic Anticipation and Imprinting in Bipolar Illness Br J Psychiatry 1997 170: 162–166
Mendlewicz J, Lindblad K, Souery D et al. Expanded trinucleotide CAG repeats in families with bipolar affective disorder Biol Psychiatry 1997 42: 1115–1122
Margolis RL, McInnes MG, Rosenblatt A, Ross CA . Trinucleotide repeat expansion and neuropsychiatric disease Arch Gen Psychiatry 1999 56: 1019–1031
Schalling M, Hudson TJ, Buetow KH, Housman DE . Direct detection of novel expanded trinucleotide repeats in the human genome Nat Genet 1993 4: 135–139
Lindblad K, Nylander PO, DeBruyn A et al. Detection of expanded CAG repeats in Bipolar Affective Disorder using the repeat expansion detection (RED) method Neurobiol Dis 1995 2: 55–62
O'Donovan MC, Guy C, Craddock N et al. Confirmation of association between expanded CAG/CTG repeats and both schizophrenia and bipolar disorder Psychol Med 1996 26: 1145–1153
Oruc L, Lindblad K, Verheyen G et al. CAG Repeat Expansions in Bipolar and Unipolar Disorders Am J Hum Genet 1997 60: 730–732
Vincent JB, Petronis A, Strong E et al. Analysis of genome-wide CAG/CTG repeats, and at SEF2-1B and ERDA1 in schizophrenia and bipolar affective disorder Mol Psychiatry 1999 4: 229–234
Li T, Vallada HP, Liu X et al. Analysis of CAG/CTG repeat size in Chinese subjects with schizophrenia and bipolar disorder using the repeat expansion detection method Biol Psychiatry 1998 44: 1160–1165
Zander C, Schurhoff F, Laurent C et al. CAG repeat sequences in bipolar affective disorder: no evidence for association in a french population Am J Med Genet 1998 81: 338–341
Guy CA, Bowen T, Jones I et al. CTG18.1 and ERDA-1 CAG/CTG repeat size in bipolar disorder Neurobiol Dis 1999 6: 302–307
Sidransky E, Burgess C, Ikeuchi T et al. A triplet repeat on 17q accounts for most expansions detected by the repeat-expansion-detection technique Am J Hum Genet 1998 62: 1548–1551
Lindblad K, Nylander PO, Zander C et al. Two commonly expanded CAG/CTG repeat loci – involvement in affective disorders? Mol Psychiatry 1998 3: 405–410
Verheyen G, Villafuerte S, Del-Favero J et al. Genetic refinement and physical mapping of a chromosome 18q candidate region for bipolar disorder Eur J Hum Genet 1998 7: 427–434
Verheyen G, Del-Favero J, Mendlewicz J et al. Molecular interpretation of expanded RED products in bipolar disorder by CAG/CTG repeats located at chromosomes 17q and 18q Neurobiol Dis 1999 6: 424–432
Breschel TS, McInnis MG, Margolis RL et al. A novel, heritable, expanding CTG repeat in an intron of the SEF2-1 gene on chromosome 18q21.1 Hum Mol Genet 1997 11: 1155–1163
Stine OC, Xu J, Koskela R et al. Evidence for linkage of bipolar disorder to chromosome 18 with a parent-of-origin effect Am J Hum Genet 1995 57: 1384–1394
De Bruyn A, Souery D, Mendelbaum K, Mendlewicz J, Van Broeckhoven C . Linkage analysis in families with bipolar illness and chromosome 18 markers Biol Psychiatry 1996 39: 679–688
Nakamoto M, Takebayashi H, Kawaguchi Y et al. A CAG/CTG expansion in the normal population Nat Genet 1997 17: 385–386
Ikeuchi T, Sanpei K, Takano H et al. A novel long and unstable CAG/CTG trinucleotide repeat on chromosome 17q Genomics 1998 49: 321–326
Souery D, Lipp O, Mahieu B et al. Association study of bipolar disorder with candidate genes involved in catecholamine neurotransmission: DRD2, DRD3, DAT1 and TH genes Am J Med Genet 1996 67: 551–555
McInnis MG, Swift-Scanlanl T, Mahoney A et al. Allelic distribution of CTG18.1 in Caucasian populations: association studies in bipolar disorder, schizophrenia, and ataxia Mol Psychiatry 2000 5: 439–442
Brook JD, McCurrach ME, Harley HG et al. Molecular basis of myotonic dystrophy: expansions of a trinucleotide (CTG) repeat at the 3′ end of a transcript encoding a protein kinase family member Cell 1992 68: 799–808
Acknowledgements
Sofie Van Gestel is a PhD fellow from the Fund for Scientific Research Flanders (FWO). The work described in this paper was in part funded by the FWO-Flanders (Belgium) and an EU grant BIOMED2 CT97-2466.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Del-Favero, J., Gestel, S., Børglum, A. et al. European combined analysis of the CTG18.1 and the ERDA1 CAG/CTG repeats in bipolar disorder. Eur J Hum Genet 10, 276–280 (2002). https://doi.org/10.1038/sj.ejhg.5200803
Received:
Revised:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1038/sj.ejhg.5200803
