

Spatial transcriptomics stratifies psoriatic disease severity by emergent cellular ecosystems
- PMID: 37267384
- PMCID: PMC10502701
- DOI: 10.1126/sciimmunol.abq7991
Spatial transcriptomics stratifies psoriatic disease severity by emergent cellular ecosystems
Abstract
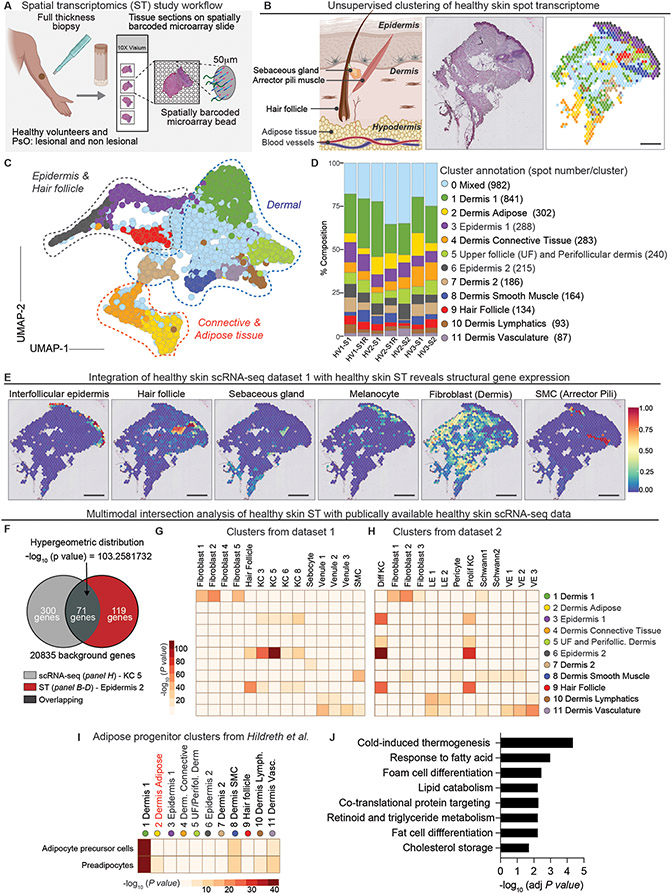
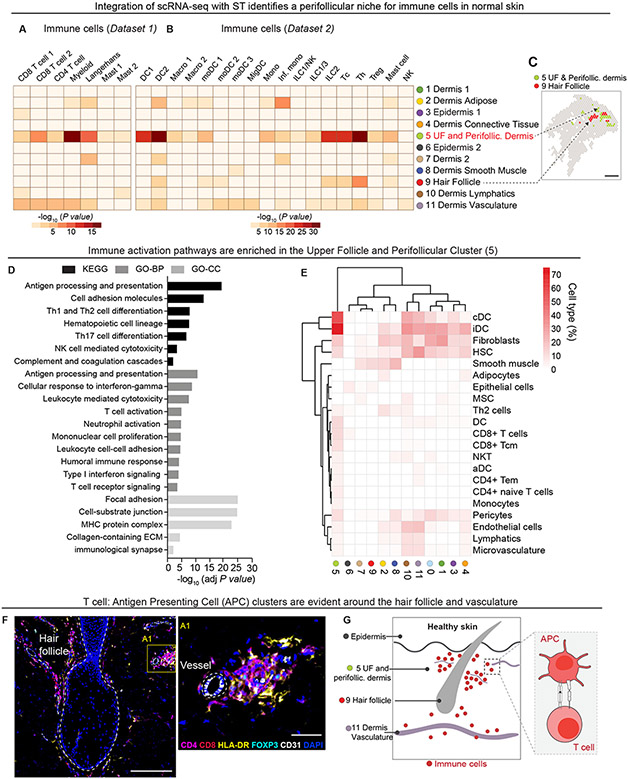
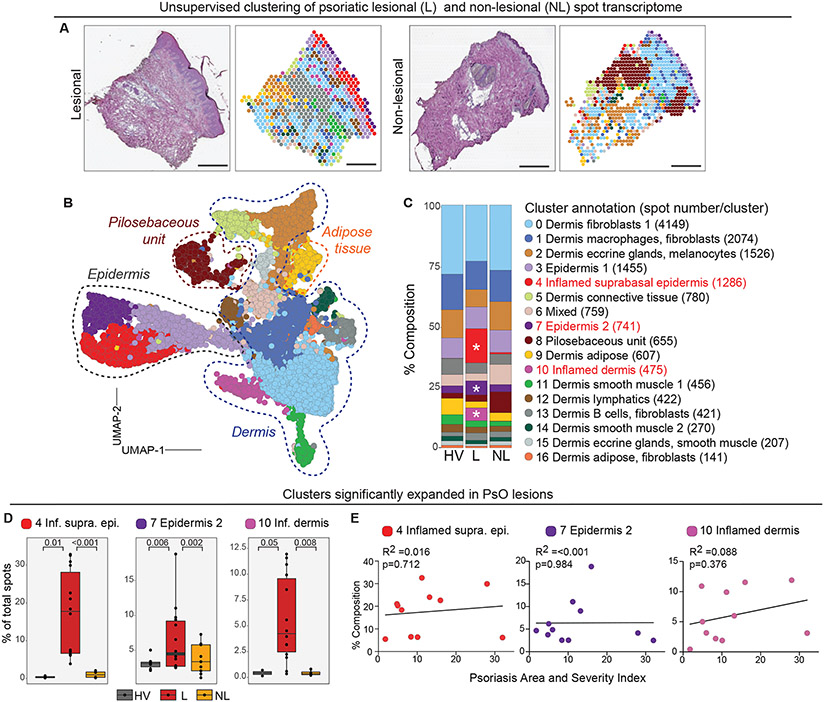
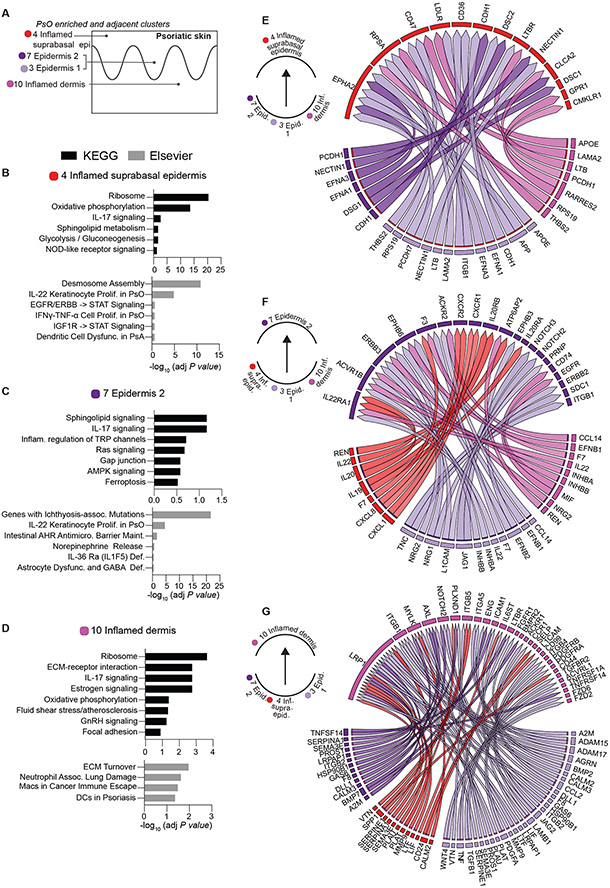
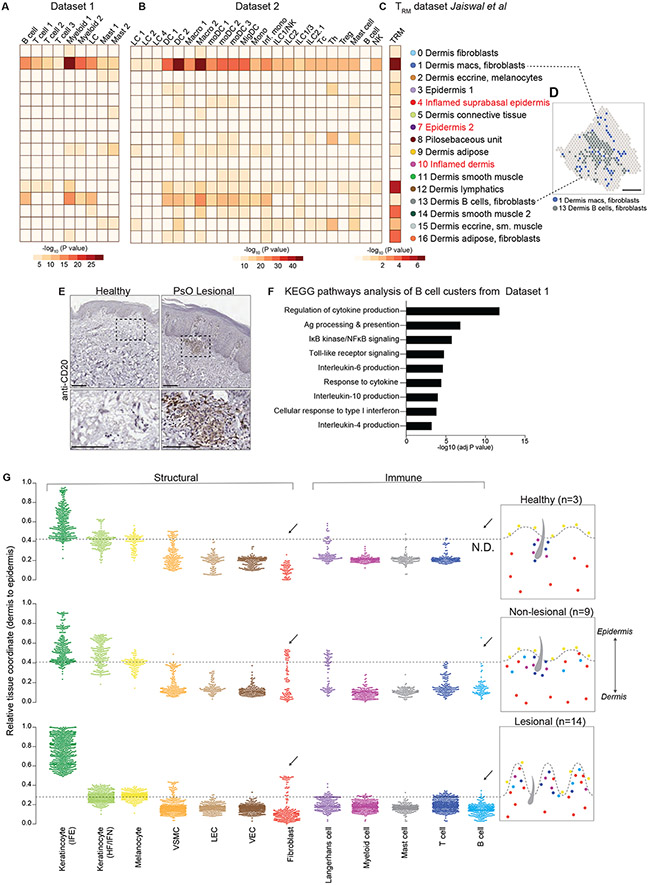
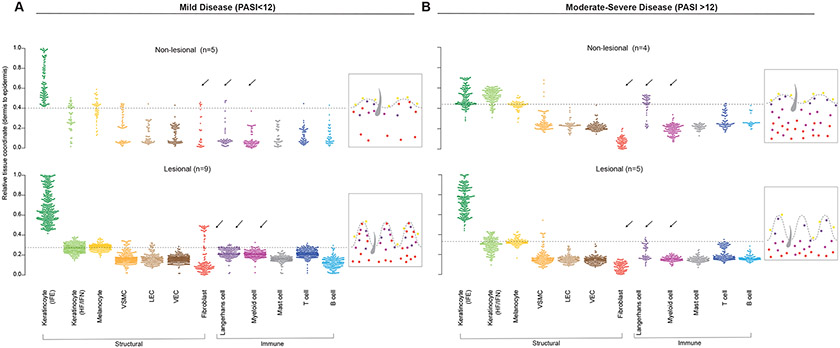
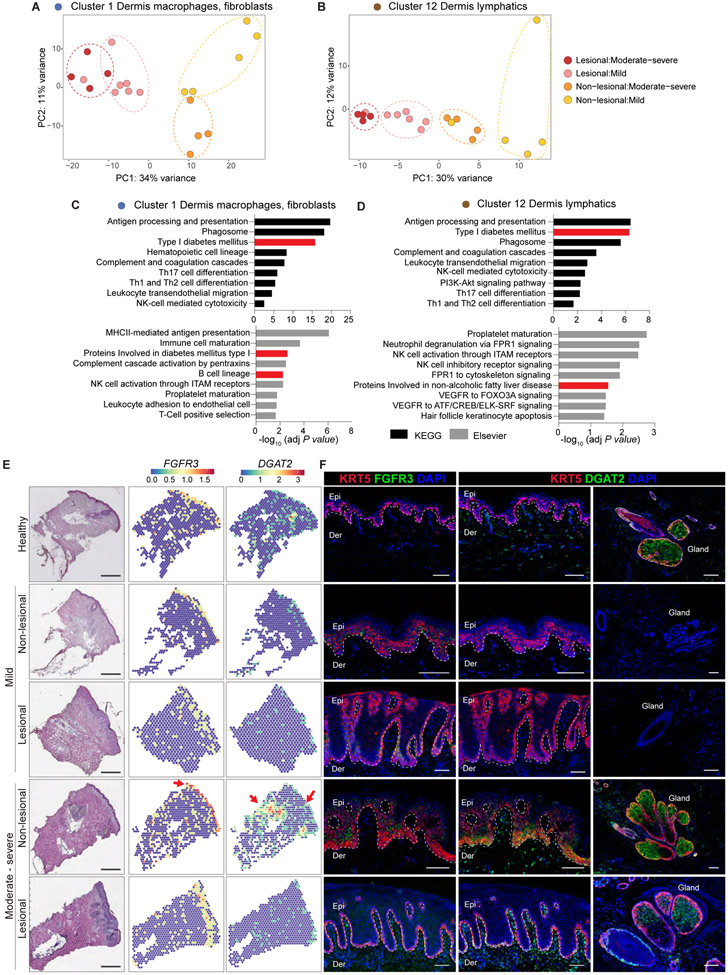
Whereas the cellular and molecular features of human inflammatory skin diseases are well characterized, their tissue context and systemic impact remain poorly understood. We thus profiled human psoriasis (PsO) as a prototypic immune-mediated condition with a high predilection for extracutaneous involvement. Spatial transcriptomics (ST) analyses of 25 healthy, active lesion, and clinically uninvolved skin biopsies and integration with public single-cell transcriptomics data revealed marked differences in immune microniches between healthy and inflamed skin. Tissue-scale cartography further identified core disease features across all active lesions, including the emergence of an inflamed suprabasal epidermal state and the presence of B lymphocytes in lesional skin. Both lesional and distal nonlesional samples were stratified by skin disease severity and not by the presence of systemic disease. This segregation was driven by macrophage-, fibroblast-, and lymphatic-enriched spatial regions with gene signatures associated with metabolic dysfunction. Together, these findings suggest that mild and severe forms of PsO have distinct molecular features and that severe PsO may profoundly alter the cellular and metabolic composition of distal unaffected skin sites. In addition, our study provides a valuable resource for the research community to study spatial gene organization of healthy and inflamed human skin.
Figures

Similar articles
-
Exploratory multi-omics analysis reveals host-microbe interactions associated with disease severity in psoriatic skin.EBioMedicine. 2024 Jul;105:105222. doi: 10.1016/j.ebiom.2024.105222. Epub 2024 Jun 25. EBioMedicine. 2024. PMID: 38924840 Free PMC article.
-
Cutaneous lesions in psoriatic arthritis are enriched in chemokine transcriptomic pathways.Arthritis Res Ther. 2023 May 2;25(1):73. doi: 10.1186/s13075-023-03034-6. Arthritis Res Ther. 2023. PMID: 37131254 Free PMC article.
-
The integration of large-scale public data and network analysis uncovers molecular characteristics of psoriasis.Hum Genomics. 2022 Nov 28;16(1):62. doi: 10.1186/s40246-022-00431-x. Hum Genomics. 2022. PMID: 36437479 Free PMC article.
-
MicroRNA profiling of psoriatic skin identifies 11 miRNAs associated with disease severity.Exp Dermatol. 2022 Apr;31(4):535-547. doi: 10.1111/exd.14497. Epub 2021 Nov 17. Exp Dermatol. 2022. PMID: 34748247 Review.
-
How Can Spatial Transcriptomic Profiling Advance Our Understanding of Skin Diseases?J Invest Dermatol. 2024 Aug 21:S0022-202X(24)01926-2. doi: 10.1016/j.jid.2024.07.006. Online ahead of print. J Invest Dermatol. 2024. PMID: 39177547 Review.
Cited by
-
The Expression of Cytokines and Chemokines Potentially Distinguishes Mild and Severe Psoriatic Non-Lesional and Resolved Skin from Healthy Skin and Indicates Different Stages of Inflammation.Int J Mol Sci. 2024 Oct 20;25(20):11292. doi: 10.3390/ijms252011292. Int J Mol Sci. 2024. PMID: 39457071 Free PMC article.
-
The neuroendocrine transition in prostate cancer is dynamic and dependent on ASCL1.Nat Cancer. 2024 Oct 11. doi: 10.1038/s43018-024-00838-6. Online ahead of print. Nat Cancer. 2024. PMID: 39394434
-
Spatial Transcriptomics Identifies Cellular and Molecular Characteristics of Scleroderma Skin Lesions: Pilot Study in Juvenile Scleroderma.Int J Mol Sci. 2024 Aug 23;25(17):9182. doi: 10.3390/ijms25179182. Int J Mol Sci. 2024. PMID: 39273131 Free PMC article.
-
Recruitment of CXCR4+ type 1 innate lymphoid cells distinguishes sarcoidosis from other skin granulomatous diseases.J Clin Invest. 2024 Sep 3;134(17):e178711. doi: 10.1172/JCI178711. J Clin Invest. 2024. PMID: 39225100 Free PMC article.
-
Single-cell and spatial transcriptomics reveal a high glycolysis B cell and tumor-associated macrophages cluster correlated with poor prognosis and exhausted immune microenvironment in diffuse large B-cell lymphoma.Biomark Res. 2024 Jun 5;12(1):58. doi: 10.1186/s40364-024-00605-w. Biomark Res. 2024. PMID: 38840205 Free PMC article.
References
-
- Kim J et al., The Spectrum of Mild to Severe Psoriasis Vulgaris Is Defined by a Common Activation of IL-17 Pathway Genes, but with Key Differences in Immune Regulatory Genes. Journal of Investigative Dermatology 136, 2173–2182 (2016). - PubMed
-
- Coates LC, FitzGerald O, Helliwell PS, Paul C, Psoriasis, psoriatic arthritis, and rheumatoid arthritis: Is all inflammation the same? Semin Arthritis Rheum 46, 291–304 (2016). - PubMed
-
- Husni ME, Merola JF, Davin S, The psychosocial burden of psoriatic arthritis. Seminars in Arthritis and Rheumatism 47, 351–360 (2017). - PubMed
-
- Husted JA et al., Cardiovascular and other comorbidities in patients with psoriatic arthritis: a comparison with patients with psoriasis. Arthritis Care Res (Hoboken) 63, 1729–1735 (2011). - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
