

Asthma and Chronic Rhinosinusitis: How Similar Are They in Pathogenesis and Treatment Responses?
- PMID: 33805199
- PMCID: PMC8037977
- DOI: 10.3390/ijms22073340
Asthma and Chronic Rhinosinusitis: How Similar Are They in Pathogenesis and Treatment Responses?
Abstract
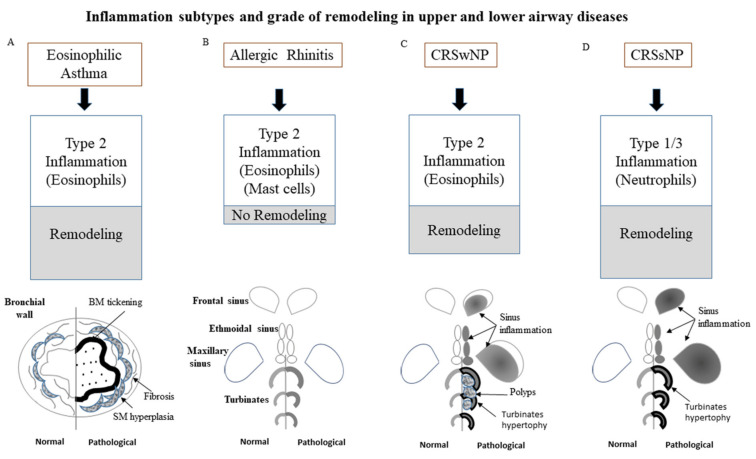
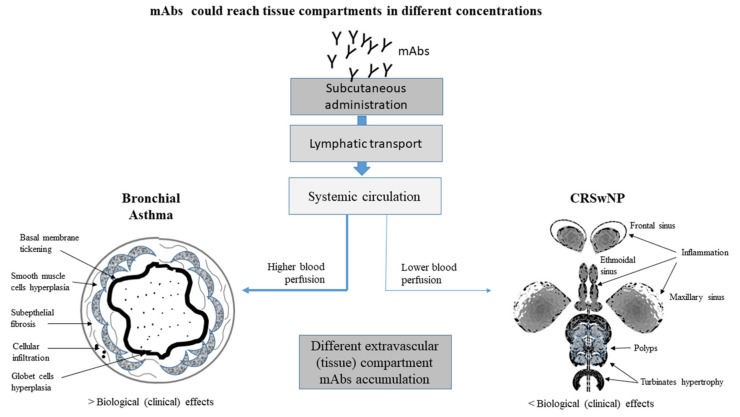
Severe asthma and rhinosinusitis represent frequent comorbidities, complicating the overall management of the disease. Both asthma and chronic rhinosinusitis (CRS) can be differentiated into endotypes: those with type 2 eosinophilic inflammation and those with a non-type 2 inflammation. A correct definition of phenotype/endotype for these diseases is crucial, taking into account the availability of novel biological therapies. Even though patients suffering from type 2 severe asthma-with or without CRS with nasal polyps-significantly benefit from treatment with biologics, the existence of different levels of patient response has been clearly demonstrated. In fact, in clinical practice, it is a common experience that patients reach a good clinical response for asthma symptoms, but not for CRS. At first glance, a reason for this could be that although asthma and CRS can coexist in the same patient, they can manifest with different degrees of severity; therefore, efficacy may not be equally achieved. Many questions regarding responders and nonresponders, predictors of response, and residual disease after blocking type 2 pathways are still unanswered. In this review, we discuss whether treatment with biological agents is equally effective in controlling both asthma and sinonasal symptoms in patients in which asthma and chronic rhinosinusitis with nasal polyps coexist.
Keywords: asthma; biological agents; chronic rhinosinusitis; nasal polyps; type 2 inflammation.
Conflict of interest statement
The authors declare no conflict of interest.
Figures
Similar articles
-
An update on the role of chronic rhinosinusitis with nasal polyps as a co-morbidity in severe asthma.Expert Rev Respir Med. 2020 Dec;14(12):1197-1205. doi: 10.1080/17476348.2020.1812388. Epub 2020 Sep 2. Expert Rev Respir Med. 2020. PMID: 32875924 Review.
-
Managing chronic rhinosinusitis in severe asthma.Curr Opin Pulm Med. 2021 Jan;27(1):23-28. doi: 10.1097/MCP.0000000000000741. Curr Opin Pulm Med. 2021. PMID: 33105235 Review.
-
Consultation for Chronic Rhinosinusitis With Nasal Polyps and Asthma: Clinical Presentation, Diagnostic Workup, and Treatment Options.J Allergy Clin Immunol Pract. 2024 Nov;12(11):2898-2905. doi: 10.1016/j.jaip.2024.07.019. Epub 2024 Jul 30. J Allergy Clin Immunol Pract. 2024. PMID: 39089438 Review.
-
Diverse Endotypes of Chronic Rhinosinusitis and Clinical Implications.Clin Rev Allergy Immunol. 2023 Dec;65(3):420-432. doi: 10.1007/s12016-023-08976-y. Epub 2024 Jan 4. Clin Rev Allergy Immunol. 2023. PMID: 38175322 Review.
-
[Clinical treatment options oriented to the endotype of chronic rhinosinusitis].Lin Chuang Er Bi Yan Hou Tou Jing Wai Ke Za Zhi. 2023 Nov;37(11):902-908. doi: 10.13201/j.issn.2096-7993.2023.11.009. Lin Chuang Er Bi Yan Hou Tou Jing Wai Ke Za Zhi. 2023. PMID: 37905485 Free PMC article. Chinese.
Cited by
-
Do Comorbidities Influence the Response to Biologics in Severe Asthma?Am J Respir Crit Care Med. 2024 Feb 1;209(3):233-235. doi: 10.1164/rccm.202311-2103ED. Am J Respir Crit Care Med. 2024. PMID: 38064716 Free PMC article. No abstract available.
-
Diagnostic biomarkers for chronic rhinosinusitis in adult asthmatics in real-world practice.World Allergy Organ J. 2024 Feb 15;17(3):100879. doi: 10.1016/j.waojou.2024.100879. eCollection 2024 Mar. World Allergy Organ J. 2024. PMID: 38380106 Free PMC article.
-
How the Immune System Responds to Allergy Immunotherapy.Biomedicines. 2022 Nov 5;10(11):2825. doi: 10.3390/biomedicines10112825. Biomedicines. 2022. PMID: 36359345 Free PMC article. Review.
-
Exploring the immunopathology of type 2 inflammatory airway diseases.Front Immunol. 2024 Apr 12;15:1285598. doi: 10.3389/fimmu.2024.1285598. eCollection 2024. Front Immunol. 2024. PMID: 38680486 Free PMC article. Review.
-
Induction of a type 2 inflammatory chronic rhinosinusitis in C57BL/6 mice.Asia Pac Allergy. 2023 Dec;13(4):164-174. doi: 10.5415/apallergy.0000000000000123. Epub 2023 Nov 2. Asia Pac Allergy. 2023. PMID: 38094094 Free PMC article.
References
-
- Siddiqui S., Shikotra A., Richardson M., Doran E., Choy D., Bell A., Austin C.D., Eastham-Anderson J., Hargadon B., Arron J.R., et al. Airway pathological heterogeneity in asthma: Visualization of disease microclusters using topological data analysis. J. Allergy Clin. Immunol. 2018;142:1457–1468. doi: 10.1016/j.jaci.2017.12.982. - DOI - PubMed
-
- Wenzel S.E., Schwartz L.B., Langmack E.L., Halliday J.L., Trudeau J.B., Gibbs R.L., Chu H.W. Evidence That Severe Asthma Can be Divided Pathologically into Two Inflammatory Subtypes with Distinct Physiologic and Clinical Characteristics. Am. J. Respir. Crit. Care Med. 1999;160:1001–1008. doi: 10.1164/ajrccm.160.3.9812110. - DOI - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
