
Abstracts
Parkinson’s disease (PD) is the second most common progressive neurodegenerative disease worldwide. However, there is no available therapy reversing the neurodegenerative process of PD. Based on the loss of dopamine or dopaminergic dysfunction in PD patients, most of the current therapies focus on symptomatic relief to improve patient quality of life. As dopamine replacement treatment remains the most effective symptomatic pharmacotherapy for PD, herein we provide an overview of the current pharmacotherapies, summarize the clinical development status of novel dopaminergic agents, and highlight the challenge and opportunity of emerging preclinical dopaminergic approaches aimed at managing the features and progression of PD.
Similar content being viewed by others


Introduction
Parkinson’s disease (PD) is a chronic, multicentric, and progressive neurodegenerative disease affecting 2%–3% of the population over the age of 60 years and is secondary only to Alzheimer’s disease (AD) [1, 2]. The pathological hallmark of PD is progressive and selective loss of dopaminergic neurons in the pars compacta of the substantia nigra (SNpc) and accumulation of α-synuclein (α-SN)-enriched intraneuronal aggregates termed Lewy bodies [2, 3]. Deficits in dopaminergic neurons results in the depletion of striatal dopamine (DA) production, leading to motor dysfunction, including resting tremor, bradykinesia, rigidity, and postural instability [3, 4]. In fact, patients have often already lost 60% of dopaminergic neurons from the SNpc when motor symptoms start to emerge at the onset of PD [5]. At that time, striatal DA in early PD patients is depleted by 80%. As the disease progresses to the later stage of PD, the involvement of nondopaminergic brain regions (e.g., the dorsal motor nucleus, locus coeruleus, substantia innominata, autonomic nervous system, and cerebral cortex) further causes the loss of nondopaminergic neurons such as cholinergic, serotonergic, glutamatergic, and noradrenergic neurons, consequently resulting in nonmotor symptoms, including hyposmia, psychiatric symptoms (e.g., depression and anxiety), rapid eye movement sleep behavior disorder, dementia, pain, fatigue, and constipation, in PD patients [4, 6,7,8,9,10,11,12,13,14].
Currently, PD is still incurable, as no treatment can stop or even slow down the progression of the disease, even though many research organizations focus on PD modification [15,16,17,18]. However, it is undeniable that various dopaminergic and nondopaminergic approaches for the treatment of the clinical symptoms of PD, including motor and nonmotor features, can improve the quality of life of PD patients for many years (Fig. 1). A number of excellent reviews on nondopaminergic therapeutics [5, 9, 19,20,21,22,23,24,25], including A2A receptor antagonists [26,27,28,29], muscarinic antagonists [30,31,32], serotonergics [33,34,35], and gluatamatergics [36,37,38,39], have discussed medicinal chemistry and clinical outcomes. As dopaminergics still represent the major therapeutic approaches for alleviating motor symptoms [40,41,42,43,44,45], this review will briefly introduce recent updates on approved PD treatments and highlight ongoing clinical efforts and recent progress on preclinical dopaminergic therapies aimed at managing the features and progression of PD since 2012.

Schematic of various strategies for PD treatment
Updates on currently approved PD treatments
Current PD therapeutic strategies, which mainly rely on the use of dopaminergic and nondopaminergic pharmacological agents for the treatment of the clinical symptoms of PD, are summarized in Tables 1 and 2. Since the early 1960s, DA replacement therapy has been the dominant therapy for the treatment of PD symptoms [46]. Levodopa (L-DOPA) [47, 48], a blood–brain barrier (BBB)-permeable DA biosynthetic precursor, is a mainstay of PD pharmacotherapy and compensates for the loss of DA and dopaminergic function through its conversion to DA by DA decarboxylase (Table 1). As L-DOPA is quickly metabolized by peripheral DA decarboxylase, monoamine oxidase-B (MAO-B), and/or catechol-O-methyltransferase (COMT), leading to poor efficacy and severe peripheral side effects, inhibitors of these enzymes were later developed as an add-on therapy to L-DOPA, to reduce the metabolism of L-DOPA and increase its central nervous system (CNS) concentration; this allowed the oral administration of lower doses of L-DOPA while maintaining the efficacy of L-DOPA and reducing its peripheral side effects such as nausea and hypotension. In 2017, safinamide [49, 50], a third-generation MAO-B inhibitor with reversibility and high selectivity that was originally developed to treat epilepsy, was approved by the Food and Drug Administration (FDA) as an adjunctive therapy to L-DOPA for PD patients with “wearing-off” episodes. Although L-DOPA is effective for symptomatic relief, its efficacy is diminished and it causes medication-related complications, particularly motor fluctuations and dyskinesia, such as L-DOPA-induced dyskinesia (LID), after chronic or long-term use [51,52,53,54].
Later, DA receptor agonists, such as those shown in Table 1, were developed either as monotherapies or combination therapies with L-DOPA for the treatment of PD. Five types of DA receptors, D1–D5, exist in the brain. The D1 and D5 receptors are grouped together as D1-like receptors based on their stimulatory effects on adenylyl cyclase (cAMP), and the D2, D3, and D4 receptors are classified as D2-like receptors due to their inhibition of cAMP activity. Many synthetic DA agonists, including pramipexole and apomorphine, activate D2-like receptors, and have a lower incidence of motor fluctuations and dyskinesia [45].
Another area of discovery in the past beyond dopaminergic-based treatments involved the examination of neurodegenerative processes in PD. Areas of the nondopaminergic system in which dysfunction occurs include the cholinergic, glutamatergic, adrenergic, adenosine, serotonergic, histaminic, and opioid pathways, and such dysfunction may also underlie motor and nonmotor symptoms of PD, thereby stimulating the development of miscellaneous nondopaminergic drugs, such as those shown in Table 2 [1, 9, 13, 55]. In general, muscarinic receptor antagonists, including benztropine, trihexyphenidyl, and biperiden, are used as adjuncts to PD treatment (e.g., L-DOPA), and they can also treat and prevent parkinsonian symptoms caused by the use of classic antipsychotic drugs (e.g., phenothiazines). Rivastigmine, a cholinesterase inhibitor, is used to treat mild-to-moderate dementia caused by AD or PD. Amantadine, a noncompetitive N-methyl-d-aspartate receptor antagonist, can treat PD and Parkinsonian symptoms. Most recently, istradefylline, the most extensively studied xanthine-based A2A antagonist, which was developed by Kyowa Kirin, Inc., and for which the first new drug application (NDA) submission was filed in 2007, was approved by the FDA as a first-in-class adenosine receptor type A2A antagonist. It is now used as a combination treatment with L-DOPA/carbidopa in adult PD patients experiencing “off” episodes.
Updates on the clinical progress of dopaminergic PD treatments
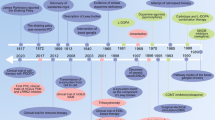
Despite the intensive efforts in PD research and development, there are clear unmet medical needs for the development of additional dopaminergic treatment options to improve current DA-centered treatment. Most currently used dopaminergic drugs selectively activate D2-like DA receptors (Table 1), but no D1-like selective agonists have been successfully approved even though the D1 receptor is a known target for PD treatment. Recently, important progress has been made in the clinical development of D1 selective agonists and allosteric modulators. All active dopaminergics since 2012 on the clinical trial website are summarized in Fig. 2 and Table 3.

Dopaminergics undergoing clinical trials
Dopamine stabilizers
Pridopidine (ACR16), which was developed by Neurosearch, is a DA stabilizer that improves motor symptoms by altering dopaminergic transmission via the dual effects of functionally low-affinity DA D2 receptor antagonism (Ki values of 17,550 nM and 7521 nM for D2 (low) and D2 (high), respectively) and strengthened cortical glutamate function [56, 57]. Originally, pridopidine was investigated for the symptomatic treatment of Huntington’s disease (HD), but two phase-3 trials sponsored by Teva did not show efficacy in improving voluntary motor function in HD patients. Later, it was found to display high binding affinity for human sigma-1 receptor (S1R) with a reported Ki value of 81.7 nM [58, 59]. Pridopidine was shown to improve functional neurorestoration, probably by acting on S1R, in a unilateral 6-hydroxydopamine (6-OHDA) lesion model of PD in mice [59]. Thus, pridopidine, a special D2 stabilizer with affinity for S1R, is currently being investigated in a phase 2 clinical study (NCT03922711) sponsored by Prilenia to evaluate its efficacy, safety and pharmacokinetics (PK) profile vs. placebo in PD patients experiencing LID.
D2 agonists
KDT3594 (structure undisclosed) is a D2 agonist developed by Kissei Pharmaceuticals [16]. A phase 2 study was initiated in February 2019 to investigate the efficacy, safety, and PK of KDT3594 vs. pramipexole in patients with early PD without concomitant treatment with L-DOPA (NCT03845387).
CLR4001 (CJH1, structure undisclosed) is a D2-specific agonist developed by Clera, Inc. [16]. A phase 2 clinical trial was initiated in 2012 to assess its ability to increase the sensitivity of DA receptors and thereby reduce the symptoms of PD. However, its clinical status is currently unknown.
D3 agonists
IRL790 (structure undisclosed) is a small molecule targeting DA D3 receptors with psychomotor stabilizing properties developed by Integrated Research Laboratories [16]. In experimental animals, IRL790 potently reduces L-DOPA-induced involuntary movement without impairing the anti-Parkinsonian effect of L-DOPA (NCT03368170). Initially, in 2016, Integrated Research Laboratories conducted a phase Ib clinical study of IRL790 in PD patients experiencing LID (NCT03531060). Later, a phase 2 study of IRL790 started in 2018, to investigate its efficacy and the optimal dose as an adjunctive treatment to reduce LID in PD patients (NCT03368170).
D1/D2 agonists
Lu AE04621, a prodrug of catecholamine, was developed as a D1/D2 agonist by Lundbeck’s neurodegeneration portfolio [16]. In 2016, a phase 1 trial of Lu AE04621 was performed in 15 PD patients, to evaluate its tolerability, efficacy, PK, and safety (NCT02649608). However, neither the clinical results nor its chemical structure have been disclosed thus far.
D1 agonists
As traditional D1-selective agonists are mainly catechol analogs and suffer from multiple challenges, such as low CNS penetration and poor metabolic stability, noncatechol agonists have become attractive due to their avoidance of such extensive metabolism [60,61,62]. Pfizer conducted several trials on clinical D1 agonists for the treatment of PD. A phase 1 study of PF-06669571 [63], a novel partial DA D1 receptor agonist, was initiated in 2014 to evaluate its safety and plasma concentrations following single and multiple ascending doses (NCT02184429) in healthy volunteers Later, in 2015, a phase 1 study in 20 participants with idiopathic PD was performed (NCT02565628). These results showed that multiple daily doses of PF-06669571 were well-tolerated and safe with no detectable safety concerns. However, the drug did not meet the pharmacodynamic endpoint of significant improvement [63].
PF-06649751 [64] represents another novel therapeutic candidate shown to exhibit highly selective DA D1/D5 agonism in phase 1 PD studies. Based on a primary clinical study of its safety, tolerability, PK profile, and efficacy, a larger clinical trial was subsequently conducted (NCT02224664 and NCT02373072). In 2017, Pfizer commenced a phase 2 trial of PF-06649751 to evaluate its long-term safety and tolerability in PD patients experiencing motor fluctuations. However, this study was terminated early, not due to safety concerns but due to a lack of demonstrated efficacy in improving PD symptoms (NCT03185481).
Another investigational drug is the noncatechol derivative PF-06412562, which is a moderately potent, orally bioavailable selective D1/D5 partial agonist [64, 65]. Since 2013, Pfizer has initiated ten phase 1 studies, eight of which were completed, one of which was terminated, and one of which had unknown outcomes. Most recently, a phase 1 study in healthy male volunteers assessed D1 receptor occupancy in the striatum after the oral administration of PF-06412562 (NCT03686501), whereas another study in advanced PD patients tested the safety and tolerability of PF-06412562 compared with that of the current medical standard of care for PD (carbidopa/L-DOPA), to determine whether it can help improve motor function, alertness, and cognitive skills (NCT03665454). The oral administration of PF-06412562 was shown to have potential anti-Parkinsonian efficacy without the significant acute cardiovascular effects previously reported with other D1 agonists [66].
D1-positive allosteric modulators
Allosteric modulators represent an alternative and promising strategy for G protein-coupled receptor (GPCR) drug discovery with high selectivity and low side effects. Eli Lilly developed the first clinical D1-positive allosteric modulator (PAM), LY3154207 [62, 67, 68], which shows no tachyphylaxis in preclinical animal models [62, 67, 68]. A phase 1 trial of LY3154207 in 80 participants, including healthy participants and PD patients, which studied the safety, tolerability, and PK of multiple ascending doses, was completed in 2017 (NCT02562768). Currently, a phase 2 study of LY3154207 in PD dementia (NCT03305809) is being performed.
COMT inhibitors
COMT inhibitors continue to be developed to extend the clinical effect of L-DOPA. The investigational drug opicapone was identified as a peripherally selective COMT inhibitor for once-daily use by Neurocrine Biosciences, Inc. [69,70,71]. Compared with the first two generations of COMT inhibitors, opicapone induces lower hepatotoxicity and requires less frequent dosing [72]. In fact, the European Commission has authorized opicapone as an adjunctive therapy to L-DOPA preparations in adult PD patients with end-of-dose motor fluctuations since June 2017. However, opicapone was not approved for use in the United States or Canada until recently. In July 2019, the FDA accepted a NDA for opicapone as an adjunctive treatment to L-DOPA/carbidopa in PD patients experiencing off episodes based on data from 38 clinical studies including two phase 3 studies (BIPARK-1 and BIPARK-2) in more than 1000 PD patients.
ODM-104 (structure undisclosed) is another COMT inhibitor that has been investigated. A phase 2 clinical trial (NCT02764125) sponsored by Orion Pharma to evaluate the safety and efficacy of ODM-104/L-DOPA/carbidopa vs. the standard of care (entacapone/L-DOPA/carbidopa) in PD patients with end-of-dose wearing-off (motor fluctuations) was completed in 2018.
Recent advances in the preclinical study of dopaminergic drugs for PD
Based on the multiple pathogenesis of PD, multifunctional agents may be good alternative options for PD treatment [5, 15, 41, 73,74,75,76,77,78]. Unfortunately, no such agents are available in the clinic. Table 4 summarizes the chemical structures and binding or agonistic activity of preclinical dopaminergics.
Dual D2/5-HT1A receptor agonists
5-HT1A receptors are critical for motor control and psychoemotional behavior in physiological and morbid states [33, 35, 79], particularly with respect to the involvement in LID; this has stimulated the development of dual D2/5-HT1A receptor agonists such as SOMCL-135 [80] and SOMCL-171 [81], as promising approaches for the treatment of PD [33, 41]. Compared with L-DOPA, both SOMCL-135 and SOMCL-171 elicit anti-Parkinsonian action in a 6-OHDA-lesioned rat model with slight dyskinesia. The chronic use of these agents attenuates the development of LID at no expense to their efficacy against PD.
Multifunctional agents with D2/D3 receptor agonist, antioxidant or iron chelating activities
Considering that D3-preferring agonists provide an additional neuroprotective effect compared with D2-preferring agonists [82,83,84,85,86], multifunctional agents with D3 agonistic activity have been developed to not only alleviate motor dysfunction in PD patients but also delay disease progression by protecting DA neurons from progressive degeneration. The Dutta group initially developed novel multifunctional agents with D2/D3 agonist activity along with antioxidant and iron chelating activities and the ability to modulate αSN aggregation, such as (−)-19 [87], D512 [88,89,90,91], D-520 [92, 93], D593 [44], D-607 [94, 95], D636 [96], D653 [96], and D656 (Table 4) [96]. Compared with ropinirole, (−)-19, D-520, D-593, D607, D636, D653, D656, and (−)-21a all exhibit in vivo efficacy in significantly reversing akinesia in reserpine-induced PD rats for a longer duration and exhibit neuroprotective effects against various types of toxicity. (±)-19 shows potent free radical scavenging activity and is nearly twofold more potent than ascorbic acid in quenching DPPH (1,1-diphenyl-2-picrylhydrazyl) radicals (IC50: 14.5 vs. 24.9 μM). D-593, D-636, D653, D656, and (−)-21a exhibit potent neuroprotective effects against 6-OHDA-induced toxicity in PC12 cells and efficiently modulate the aggregation of α-SN protein. D-520 not only modulates the in vitro aggregation of αSN but also shows significant protective effects against toxicity caused by αSN in fly eyes. Moreover, D-520 can protect MN9D cells from 6-OHDA toxicity. D607, as a D2/D3 agonist with efficient preferential iron (II) chelation properties, is neuroprotective against the neurotoxin Fe(III)-8HQ complex and 6-OHDA. D607 also significantly suppresses toxicity in an in vivo Drosophila melanogaster model expressing the α-SN protein in the fly eyes and reduces the levels of aggregated α-SN. Furthermore, D-607 rescues dopaminergic neurons from 1-methyl-4-phenyl-1,2,3,6-tetrahydropyridine (MPTP) toxicity in mice via both subchronic and chronic MPTP administration.
Compared with ropinirole, D512 exhibits superior peak-dose efficacy and longer duration effects in improving the rotational activity in the 6-OHDA-induced unilaterally lesioned rat model despite having similar side effects, including drug-induced dyskinesia. In addition, D512 protects dopaminergic MN9D cells from MPP+- and 6-OHDA-induced toxicity, inhibits lipid peroxidation and caspase 3/7 activity, and rescues 6-OHDA-induced changes in nuclear morphology. Moreover, D512 protects rat adrenal pheochromocytoma PC12 cells from 6-OHDA-induced apoptotic cell death and rescues dopaminergic neurons in the MPTP mouse model of PD. Furthermore, D512 displays neuroprotective effects against oxidative insult produced by buthionine sulfoximine, an inhibitor of glutathione synthesis, and 6-OHDA in PC12 cells.
Multifunctional agents with D3 receptor agonist and antioxidant activities
The Dutta group also developed novel multifunctional agents with D3-preferring agonist activity along with antioxidant activity, such as the selective full D3 agonists D440 [90], (−)-34 [91], and (−)-9b [97] 2019-12-1933, and the selective partial D3 agonist (−)-8b [97]. D440 not only exhibits in vivo efficacy in rats with 6-OHDA-induced unilateral lesions but also protects dopaminergic MN9D cells from MPP+- and 6-OHDA-induced toxicity. Both (−)-34 and (−)-9b significantly increase locomotor activity in an animal model of reserpine-induced PD. Moreover, (−)-9b also exhibits strong in vivo activity in rats with 6-OHDA-induced unilateral lesions and protects MN9D cells from MPP+-induced toxicity. Of note, (−)-8b is a selective partial D3 agonist, but it also exhibits strong in vivo activity, both in reversing akinesia in reserpine-treated rats and inducing rotation in rats with 6-OHDA-induced unilateral lesions; additionally, its activity is more potent than that of (−)-9b. However, (−)-8b shows no neuroprotective effects against MPP+-induced toxicity in MN9D cells.
G-protein-biased selective D3 receptor agonists
SK609 (Fig. 3), a G-protein-biased selective D3 agonist, has no significant effect on β-arrestin signaling pathway or on the corresponding desensitization [98,99,100]. However, SK609 can significantly improve the performance of the impaired paw and normalize bilateral asymmetry in a hemi-Parkinsonian rodent model. Chronic treatment with SK609 does not induce any abnormal involuntary movements. Furthermore, SK609 can be combined synergistically with L-DOPA to improve motor deficits without aggravating dyskinesia.

Other dopaminergics examined in preclinical studies
Selective D1 receptor agonists
Selective D1 agonists have received a resurgence of attention over the last 3 years. As derivatives of catechols, all known selective D1 agonists exert short duration effects, because they are rapidly metabolized and desensitize D1 receptors after prolonged exposure [44]. Recently, potent noncatechol selective D1 agonists (Fig. 3) with good in vivo efficacy and promising pharmacokinetic properties were identified [62]. PF-2334 [60], a G-protein-biased D1 agonist, shows sustained plasma concentrations and induces robust in vivo pharmacological responses without functional tachyphylaxis. The oral administration of PF-2334 has potent in vivo effects both on eye-blink responses in nonhuman primates and in a unilateral 6-OHDA lesioned rodent model of PD. On the other hand, 10 [101], a balanced agonist with highly potent effects on both signaling pathways, also displays satisfactory PK profiles, including good BBB penetrance. Importantly, 10 displays in vivo anti-Parkinsonian activity, restoring locomotion and prodyskinetic potential while potentiating behaviors indicative of dyskinesia in a 6-OHDA-lesioned mouse model of PD.
D2/D3-positive allosteric modulators
Unlike direct acting DA agonists, a newly identified D2/D3 PAM (Fig. 3) [102] affects the affinity and/or efficacy of the endogenous ligand, DA, with superior receptor-subtype selectivity and reduced desensitization. The racemic D2/D3 PAM lacks activity at all tested receptors, including D1, and lacks PAM activity at related Gi-coupled GPCRs; however, it potentiates the effect of DA at both the human D2 and D3 receptors in [35S]-GTPϒS and [3H]-DA binding assays. Its R isomer produces a greater improvement, whereas the S isomer is inactive. Moreover, this D2/D3 PAM potentiates in vivo effects on the level of L-DOPA-induced contralateral rotations in unilateral 6-OHDA-lesioned rats.
MAO-B selective inhibitors
The development of selective MAO-B inhibitors is still ongoing even though three selective MAO-B inhibitors have been approved for clinical use as add-on therapies and monotherapies [74, 103,104,105]. MAO-B inhibitors not only prolong the effectiveness of L-DOPA by increasing available DA but also demonstrate disease-modifying effects in preclinical models (e.g., neuroprotective effects against dopaminergic cell death). Polypharmacological ligands with MAO-B inhibitory effects along with iron chelation (e.g., M30 [106] and VAR10303 [107]), ChE inhibitory (e.g., Ladostigil [74] and MT-30R [108]), H3 antagonism (e.g., Contilisant [109]), or A2A antagonism (e.g., CSC [110]) properties have thus been developed on the basis of the complex pathogenesis of PD. The Cheong group [15] summarized the potential of MAO-B-related multitarget therapy as a treatment for PD in 2019. In addition, SU4312, a potent and selective inhibitor of vascular endothelial growth factor receptor-2 originally used as an anticancer agent, was identified as a dual ligand that protects against MPTP-associated neurotoxicity in PD in vitro and in vivo via the activation of the transcriptional activity of myocyte enhancer factor 2 and the inhibition of MAO-B [111].
On the other hand, there is still a pressing medical need for the development of reversible selective MAO-B inhibitors with effectiveness and safety for long-term use to treat PD [112]. Selegiline and rasagiline are irreversible MAO-B inhibitors with undesirable adverse effects, including hallucination and headache, the production of neurotoxic or ineffective metabolites, and gradual short-lived action after long-term use. Safinamide, a recently approved MAO-B inhibitor with high selectivity and reversibility, can also cause adverse effects due to undesirable actions, such as the inhibition of sodium and calcium channels and the stimulation of glutamate release [113,114,115]. Examples of highly selective MAO-B inhibitors tested preclinically for the treatment of PD are shown in Fig. 4. Compound 8 [116] (100 mg/kg) induces increases in motor activity, velocity and movement comparable with those induced by selegiline in mice pretreated with reserpine. SZV558 [117, 118] is not only protective against oxidative stress induced by 6-OHDA and rotenone during PC-12 cell death in vitro but also has neuroprotective effects against striatal DA depletion and motor dysfunction in vivo in MPTP-induced PD mice and in a chronic mouse model of MPTP plus probenecid administration. 5b [114] is a reversible selective MAO-B inhibitor with metabolic stability in human liver microsomes that has a minimal effect on CYP inhibition, and the oral administration of this inhibitor shows potent in vivo therapeutic efficacy on motor deficits similar to that of safinamide in an animal model of MPTP-induced PD. The oral administration of 12c [113] can significantly protect tyrosine hydroxylase-immunopositive DA neurons and attenuate PD-associated motor impairment in a mouse model of MPTP-induced PD.

Selective MAO-B inhibitors for preclinical PD treatment
Summary and perspectives
Although L-DOPA has been considered to be the most effective therapeutic strategy for PD for more than 50 years, currently approved drug therapies remain unsatisfactory since they only provide symptomatic relief but are unable to reverse disease progression. Additional options emerging in the clinic are symptomatic treatments. Although most agents currently being developed activate the D2 and D3 DA receptors, there has been a substantial research effort in efficaciously and selectively activating the DA D1 receptor, a known target for the treatment of PD that has been pursued for 40 years but for which there are no approved drugs. Recent clinical and preclinical advances in noncatechol selective D1R agonists have highlighted the potential to overcome the drawbacks of previous catechol selective D1R ligands. Moreover, the GS-mediated D1 receptor signaling pathway may be responsible for the development of LID, whereas β-arrestin2-mediated signaling may attenuate LID and remedy locomotor deficits; [117] thus, it is worth developing biased D1 DA ligands as valuable chemical tools for PD research. In addition, the identification of PAMs also offers new potentials for PD treatment [118,119,120]. Such endeavors will further expand the biological options for PD drugs.
The design of multitargeted ligands involved in neuroprotection, including MAO-B inhibitors, to address the medical limitations of current PD treatments continues to be an important focus with intensive preclinical and clinical efforts. Promising multifunctional lead molecules such as D-607, D636, and D653 have the potential to be viable symptomatic and disease-modifying PD therapies. A deep understanding of PD pathogenesis through biochemical and genetic characterization will shed more light on disease-modifying approaches for delaying the disease progression of PD.
References
Poewe W, Seppi K, Tanner CM, Halliday GM, Brundin P, Volkmann J, et al. Parkinson disease. Nat Rev Dis Prim. 2017;3:17013.
Lees AJ, Hardy J, Revesz T. Parkinson’s disease. Lancet. 2009;373:2055–66.
Obeso JA, Rodriguez-Oroz MC, Rodriguez M, Lanciego JL, Artieda J, Gonzalo N, et al. Pathophysiology of the basal ganglia in Parkinson’s disease. Trends Neurosci. 2000;23:S8–19.
Vu TC, Nutt JG, Holford NH. Progression of motor and nonmotor features of parkinson's disease and their response to treatment. Br J Clin Pharm. 2012;74:267–83.
Dauer W, Przedborski S. Parkinson's disease: mechanisms and models. Neuron. 2003;39:889–909.
Starkstein SE, Brockman S. Management of depression in Parkinson’s disease: a systematic review. Mov Disord Clin Pr. 2017;4:470–7.
Doty RL. Olfaction in Parkinson’s disease and related disorders. Neurobiol Dis. 2012;46:527–52.
Doty RL. Olfactory dysfunction in Parkinson disease. Nat Rev Neurol. 2012;8:329–39.
Fox SH. Non-dopaminergic treatments for motor control in Parkinson’s disease. Drugs. 2013;73:1405–15.
Suttrup I, Warnecke T. Dysphagia in Parkinson’s disease. Dysphagia. 2016;31:24–32.
Gratwicke J, Jahanshahi M, Foltynie T. Parkinson’s disease dementia: a neural networks perspective. Brain. 2015;138:1454–76.
Knie B, Mitra MT, Logishetty K, Chaudhuri KR. Excessive daytime sleepiness in patients with Parkinson’s disease. CNS Drugs. 2011;25:203–12.
Sanjari Moghaddam H, Zare-Shahabadi A, Rahmani F, Rezaei N. Neurotransmission systems in Parkinson’s disease. Rev Neurosci. 2017;28:509–36.
Marras C, Chaudhuri KR. Nonmotor features of Parkinson’s disease subtypes. Mov Disord. 2016;31:1095–102.
Cheong SL, Federico S, Spalluto G, Klotz KN, Pastorin G. The current status of pharmacotherapy for the treatment of Parkinson’s disease: transition from single-target to multitarget therapy. Drug Discov Today. 2019;24:1769–83.
Ellis JM, Fell MJ. Current approaches to the treatment of Parkinson’s disease. Bioorg Med Chem Lett. 2017;27:4247–55.
Kulisevsky J, Oliveira L, Fox SH. Update in therapeutic strategies for Parkinson’s disease. Curr Opin Neurol. 2018;31:439–47.
Smith Y, Wichmann T, Factor SA, DeLong MR. Parkinson’s disease therapeutics: new developments and challenges since the introduction of levodopa. Neuropsychopharmacology. 2012;37:213–46.
Freitas ME, Fox SH. Nondopaminergic treatments for Parkinson's disease: current and future prospects. Neurodegener Dis Manag. 2016;6:249–68.
Chaudhuri KR, Healy DG, Schapira AH.National Institute for Clinical Excellence Non-motor symptoms of Parkinson’s disease: diagnosis and management. Lancet Neurol. 2006;5:235–45.
Stayte S, Vissel B. Advances in non-dopaminergic treatments for Parkinson’s disease. Front Neurosci. 2014;8:113.
Muller T. Current and investigational non-dopaminergic agents for management of motor symptoms (including motor complications) in Parkinson’s disease. Expert Opin Pharmacother. 2017;18:1457–65.
Vanle B, Olcott W, Jimenez J, Bashmi L, Danovitch I, IsHak WW. NMDA antagonists for treating the non-motor symptoms in Parkinson’s disease. Transl Psychiatry. 2018;8:117.
Kalia LV, Brotchie JM, Fox SH. Novel nondopaminergic targets for motor features of Parkinson’s disease: review of recent trials. Mov Disord. 2013;28:131–44.
Guo L, Zhen X. Sigma-2 receptor ligands: neurobiological effects. Curr Med Chem. 2015;22:989–1003.
Zheng J, Zhang X, Zhen X. Development of adenosine a2a receptor antagonists for the treatment of Parkinson’s disease: a recent update and challenge. ACS Chem Neurosci. 2019;10:783–91.
Pinna A. Adenosine a2a receptor antagonists in Parkinson’s disease: progress in clinical trials from the newly approved istradefylline to drugs in early development and those already discontinued. CNS Drugs. 2014;28:455–74.
Cacciari B, Spalluto G, Federico S. A2a adenosine receptor antagonists as therapeutic candidates: are they still an interesting challenge? Mini Rev Med Chem. 2018;18:1168–74.
de Lera Ruiz M, Lim YH, Zheng J. Adenosine a2a receptor as a drug discovery target. J Med Chem. 2014;57:3623–50.
Katzenschlager R, Sampaio C, Costa J, Lees A Anticholinergics for symptomatic management of parkinson's disease. Cochrane Database Syst. Rev. 2003:CD003735.
Langmead CJ, Watson J, Reavill C. Muscarinic acetylcholine receptors as cns drug targets. Pharmacol Ther. 2008;117:232–43.
Conn PJ, Jones CK, Lindsley CW. Subtype-selective allosteric modulators of muscarinic receptors for the treatment of cns disorders. Trends Pharmacol Sci. 2009;30:148–55.
Huot P, Sgambato-Faure V, Fox SH, McCreary AC. Serotonergic approaches in Parkinson’s disease: translational perspectives, an update. ACS Chem Neurosci. 2017;8:973–86.
Politis M, Niccolini F. Serotonin in Parkinson’s disease. Behav Brain Res. 2015;277:136–45.
Ohno Y, Shimizu S, Tokudome K, Kunisawa N, Sasa M. New insight into the therapeutic role of the serotonergic system in Parkinson’s disease. Prog Neurobiol. 2015;134:104–21.
Litim N, Morissette M, Di Paolo T. Metabotropic glutamate receptors as therapeutic targets in Parkinson’s disease: an update from the last 5 years of research. Neuropharmacology. 2017;115:166–79.
Amalric M. Targeting metabotropic glutamate receptors (mglurs) in Parkinson’s disease. Curr Opin Pharm. 2015;20:29–34.
Charvin D. Mglu4 allosteric modulation for treating Parkinson’s disease. Neuropharmacology. 2018;135:308–15.
Lindsley CW, Emmitte KA, Hopkins CR, Bridges TM, Gregory KJ, Niswender CM, et al. Practical strategies and concepts in GPCR allosteric modulator discovery: recent advances with metabotropic glutamate receptors. Chem Rev. 2016;116:6707–41.
Ye N, Neumeyer JL, Baldessarini RJ, Zhen X, Zhang A. Update 1 of: Recent progress in development of dopamine receptor subtype-selective agents: potential therapeutics for neurological and psychiatric disorders. Chem Rev. 2013;113:PR123–178.
Ye N, Song Z, Zhang A. Dual ligands targeting dopamine D2 and serotonin 5-HT1A receptors as new antipsychotical or anti-Parkinsonian agents. Curr Med Chem. 2014;21:437–57.
Zhang A, Zhang Y, Branfman AR, Baldessarini RJ, Neumeyer JL. Advances in development of dopaminergic aporphinoids. J Med Chem. 2007;50:171–81.
Zhang A, Neumeyer JL, Baldessarini RJ. Recent progress in development of dopamine receptor subtype-selective agents: potential therapeutics for neurological and psychiatric disorders. Chem Rev. 2007;107:274–302.
Zhang J, Xiong B, Zhen X, Zhang A. Dopamine D1 receptor ligands: where are we now and where are we going. Medicinal Res Rev. 2009;29:272–94.
Alonso Canovas A, Luquin Piudo R, Garcia Ruiz-Espiga P, Burguera JA, Campos Arillo V, Castro A, et al. Dopaminergic agonists in Parkinson’s disease. Neurologia. 2014;29:230–41.
Fahn S. The history of dopamine and levodopa in the treatment of Parkinson’s disease. Mov Disord. 2008;23(Suppl 3):S497–508.
Salat D, Tolosa E. Levodopa in the treatment of Parkinson’s disease: current status and new developments. J Parkinsons Dis. 2013;3:255–69.
LeWitt PA, Fahn S. Levodopa therapy for parkinson disease: a look backward and forward. Neurology. 2016;86:S3–12.
Blair HA, Dhillon S. Safinamide: a review in Parkinson’s disease. CNS Drugs. 2017;31:169–76.
Dezsi L, Vecsei L. Safinamide for the treatment of Parkinson’s disease. Expert Opin Investig Drugs. 2014;23:729–42.
Espay AJ, Morgante F, Merola A, Fasano A, Marsili L, Fox SH, et al. Levodopa-induced dyskinesia in Parkinson disease: current and evolving concepts. Ann Neurol. 2018;84:797–811.
Brotchie JM, Lee J, Venderova K. Levodopa-induced dyskinesia in Parkinson’s disease. J Neural Transm. 2005;112:359–91.
Fisone G, Bezard E. Molecular mechanisms of L-DOPA-induced dyskinesia. Int Rev Neurobiol. 2011;98:95–122.
Jenner P. Molecular mechanisms of L-DOPA-induced dyskinesia. Nat Rev Neurosci. 2008;9:665–77.
Nutt JG, Bohnen NI. Non-dopaminergic therapies. J Parkinsons Dis. 2018;8:S73–S78.
Ponten H, Kullingsjo J, Lagerkvist S, Martin P, Pettersson F, Sonesson C, et al. In vivo pharmacology of the dopaminergic stabilizer pridopidine. Eur J Pharm. 2010;644:88–95.
Dyhring T, Nielsen EO, Sonesson C, Pettersson F, Karlsson J, Svensson P, et al. The dopaminergic stabilizers pridopidine (acr16) and (-)-osu6162 display dopamine d(2) receptor antagonism and fast receptor dissociation properties. Eur J Pharm. 2010;628:19–26.
Sahlholm K, Arhem P, Fuxe K, Marcellino D. The dopamine stabilizers acr16 and (-)-osu6162 display nanomolar affinities at the sigma-1 receptor. Mol Psychiatry. 2013;18:12–14.
Francardo V, Geva M, Bez F, Denis Q, Steiner L, Hayden MR, et al. Pridopidine induces functional neurorestoration via the sigma-1 receptor in a mouse model of Parkinson’s disease. Neurotherapeutics. 2019;16:465–79.
Gray DL, Allen JA, Mente S, O’Connor RE, DeMarco GJ, Efremov I, et al. Impaired beta-arrestin recruitment and reduced desensitization by non-catechol agonists of the D1 dopamine receptor. Nat Commun. 2018;9:674.
Wang P, Felsing DE, Chen H, Raval SR, Allen JA, Zhou J. Synthesis and pharmacological evaluation of noncatechol g protein biased and unbiased dopamine D1 receptor agonists. ACS Med Chem Lett. 2019;10:792–9.
Hall A, Provins L, Valade A. Novel strategies to activate the dopamine D1 receptor: recent advances in orthosteric agonism and positive allosteric modulation. J Med Chem. 2019;62:128–40.
Gurrell R, Duvvuri S, Sun P, DeMartinis N. A phase i study of the safety, tolerability, pharmacokinetics, and pharmacodynamics of the novel dopamine D1 receptor partial agonist, pf-06669571, in subjects with idiopathic Parkinson’s disease. Clin Drug Investig. 2018;38:509–17.
Sohur US, Gray DL, Duvvuri S, Zhang Y, Thayer K, Feng G. Phase 1 parkinson’s disease studies show the dopamine D1/D5 agonist pf-06649751 is safe and well tolerated. Neurol Ther. 2018;7:307–19.
Arce E, Balice-Gordon R, Duvvuri S, Naylor M, Xie Z, Harel B, et al. A novel approach to evaluate the pharmacodynamics of a selective dopamine D1/d5 receptor partial agonist (pf-06412562) in patients with stable schizophrenia. J Psychopharmacol. 2019;33:1237–47.
Papapetropoulos S, Liu W, Duvvuri S, Thayer K, Gray DL. Evaluation of D1/d5 partial agonist pf-06412562 in Parkinson’s disease following oral administration. Neurodegener Dis. 2018;18:262–9.
Hao J, Beck JP, Schaus JM, Krushinski JH, Chen Q, Beadle CD, et al. Synthesis and pharmacological characterization of 2-(2,6-dichlorophenyl)-1-((1 s,3r)-5-(3-hydroxy-3-methylbutyl)-3-(hydroxymethyl)-1 -methyl-3,4-dihydroisoquinolin-2(1 h)-yl)ethan-1-one (ly3154207), a potent, subtype selective, and orally available positive allosteric modulator of the human dopamine D1 receptor. J Med Chem. 2019;62:8711–32.
Svensson KA, Hao J, Bruns RF. Positive allosteric modulators of the dopamine D1 receptor: a new mechanism for the treatment of neuropsychiatric disorders. Adv Pharm. 2019;86:273–305.
Lees AJ, Ferreira J, Rascol O, Poewe W, Rocha JF, McCrory M, et al. Opicapone as adjunct to levodopa therapy in patients with Parkinson disease and motor fluctuations: a randomized clinical trial. JAMA Neurol. 2017;74:197–206.
Bonifacio MJ, Torrao L, Loureiro AI, Palma PN, Wright LC, Soares-da-Silva P. Pharmacological profile of opicapone, a third-generation nitrocatechol catechol-o-methyl transferase inhibitor, in the rat. Br J Pharm. 2015;172:1739–52.
Fabbri M, Ferreira JJ, Lees A, Stocchi F, Poewe W, Tolosa E, et al. Opicapone for the treatment of Parkinson’s disease: a review of a new licensed medicine. Mov Disord. 2018;33:1528–39.
Muller T. Catechol-o-methyltransferase inhibitors in Parkinson’s disease. Drugs. 2015;75:157–74.
Liu Z, Zhang J, Zhang A. Design of multivalent ligand targeting G-protein-coupled receptors. Curr Pharm Des. 2009;15:682–718.
Youdim MB, Kupershmidt L, Amit T, Weinreb O. Promises of novel multi-target neuroprotective and neurorestorative drugs for Parkinson’s disease. Parkinsonism Relat Disord. 2014;20(Suppl 1):S132–136.
Butini S, Nikolic K, Kassel S, Bruckmann H, Filipic S, Agbaba D, et al. Polypharmacology of dopamine receptor ligands. Prog Neurobiol. 2016;142:68–103.
Geldenhuys WJ, Van, der Schyf CJ. Rationally designed multi-targeted agents against neurodegenerative diseases. Curr Med Chem. 2013;20:1662–72.
Wu J, Du J, Gu R, Zhang L, Zhen X, Li Y, et al. Inhibition of neuroinflammation by synthetic androstene derivatives incorporating amino acid methyl esters on activated bv-2 microglia. ChemMedChem. 2015;10:610–6.
Meng XY, Mezei M, Cui M. Computational approaches for modeling GPCR dimerization. Curr Pharm Biotechnol. 2014;15:996–1006.
Liu Z, Zhang H, Ye N, Zhang J, Wu Q, Sun P, et al. Synthesis of dihydrofuroaporphine derivatives: identification of a potent and selective serotonin 5-HT 1A receptor agonist. J Med Chem. 2010;53:1319–28.
Zhang H, Ye N, Zhou S, Guo L, Zheng L, Liu Z, et al. Identification of n-propylnoraporphin-11-yl 5-(1,2-dithiolan-3-yl)pentanoate as a new anti-Parkinson’s agent possessing a dopamine D2 and serotonin 5-HT1A dual-agonist profile. J Med Chem. 2011;54:4324–38.
Zhao R, Lu W, Fang X, Guo L, Yang Z, Ye N, et al. 6ar)-11-amino-n-propyl-noraporphine, a new dopamine D2 and serotonin 5-HT1A dual agonist, elicits potent anti-Parkinsonian action and attenuates levodopa-induced dyskinesia in a 6-ohda-lesioned rat model of Parkinson’s disease. Pharmacol Biochem Behav. 2014;124:204–10.
Ye N, Wu Q, Zhu L, Zheng L, Gao B, Zhen X, et al. Further sar study on 11-o-substituted aporphine analogues: Identification of highly potent dopamine D3 receptor ligands. Bioorg Med Chem. 2011;19:1999–2008.
Zou L, Jankovic J, Rowe DB, Xie W, Appel SH, Le W. Neuroprotection by pramipexole against dopamine- and levodopa-induced cytotoxicity. Life Sci. 1999;64:1275–85.
Kim M, Lee S, Cho J, Kim G, Won C. Dopamine D3 receptor-modulated neuroprotective effects of lisuride. Neuropharmacology. 2017;117:14–20.
Ghosh B, Antonio T, Zhen J, Kharkar P, Reith ME, Dutta AK. Development of (s)-n6-(2-(4-(isoquinolin-1-yl)piperazin-1-yl)ethyl)-n6-propyl-4,5,6,7-tetrahydro benzo[d]-thiazole-2,6-diamine and its analogue as a D3 receptor preferring agonist: potent in vivo activity in Parkinson’s disease animal models. J Med Chem. 2010;53:1023–37.
Inden M, Kitamura Y, Tamaki A, Yanagida T, Shibaike T, Yamamoto A, et al. Neuroprotective effect of the antiparkinsonian drug pramipexole against nigrostriatal dopaminergic degeneration in rotenone-treated mice. Neurochem Int. 2009;55:760–7.
Johnson M, Antonio T, Reith ME, Dutta AK. Structure-activity relationship study of n(6)-(2-(4-(1h-indol-5-yl)piperazin-1-yl)ethyl)-n(6)-propyl-4,5,6,7-tetrahydroben zo[d]thiazole-2,6-diamine analogues: development of highly selective D3 dopamine receptor agonists along with a highly potent D2/D3 agonist and their pharmacological characterization. J Med Chem. 2012;55:5826–40.
Lindenbach D, Das B, Conti MM, Meadows SM, Dutta AK, Bishop C. D-512, a novel dopamine D2/3 receptor agonist, demonstrates greater anti-Parkinsonian efficacy than ropinirole in Parkinsonian rats. Br J Pharm. 2017;174:3058–71.
Shah M, Rajagopalan S, Xu L, Voshavar C, Shurubor Y, Beal F, et al. The high-affinity D2/D3 agonist d512 protects pc12 cells from 6-ohda-induced apoptotic cell death and rescues dopaminergic neurons in the MPTP mouse model of Parkinson’s disease. J Neurochem. 2014;131:74–85.
Santra S, Xu L, Shah M, Johnson M, Dutta A. D-512 and d-440 as novel multifunctional dopamine agonists: characterization of neuroprotection properties and evaluation of in vivo efficacy in a Parkinson’s disease animal model. ACS Chem Neurosci. 2013;4:1382–92.
Das B, Vedachalam S, Luo D, Antonio T, Reith ME, Dutta AK. Development of a highly potent D2/D3 agonist and a partial agonist from structure-activity relationship study of n(6)-(2-(4-(1h-indol-5-yl)piperazin-1-yl)ethyl)-n(6)-propyl-4,5,6,7-tetrahydroben zo[d]thiazole-2,6-diamine analogues: implication in the treatment of Parkinson’s disease. J Med Chem. 2015;58:9179–95.
Modi G, Voshavar C, Gogoi S, Shah M, Antonio T, Reith ME, et al. Multifunctional D2/D3 agonist d-520 with high in vivo efficacy: modulator of toxicity of alpha-synuclein aggregates. ACS Chem Neurosci. 2014;5:700–17.
Yedlapudi D, Joshi GS, Luo D, Todi SV, Dutta AK. Inhibition of alpha-synuclein aggregation by multifunctional dopamine agonists assessed by a novel in vitro assay and an in vivo Drosophila synucleinopathy model. Sci Rep. 2016;6:38510.
Das B, Rajagopalan S, Joshi GS, Xu L, Luo D, Andersen JK, et al. A novel iron (ii) preferring dopamine agonist chelator d-607 significantly suppresses alpha-syn- and MPTP-induced toxicities in vivo. Neuropharmacology. 2017;123:88–99.
Das B, Kandegedara A, Xu L, Antonio T, Stemmler T, Reith MEA, et al. A novel iron(ii) preferring dopamine agonist chelator as potential symptomatic and neuroprotective therapeutic agent for Parkinson’s disease. ACS Chem Neurosci. 2017;8:723–30.
Elmabruk A, Das B, Yedlapudi D, Xu L, Antonio T, Reith MEA, et al. Design, synthesis, and pharmacological characterization of carbazole based dopamine agonists as potential symptomatic and neuroprotective therapeutic agents for Parkinson’s disease. ACS Chem Neurosci. 2019;10:396–411.
Modi G, Antonio T, Reith M, Dutta A. Structural modifications of neuroprotective anti-Parkinsonian (-)-n6-(2-(4-(biphenyl-4-yl)piperazin-1-yl)-ethyl)-n6-propyl-4,5,6,7-tetrahydrobe nzo[d]thiazole-2,6-diamine (d-264): an effort toward the improvement of in vivo efficacy of the parent molecule. J Med Chem. 2014;57:1557–72.
Cote SR, Kuzhikandathil EV. In vitro and in vivo characterization of the agonist-dependent D3 dopamine receptor tolerance property. Neuropharmacology. 2014;79:359–67.
Simms SL, Huettner DP, Kortagere S. In vivo characterization of a novel dopamine D3 receptor agonist to treat motor symptoms of Parkinson’s disease. Neuropharmacology. 2016;100:106–15.
Xu W, Wang X, Tocker AM, Huang P, Reith ME, Liu-Chen LY, et al. Functional characterization of a novel series of biased signaling dopamine D3 receptor agonists. ACS Chem Neurosci. 2017;8:486–500.
Martini ML, Ray C, Yu X, Liu J, Pogorelov VM, Wetsel WC, et al. Designing functionally selective noncatechol dopamine D1 receptor agonists with potent in vivo anti-Parkinsonian activity. ACS Chem Neurosci. 2019;10:4160–82.
Wood M, Ates A, Andre VM, Michel A, Barnaby R, Gillard M. In vitro and in vivo identification of novel positive allosteric modulators of the human dopamine D2 and D3 receptor. Mol Pharm. 2016;89:303–12.
Dezsi L, Vecsei L. Monoamine oxidase b inhibitors in Parkinson’s disease. CNS Neurol Disord Drug Targets. 2017;16:425–39.
Robakis D, Fahn S. Defining the role of the monoamine oxidase-b inhibitors for Parkinson’s disease. CNS drugs. 2015;29:433–41.
Olanow CW. A rationale for monoamine oxidase inhibition as neuroprotective therapy for Parkinson’s disease. Mov Disord. 1993;8(Suppl 1):S1–7.
Youdim MB. Multi target neuroprotective and neurorestorative anti-Parkinson and anti-Alzheimer drugs ladostigil and m30 derived from rasagiline. Exp Neurobiol. 2013;22:1–10.
Bar-Am O, Amit T, Kupershmidt L, Aluf Y, Mechlovich D, Kabha H, et al. Neuroprotective and neurorestorative activities of a novel iron chelator-brain selective monoamine oxidase-a/monoamine oxidase-b inhibitor in animal models of Parkinson’s disease and aging. Neurobiol Aging. 2015;36:1529–42.
Liu Z, Cai W, Lang M, Yan R, Li Z, Zhang G, et al. Neuroprotective effects and mechanisms of action of multifunctional agents targeting free radicals, monoamine oxidase b and cholinesterase in Parkinson’s disease model. J Mol Neurosci. 2017;61:498–510.
Bautista-Aguilera OM, Hagenow S, Palomino-Antolin A, Farre-Alins V, Ismaili L, Joffrin PL, et al. Multitarget-directed ligands combining cholinesterase and monoamine oxidase inhibition with histamine h3 r antagonism for neurodegenerative diseases. Angew Chem Int Ed. 2017;56:12765–9.
Aguiar LM, Macedo DS, Vasconcelos SM, Oliveira AA, de Sousa FC, Viana GS. Csc, an adenosine a(2a) receptor antagonist and MAO B inhibitor, reverses behavior, monoamine neurotransmission, and amino acid alterations in the 6-OHDA-lesioned rats. Brain Res. 2008;1191:192–9.
Guo B, Hu S, Zheng C, Wang H, Luo F, Li H, et al. Substantial protection against MPTP-associated Parkinson’s neurotoxicity in vitro and in vivo by anti-cancer agent su4312 via activation of MEF2d and inhibition of MAO-B. Neuropharmacology. 2017;126:12–24.
Tripathi RKP, Ayyannan SR. Monoamine oxidase-B inhibitors as potential neurotherapeutic agents: an overview and update. Med Res Rev. 2019;39:1603–706.
Yeon SK, Choi JW, Park JH, Lee YR, Kim HJ, Shin SJ, et al. Synthesis and evaluation of biaryl derivatives for structural characterization of selective monoamine oxidase B inhibitors toward parkinson's disease therapy. Bioorg Med Chem. 2018;26:232–44.
Nam MH, Park M, Park H, Kim Y, Yoon S, Sawant VS, et al. Indole-substituted benzothiazoles and benzoxazoles as selective and reversible MAO-B inhibitors for treatment of Parkinson’s disease. ACS Chem Neurosci. 2017;8:1519–29.
Cattaneo C, Kulisevsky J, Tubazio V, Castellani P. Long-term efficacy of safinamide on Parkinson’s disease chronic pain. Adv Ther. 2018;35:515–22.
Matos MJ, Vilar S, Gonzalez-Franco RM, Uriarte E, Santana L, Friedman C, et al. Novel (coumarin-3-yl)carbamates as selective MAO-B inhibitors: synthesis, in vitro and in vivo assays, theoretical evaluation of adme properties and docking study. Eur J Med Chem. 2013;63:151–61.
Urs NM, Bido S, Peterson SM, Daigle TL, Bass CE, Gainetdinov RR, et al. Targeting beta-arrestin2 in the treatment of L-DOPA-induced dyskinesia in Parkinson’s disease. Proc Natl Acad Sci USA. 2015;112:E2517–2526.
Nickols HH, Conn PJ. Development of allosteric modulators of GPCRs for treatment of CNS disorders. Neurobiol Dis. 2014;61:55–71.
Conn PJ, Christopoulos A, Lindsley CW. Allosteric modulators of GPCRs: a novel approach for the treatment of CNS disorders. Nat Rev Drug Discov. 2009;8:41–54.
Conn PJ, Lindsley CW, Meiler J, Niswender CM. Opportunities and challenges in the discovery of allosteric modulators of GPCRs for treating CNS disorders. Nat Rev Drug Disco. 2014;13:692–708.
Luo D, Sharma H, Yedlapudi D, Antonio T, Reith MEA, Dutta AK. Novel multifunctional dopamine D2/D3 receptors agonists with potential neuroprotection and anti-alpha synuclein protein aggregation properties. Bioorg Med Chem. 2016;24:5088–102.
Acknowledgements
Financial support was obtained from the National Natural Science Foundation of China (81703330), the Natural Science Foundation of Jiangsu Province (BK20170347), the Priority Academic Program Development of the Jiangsu Higher Education Institutes (PAPD), and the Jiangsu Key Laboratory of Neuropsychiatric Diseases (BM2013003).
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Competing interests
The authors declare no competing interests.
Rights and permissions
About this article

Cite this article
Mao, Q., Qin, Wz., Zhang, A. et al. Recent advances in dopaminergic strategies for the treatment of Parkinson’s disease. Acta Pharmacol Sin 41, 471–482 (2020). https://doi.org/10.1038/s41401-020-0365-y
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1038/s41401-020-0365-y
