
Abstract
Valemetostat tosilate (valemetostat; EZHARMIA®), a selective dual inhibitor of histone-lysine N-methyltransferases enhancer of zeste homolog 1 and 2 (EZH1/2), is being developed by Daiichi Sankyo Company, Ltd for the treatment of various haematological malignancies and solid tumours, including types of non-Hodgkin lymphomas (NHL). Valemetostat was approved in Japan in September 2022 for the treatment of patients with relapsed or refractory adult T-cell leukaemia/lymphoma (R/R ATL), a subtype of NHL. This article summarizes the milestones in the development of valemetostat leading to this first approval for R/R ATL.
Similar content being viewed by others


Explore related subjects
Discover the latest articles, news and stories from top researchers in related subjects.Avoid common mistakes on your manuscript.
Digital Features for this AdisInsight Report can be found at https://doi.org/10.6084/m9.figshare.21405570 |
A selective dual inhibitor of EZH1/2 that is being developed by Daiichi Sankyo for the treatment of various haematological malignancies and solid tumours |
Received its first approval on 26 September 2022 in Japan |
Approved for the treatment of patients with R/R ATL |
1 Introduction
Epigenetic regulators of gene expression are an emerging new target class for cancer therapy, and numerous epigenetic therapies are currently in clinical development [1, 2]. Enhancer of zeste homolog 1 and 2 (EZH1 and EZH2) are alternative subunits of polycomb repressive complex 2 (PRC2) and initiate chromatin folding via tri-methylation of the 27th lysine residue of histone H3 (H3K27), resulting in repression of genes associated with tumour suppression and cell differentiation [3,4,5,6]. Epigenomic studies of chromatin and transcription regulation have shown that inappropriate H3K27me3 deposition [resulting from a gain-of-function (GOF) mutation of EZH2 and/or overexpression of EZH2] is a key determinant of the abnormal transcriptome and has been implicated in the development and progression of a range of solid tumours and lymphomas, including non-Hodgkin lymphomas (NHL) [4,5,6]. Other preclinical studies have shown that EZH1 is also involved in abnormal H3K27 methylation and compensates for loss of EZH2 after exposure of cells to EZH2 inhibition in vitro [5].
Among NHL subtypes, the most rare, aggressive and difficult to treat include adult T-cell leukaemia/lymphoma (ATL) [arises from T cells infected with human T-lymphotropic virus type 1 (HTLV-1)], peripheral T-cell lymphoma (PTCL), and B-cell lymphomas [7]. First-line treatment for these lymphoma subtypes is multiagent chemotherapy; however, the response to treatment is not durable, relapse is common and the prognosis is generally poor [3, 7,8,9]. Thus, there is a need for new treatment options.

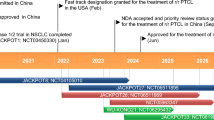
Key milestones in the development of valemetostat for the treatment of non-Hodgkin lymphomas. ATL adult T-cell leukaemia/lymphoma, BCL B-cell lymphoma, NDA new drug application, NHL non-Hodgkin lymphoma, PTCL peripheral T-cell lymphoma, R/R relapsed/refractory
Valemetostat tosilate (valemetostat; EZHARMIA®), an orally administered, selective dual inhibitor of both wild-type and mutated forms of EZH2 and EZH1 [10], has been developed by Daiichi Sankyo Company, Ltd for the treatment of cancers, and is being studied in NHL and a range of solid tumours. SAKIGAKE designation was granted in Japan in 2019 based on the preliminary results of a phase 1 trial of valemetostat in patients with NHL, including PTCL (NCT02732275) [11]. In September 2022, valemetostat was approved in Japan for the treatment of patients with relapsed or refractory (R/R) ATL [10, 12]. The approved dosage of valemetostat in patients with R/R ATL is 200 mg once daily on an empty stomach. Exposure to valemetostat (Cmax and AUC) is reduced when it is administered with or after food; patients should therefore avoid taking the drug between 1 h before and 2 h after food.
Patients should be carefully monitored for myelosuppression during valemetostat treatment [10]. If adverse reactions (neutropenia, thrombocytopenia, anaemia or ≥ grade 3 non-haematological toxicity) occur, treatment suspension is required until recovery. If the adverse reaction reappears after resumption of the same daily dose, treatment should again be suspended until recovery. After recovery, the administered dose should then be reduced by one step from the previous dose. Dose reduction due to adverse reactions should be limited to two levels, and the drug should be discontinued if a reduction to below 50 mg/day is required [10]. Exposure to valemetostat is increased when it is coadministered with drugs that are strong CYP3A and/or P-gp inhibitors, and valemetostat dosage reductions are required because of increased adverse reactions. In some instances, an appropriate reduction in the valemetostat dosage is not possible and coadministration should be avoided. Caution is required when valemetostat is coadministered with moderate CYP3A inhibitors (because of increased valemetostat exposure), strong or moderate CYP3A inducers (because of decreased valemetostat exposure) and P-gp substrates (exposure to P-gp substrate drugs may be increased) [10]. Clinical trials have not been conducted in patients with severe liver dysfunction. Contraception should be used during treatment and for a defined period after the last dose. Pregnant women should only be treated with valemetostat if the potential benefits outweigh the risks; embryofetal toxicity and teratogenicity have been reported in animal studies of valemetostat at exposures corresponding to ≈ 0.05 times clinical exposure in humans at the recommended dose. It is advisable not to breastfeed during treatment. Secondary malignancies, such as chronic myelomonocytic leukaemia and chronic leukaemia, have been reported in clinical studies and precursor B-cell acute leukaemia has been reported in paediatric neuroblastoma patients [10].
1.1 Company Agreements
In February 2021, Daiichi Sankyo entered into a research and development agreement with the Lymphoma Study Association (LYSA), the Lymphoma Academic Research Organization (LYSARC), and the CALYM Carnot Institute (LYSA-LYSARC-CALYM is a multidisciplinary community of the three organizations that conduct lymphoma research in France and Belgium). The strategic research collaboration is assessing valemetostat in B-cell malignancies, starting with a phase 2 study, and will build upon the ongoing phase 1 trial of valemetostat in patients with R/R NHL (i.e. study NCT02732275) [13]. In September 2017, the University of Texas MD Anderson Cancer Center entered into a multi-year research and development agreement with Daiichi Sankyo to accelerate development of acute myeloid leukemia therapies, including valemetostat [14]; however, the clinical study (NCT03110354) was terminated due to slow patient accrual.

Chemical structure of valemetostat tosilate
2 Scientific Summary
2.1 Pharmacodynamics
While the exact mechanism of action is unknown, it is thought that valemetostat inhibits the methylation activity of EZH1/2 [IC50 10.0 nM (EZH1) and 6.0 nM (EZH2) in cell-free enzymatic assays [15]], thereby inhibiting the methylation of the lysine residue at position 27 and other residues of histone H3 [10]. The decrease in histone methylation alters gene expression patterns associated with cancer pathways, enhances transcription of certain target genes, and reactivation of silenced genes results in decreased proliferation of EZH1/2-expressing cancer cells [15]. Preclinical research indicates that EZH1 and EZH2 play a role in haematological malignancy progression; in vitro, EZH1/2 dual inhibitors suppressed trimethylation of H3K27 in cells more strongly than EZH2 selective inhibitors [15, 16]. Valemetostat displayed antiproliferative effects in various haematological cancer cell lines [including various NHL cells (GI50 < 100 nM)] and clinical activity in a phase 1 trial in patients with R/R NHL (NCT02732275), regardless of EZH2 mutation status [16, 17]. While tazemetostat (a selective EZH2 inhibitor) and valemetostat significantly reduced global H3K27me3 levels in an in vitro study, ectopic EZH1/2 accumulation was evident after treatment with tazemetostat in several tumour suppressor gene loci, resulting in a partial reduction in H3K27me3 and reversal of the reactivation of silenced gene expression. In contrast, valemetostat treatment was not associated with ectopic enrichment of EZH1/2, and H3K27me3 levels remained depleted [18]. Valemetostat induced cell differentiation, growth inhibition and apoptosis in most subtypes of AML tested in vitro, with effects similar to those seen with genetic depletion of EZH1/2. However, a selective EZH2 inhibitor did not affect the growth and survival of AML cells to the same extent as valemetostat [19]. Oral administration of valemetostat reduced the number of leukaemia stem cells, impaired leukaemia progression and prolonged survival in AML mouse models and patient-derived xenograft models in a manner similar to the effect of genetic deletion of EZH1/2 [19].
In vitro, valemetostat showed antiproliferative activity against the TL-Om1 cell line derived from human ATL [10] and against the activated B-cell-like (ABC) and germinal center B-cell-like (GCB) subtypes of diffuse large B-cell lymphoma (DLBCL) cells, and induced apoptosis in DLBCL cell lines, regardless of subtype. Valemetostat also suppressed the expression level of BCL6 protein (a key oncogene in B cell lymphoma) in vitro [20]. Valemetostat blocked primary ATL cell survival in vitro and reduced in vivo tumour growth in ATL and DLBCL models [21]. Compared with an EZH2 selective inhibitor, various of models of haematological malignancies (ATL, DLBCL, Burkitt lymphoma and PTCL) showed greater sensitivity (5.2- to ≈ 200-fold) against valemetostat. No significant adverse effects were observed in normal T cells [21]. In a DLBCL tumour xenograft model, once daily oral administration of valemetostat 100 mg/kg was associated with almost complete tumour regression without weight loss; a lower dosage (25 mg/kg) slowed tumour growth [15]. Valemetostat also showed synergism with NHL and DLBCL standard-of-care treatments in vitro and in vivo [17, 20].
2.2 Pharmacokinetics
On day 15 after repeated administration of oral valemetostat 200 mg in the fasted state in a phase 2 study in 25 patients with R/R ATL (NCT04102150), the steady-state mean Cmax of total valemetostat (2300 ng/mL) was achieved in a median 3.79 h, AUC24 was 20,800 ng·h/mL and the mean accumulation ratio for total valemetostat was 1.19 [3, 10]. Food has a significant effect on the pharmacokinetics of valemetostat. After administration of a single 200 mg dose of valemetostat in healthy adults, the ratio of the geometric mean Cmax and AUC∞ values after a high fat meal to a fasting dose were 0.487 and 0.703, and those after a low fat meal to a fasting dose were 0.375 and 0.466, respectively [10]. Valemetostat is highly protein bound (94–95%) after administration of a 200 mg dose in healthy adults; valemetostat predominantly binds to human a1 acidic glycoprotein in vitro [10]. The apparent volume of distribution of total valemetostat at steady state was 268 L [3]. The human blood/plasma concentration ratios at low (300 ng/mL), medium (1,500 ng/mL) and high (5,000 ng/mL) concentrations in vitro were 0.58, 0.61 and 0.74, respectively [10].
Valemetostat is predominantly metabolized by CYP3A. After a single oral 200 mg dose of 14C-labelled valemetostat in healthy adults, the unchanged drug and an oxidized metabolite (CALZ-1809a) were detected in plasma. The ratio of the unchanged drug to AUC∞ of total radioactivity in plasma was 54.6% and the AUC∞ ratio of CALZ-1809a to the unchanged drug was 83.0% [10]. Valemetostat is mainly excreted in faeces; 79.8% of the total radioactivity excreted at up to 360 h after a single oral 200 mg dose of 14C-labelled valemetostat was detected in faeces and 15.6% was detected in urine. Unchanged valemetostat was excreted in both faeces (64.9%) and urine (10.0%) [10]. At steady state, the apparent oral clearance of total valemetostat was 58.1 L/h and the mean elimination half-life was 11.1 h [3].
After a single oral administration of valemetostat 50 mg in a US study (NCT04276662), the ratios of the geometric mean Cmax and AUC∞ of unbound valemetostat in subjects with normal hepatic function to subjects with mild hepatic impairment were 0.706 and 1.19, respectively, and in subjects with normal hepatic function to subjects with moderate hepatic impairment were 0.813 and 1.25 [10].
Exposure to valemetostat is increased when coadministered with the strong CYP3A and P-gp inhibitor itraconazole and the moderate CYP3A inhibitor fluconazole in healthy adults (JapicCTI183902) [22]. The ratios of the geometric mean Cmax and AUC∞ values after coadministration of valemetostat and itraconazole to administration of valemetostat alone were 2.92 and 4.19, while those after coadministration of valemetostat and fluconazole to administration of valemetostat alone were 1.61 and 1.58 [10, 22]. Exposure to valemetostat is decreased when coadministered with the strong CYP3A inducer rifampicin (JapicCTI205338) or with the moderate CYP3A inducer efavirenz. The ratios of the geometric mean Cmax and AUC∞ values after coadministration of valemetostat and rifampicin to administration of valemetostat alone in healthy adults were 0.417 and 0.286, while those after coadministration of valemetostat and efavirenz to administration of valemetostat alone were 0.666 and 0.575. In patients with R/R NHL, the ratios of the geometric mean Cmax and AUClast values after coadministration of valemetostat and midazolam (a substrate of CYP3A) to administration of valemetostat alone were 0.926 and 0.861, while those after coadministration of valemetostat and digoxin (a P-gp substrate) to administration of valemetostat alone were 1.30 and 1.27 [10]. According to pharmacokinetic modelling, the ratios of the geometric mean Cmax and AUC∞ values after coadministration of valemetostat and a strong CYP3A inhibitor to administration of valemetostat alone were predicted to be 2.13 and 2.67, the ratios of the geometric mean Cmax and AUC96 values after coadministration of valemetostat and a P-gp inhibitor to administration of valemetostat alone were predicted to be 1.59 and 2.58 [10]. Valemetostat is a substrate of and inhibitor of P-gp; it is also an MATE1 and MATE2-K and inhibits MATE1 in vitro (IC50 0.548 µmol/L) [10].
Features and properties of valemetostat
Alternative names | DS-3201; DS-3201b; EZHARMIA; valemetostat tosylate; valemetostat tosilate; (R)‐OR‐S2 |
Class | Amides; amines; antineoplastics; benzodioxoles; chlorinated hydrocarbons; cyclohexanes; pyridones; small molecules |
Mechanism of action | Enhancer of zeste homolog 1 protein inhibitors; enhancer of zeste homolog 2 protein inhibitors |
Route of administration | Oral |
Pharmacodynamics | Inhibits methylation activity of EZH1/2 [IC50 10.0 nM (EZH1) and 6.0 nM (EZH2), suppressing tri-methylation of H3K27; antiproliferative effects in haematological cancer cell lines [including various NHL cells (GI50 < 100 nM)], regardless of EZH2 mutation status; significantly reduces global H3K27me3 levels and reactivates silenced gene expression; antiproliferative activity against the TL-Om1 cell line derived from human ATL, and the ABC and GCB subtypes of DLBCL cells; induces apoptosis in DLBCL cell lines, regardless of subtype; blocks primary ATL cell survival in vitro and reduces ATL and DLBCL tumour growth in vivo; synergism with NHL and DLBCL standard-of-care treatments in vitro and in vivo |
Pharmacokinetics (total valemetostat at steady state; mean values unless stated) | Cmax 2300 ng/mL, median Tmax 3.79 h, AUC24 20,800 ng·h/mL, accumulation ratio 1.19, 94–95% protein bound, Vz/F 68 L, CL/F 58.1 L/h, t½ 11.1 h. Predominantly metabolized by CYP3A; mainly excreted in faeces |
Adverse events | |
Most frequent | Thrombocytopenia, anaemia, alopecia, dysgeusia, lymphopenia, neutropenia, leukopenia |
Of special interest | Thrombocytopenia |
ATC codes | |
WHO ATC code | L01 (antineoplastic agents) |
EphMRA ATC code | L1 (antineoplastics) |
Chemical name | (2R)-7-Chloro-2-[trans-4-(dimethylamino)cyclohexyl]-N-[(4,6-dimethyl-2-oxo-1,2-dihydropyridin-3-yl)methyl]-2,4-dimethyl-1,3-benzodioxole-5-carboxamide mono(4- methylbenzenesulfonate) |
2.3 Therapeutic Trials
Valmetostat 200 mg once daily showed promising efficacy in in patients with R/R ATL in a phase 2 Japanese trial (NCT04102150) [3]. The primary endpoint was achieved, in that the centrally reviewed independent efficacy assessment committee (IEAC)-assessed overall response rate (ORR) was 48% (12/25 patients; p < 0.0001). A complete response (CR) was seen in 20% of patients (5/25) and a partial response (PR) in 28% (7/25). 40% of patients (10/25) had stable disease (SD) and 12% (3/25) had relapse or disease progression (RD/PD). The ORR by disease subtype was 62.5% (10/16) for acute, 16.7% (1/6) for lymphoma, and 33.3% (1/3) for unfavourable chronic types. The tumour control rate (CR + PR + SD) was 88.0% (22/25 patients). In patients who had received prior treatment with mogamulizumab, the ORR was 45.8% (11/24 patients), while in those who were refractory to mogamulizumab the ORR was 50.0% (3/6). The median follow-up at data cut-off (24 April 2021) was 6.5 months. At data cut-off, the IEAC-assessed median time to response was 1.4 months and 8 patients were continuing to receive treatment; the IEAC-assessed median duration of response (DOR) had not been reached [3].
Eligible patients in this study were aged ≥ 20 years, had cytologically or pathologically diagnosed R/R ATL (acute, lymphoma, or unfavourable chronic types), antibody-confirmed HTLV-1 infection and had failed prior mogamulizumab therapy or, if mogamulizumab was contraindicated/not tolerated, ≥1 systemic therapy with cytotoxic chemotherapy. Patients who had received prior allogeneic or autologous hematopoietic stem cell transplantation as treatment for AST were excluded from the study because of potential worsening of graft-versus-host disease. At baseline, the median age was 69.0 years and patients had received a median three prior lines of therapy (24 of 25 participants had received prior treatment with mogamulizumab; one patient was CCR4 negative and was not eligible for mogamulizumab treatment). Valemetostat was administered under fasted conditions on continuous 28-day cycles until disease progression or unacceptable toxicity. The valemetostat dosage was reduced to 100 mg/day in patients coadministered strong CYP3A or P-gp inhibitors and to 50 mg/day in those coadministered a strong CYP3A and P-gp inhibitor. The threshold ORR was 5%, because no established treatment exists for patients with R/R ATL, and the expected ORR was 30% based primarily on outcomes in a study of lenalidomide in R/R ATL [3].
Valmetostat showed promising clinical activity in the subset of patients with R/R ATL and R/R PTCL in a US and Japanese phase 1 trial in R/R NHL (NCT02732275) [4, 23]. In patients administered valemetostat 200 mg once daily in the dose expansion cohort, the ORR in the R/R ATL subset (n = 14) was 57.1% (8/14 patients) [investigator’s assessment]. CR and PR were both 28.6% (4 of 14 patients each); 14.3% (2/14) of patients had SD and 21.4% (3/14) had PD. The median time to response was 8.14 weeks. After a median 23.07 weeks’ follow up, median DOR and PFS were not estimable in this patient cohort. In the R/R PTCL subset (n = 44), the ORR based on investigator’s assessment was 54.5% (24/44 patients) [investigator’s assessment]. CR and PR were both 27.3% (12 of 44 patients each), 11.4% (5/44) of patients had SD and 18.2% (8/44) had PD. The median time to response was 8.14 weeks. After a median 19.93 weeks’ follow-up, the median DOR was 56.0 weeks and the median PFS was 52.0 weeks. At the time of data cut-off (2 November 2020), 6 patients with R/R ATL and 12 patients with R/R PTCL continued to be treated with valemetostat. [4, 23].
Eligible patients in this multiple ascending dose trial were aged ≥ 18 (USA) or ≥ 20 (Japan) years of age. The dose-escalation cohort were administered valemetostat 150–300 mg once daily and the dose expansion cohort (which was limited to patients with R/R PTCL or R/R ATL) were administered valemetostat 200 mg once daily. Treatment was administered under fasted conditions in continuous 28-day cycles until disease progression or unacceptable toxicity. At baseline, the median age in patients with R/R ATL was 66.5 years and they had received a median of two prior treatments, including HSCT (in 2 of 14 patients). The median age in patients with R/R PTCL was 68.5 years and they had also received a median of two prior treatments, including HSCT (9 of 44 patients) [4, 23].
Key clinical trials of valemetostat
Drug(s) | Indication | Phase | Status | Location(s) | Sponsor/Collaborator | Identifier |
|---|---|---|---|---|---|---|
Valemetostat | R/R ATL | 2 | Ongoing | Japan | Daiichi Sankyo | NCT04102150; JapicCTI-194964 |
Valemetostat | R/R PTCL | 2 | Ongoing | Global | Daiichi Sankyo | NCT04703192; EudraCT2020-004954-31; jRCT2071200095; VALENTINE-PTCL01 |
Valemetostat | R/R NHL (including BCL, ATL and PTCL) | 1 | Ongoing | Japan, USA | Daiichi Sankyo | NCT02732275; JapicCTI-163173 |
Valemetostat | R/R BCL | 2 | Ongoing | Belgium, France | The Lymphoma Academic Research Organisation; Daiichi Sankyo | NCT04842877; EudraCT2020-005225-81; VALYM |
Valemetostat | AML or ALL | 1 | Terminateda | USA | Daiichi Sankyo | NCT03110354 |
Valemetostat, irinotecan | Recurrent SCLC | 1/2 | Ongoing | USA | Memorial Sloan Kettering Cancer Center | NCT03879798 |
Valemetostat, ipilimumab | Metastatic prostate, urothelial, and renal cell cancers | 1 | Ongoing | USA | M.D. Anderson Cancer Center; National Cancer Institute | NCT04388852; NCI-2020-02916 |
Valemetostat | Malignant solid tumoursb | 1 | Ongoing | Japan | National Cancer Center Hospital, Tokyo | jRCT2031190268 NCCH1904/MK007; ELEPHANT |
2.4 Adverse Events
The tolerability and safety profile of valemetostat 200 mg once daily was manageable in clinical trials [3, 4, 10]. Most (96%) patients in the Japanese phase 2 trial in patients with R/R ATL (NCT04102150; n = 25) reported an adverse reaction [10]. The most frequent adverse reactions (any grade) were thrombocytopenia (80%; 20/25 patients), anaemia (44%; 11/25), alopecia (40.0%; 10/25), dysgeusia (36.0%; 9/25), lymphopenia (20%; 5/25), neutropenia (20.0%; 5/25) and leukopenia (20.0%; 5/25) [10]. Serious treatment-emergent adverse events (TEAEs) were reported in 32% (8/25) patients. Of the 20 patients who experienced thrombocytopenia (a prespecified AE of special interest), 3 experienced grade 4 thrombocytopenia (platelet count < 25 × 109/L) and 3 required dose modification (discontinuation, 1 patient; dose interruption, 2 patients). TEAEs led to dose reduction in 2 patients (8%) and dose interruption in 5 patients (20%). Two patients (8%) who had achieved SD discontinued study treatment due to adverse events. No treatment-related deaths occurred [3]. Secondary malignancies, including haematological malignancy, were not reported in this trial. The median dose of valemetostat was 199.33 mg/day and the median duration of treatment was 4.3 months [3].
The most frequent adverse reactions occurring with valemetostat 200 mg once daily in patients with R/R ATL in pooled data from the Japanese phase 2 trial (NCT04102150; n = 25) [3] and the 200 mg once daily cohort in the international phase 1 trial in patients with R/R NHL (NCT02732275; n = 14) [4] were alopecia (40.5%) and dysgeusia (40.5%). Dry skin, rash, nausea, increased ALT and loss of appetite were each reported in 10% to ≈ 20% of patients, and diarrhoea, increased AST and fatigue were each reported in < 10% of patients [10]. Other adverse reactions included thrombocytopenia (73.0%), anaemia (40.5%), neutropenia (27.0%), leukopenia (21.6%), lymphopenia (16.2%) and upper respiratory tract infection (5.4%) [10].
2.5 Ongoing Clinical Trials
In addition to the Japanese phase 2 trial in patients with R/R ATL (NCT04102150) and the Japanese/US phase 1 trial in R/R NHL (NCT02732275) discussed above, several other trials in R/R NHL are ongoing. These include the global phase 2 VALENTINE trial in R/R PTCL (NCT04703192) [24] and the French/Belgian phase 2 VALYM trial in R/R BCL conducted by the LYSARC (NCT04842877). Valemetostat is also being investigated several trials in patients with solid tumours, including a US phase 1 trial of valemetostat in combination with ipilimumab in metastatic prostate, urothelial, and renal cell cancers (NCT04388852), a US phase 1/2 trial of valemetostat in combination with irinotecan in recurrent small cell lung cancer (NCT03879798) and a Japanese phase 1 trial of valemetostat monotherapy in patients aged 3–29 years with solid tumours (jRCT2031190268; ELEPHANT) [25].
3 Current Status
Valemetostat received its first approval on 26 September 2022 for the treatment of R/R ATL in Japan [12].
Change history
28 November 2022
A Correction to this paper has been published: https://doi.org/10.1007/s40265-022-01818-9
References
Bates SE. Epigenetic therapies for cancer. N Engl J Med. 2020;383(7):650–63.
Sun S, Yu F, Xu D, et al. EZH2, a prominent orchestrator of genetic and epigenetic regulation of solid tumor microenvironment and immunotherapy. BBA Rev Cancer. 2022. https://doi.org/10.1016/j.bbcan.2022.188700.
Izutsu K, Makita S, Nosaka K, et al. An open-label, single-arm, phase 2 trial of valemetostat in relapsed or refractory adult T-cell leukemia/lymphoma. Blood. 2022. https://doi.org/10.1182/blood.2022016862.
Kusumoto S, Izutsu K, Maruyama D, et al. First-in-human study of the EZH and EZH2 dual inhibitor valemetostat tosylate (DS-3201B) in patients with relapsed or refractory non-Hodgkin lymphomas [abstract no. S218]. In: 26th Congress of the European Haematology Association. 2021.
Yamagishi M, Hori M, Fujikawa D, et al. Targeting excessive EZH1 and EZH2 activities for abnormal histone methylation and transcription network in malignant lymphomas. Cell Rep. 2019;29(8):2321-37.e7.
Nakagawa M, Kitabayashi I. Oncogenic roles of enhancer of zeste homolog 1/2 in hematological malignancies. Cancer Sci. 2018;109(8):2342–8.
Lymphoma Research Foundation. About lymphoma and subtypes. 2021. https://lymphoma.org/. Accessed 13 Oct 2022.
Zhuang Y, Che J, Wu M, et al. Altered pathways and targeted therapy in double hit lymphoma. J Hematol Oncol. 2022. https://doi.org/10.1186/s13045-022-01249-9.
Cook LB, Fuji S, Hermine O, et al. Revised adult T-cell leukemia-lymphoma International Consensus Meeting report. J Clin Oncol. 2019;37(8):677–87.
Daichii-Sankyo Company Ltd. EZHARMIA® (valemetostat tosilate): Japanese prescribing information. 2022. https://www.pmda.go.jp/PmdaSearch/iyakuSearch/. Accessed 28 Sept 2022.
Daiichi Sankyo Company Ltd. Daiichi Sankyo's EZH1/2 dual inhibitor valemetostat (DS-3201) receives SAKIGAKE designation for treatment of patients with relapsed/refractory peripheral T-cell lymphoma from Japan MHLW [media release]. 9 Apr 2019. http://www.daiichisankyo.com.
Daiichi Sankyo Company Ltd. EZHARMIA® approved in Japan as first dual EZH1 and EZH2 inhibitor therapy for patients with adult T-cell leukemia/lymphoma [media release]. 26 Sep 2022. https://www.daiichisankyo.com/.
Daiichi Sankyo Company Ltd, LYSA-LYSARC-CALYM. Daiichi Sankyo and LYSA-LYSARC-CALYM enter research collaboration for valemetostat in patients with relapsed/refractory B-Cell lymphoma [media release]. 24 Feb 2021. https://daiichisankyo.us/.
Daiichi Sankyo Company Ltd, The University of Texas MD Anderson Cancer Center. MD Anderson and Daiichi Sankyo enter research collaboration to accelerate development of acute myeloid leukemia therapies [media release]. 14 Sep 2017. http://www.daiichisankyo.com.
Honma D, Adachi N, Kanno O, et al. Development and characterization of the novel orally bioavailable EZH1/2 dual inhibitor DS-3201 [abstract no. 2073]. Blood. 2017;130(Suppl 1).
Honma D, Kanno O, Watanabe J, et al. Novel orally bioavailable EZH1/2 dual inhibitors with greater antitumor efficacy than an EZH2 selective inhibitor. Cancer Sci. 2017;108(10):2069–78.
Honma D, Nosaka E, Shiroishi M, et al. DS-3201, a potent EZH1/2 dual inhibitor, demonstrates antitumor activity against non-Hodgkin lymphoma (NHL) regardless of EZH2 mutation [abstract no. 2217]. Blood. 2018;132 (Suppl. 1).
Banjo T, Hama Y, Nosaka E, et al. EZH1/2 dual inhibitor valemetostat tosylate (DS-3201b) acts differently from EZH2 selective inhibitor on epigenetic landscape to exert greater anti-tumor effect against diffuse large B-cell lymphoma [abstract no. 2948]. Blood. 2021;138(Suppl. 1 ).
Fujita S, Honma D, Adachi N, et al. Dual inhibition of EZH1/2 breaks the quiescence of leukemia stem cells in acute myeloid leukemia. Leukemia. 2018;32(4):855–64.
Hama Y, Banjo T, Honma D, et al. Anti-tumor effect of the EZH1/2 dual inhibitor valemetostat against diffuse large B-cell lymphoma via modulation of B-cell receptor signaling and c-Myc signaling pathways [abstract no. 4642]. Blood. 2019;134(Suppl 1).
Yamagishi M, Hori M, Fujikawa D, et al. Development and molecular analysis of synthetic lethality by targeting EZH1 and EZH2 in non-Hodgkin Lymphomas [abstract no. 462]. Blood. 2016;128(22).
Tachibana M, Maekawa Y, Matsuki S, et al. Open-label study to evaluate the effect of itraconazole and fluconazole on the pharmacokinetics of valemetostat tosylate (valemetostat, DS-3201b) in healthy participants [abstract no. P-175]. Clin Pharmacol Ther. 2022;111(Suppl S1):S51-2.
Daiichi Sankyo Company Ltd. Valemetostat data at EHA shows promising durable tumor response in patients with peripheral T-cell lymphoma and adult T-cell leukemia/lymphoma [media release]. 11 Jun 2021. http://www.daiichisankyo.com.
Foss FM, Porcu P, Horwitz SM, et al. A global phase 2 study of valemetostat tosylate (valemetostat) in patients with relapsed or refractory (R/R) peripheral T-cell lymphoma (PTCL), including R/R adult T-cell leukemia/lymphoma (ATL)—Valentine-PTCL01 [abstract no. 2533]. Blood. 2021;138(Suppl. 1).
Arakawa A, Ozawa H, Hirakawa A, et al. Trial in progress: a phase I trial of dual EZH 1/2 inhibitor valemetostat tosylate (DS- 3201b) in pediatric, adolescent, and young adult patients with malignant solid tumors [abstract no. TPS10059]. J Clin Oncol. 2022;40 (16 Suppl).
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Funding
The preparation of this review was not supported by any external funding.
Authorship and Conflict of interest
During the peer review process the manufacturer of the agent under review was offered an opportunity to comment on the article. Changes resulting from any comments received were made by the authors on the basis of scientific completeness and accuracy. Susan J. Keam is a contracted employee of Adis International Ltd/Springer Nature, and declares no relevant conflicts of interest. All authors contributed to the review and are responsible for the article content.
Ethics approval, Consent to participate, Consent to publish, Availability of data and material, Code availability
Not applicable.
Additional information
This profile has been extracted and modified from the AdisInsight database. AdisInsight tracks drug development worldwide through the entire development process, from discovery, through pre-clinical and clinical studies to market launch and beyond.
The original article has been revised due to retrospective open choice order.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License, which permits any non-commercial use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by-nc/4.0/.
About this article

Cite this article
Keam, S.J. Valemetostat Tosilate: First Approval. Drugs 82, 1621–1627 (2022). https://doi.org/10.1007/s40265-022-01800-5
Published:
Issue Date:
DOI: https://doi.org/10.1007/s40265-022-01800-5