

Use of endotypes, phenotypes, and inflammatory markers to guide treatment decisions in chronic rhinosinusitis
- PMID: 32007571
- PMCID: PMC7192133
- DOI: 10.1016/j.anai.2020.01.013
Use of endotypes, phenotypes, and inflammatory markers to guide treatment decisions in chronic rhinosinusitis
Abstract
Objective: With the advent of new treatment options for Chronic Rhinosinusitis (CRS) comes the ability for physicians to provide more individualized patient care. Physicians are now tasked with identifying who may be the best candidate for a particular therapy. In this review, existing biomarkers and potentially new methods that could guide treatment choices in CRS patients will be discussed.
Data sources: Published literature obtained through PubMed searches.
Study selection: Studies relevant to inflammatory endotypes, phenotypes, and biomarkers in CRS were included.
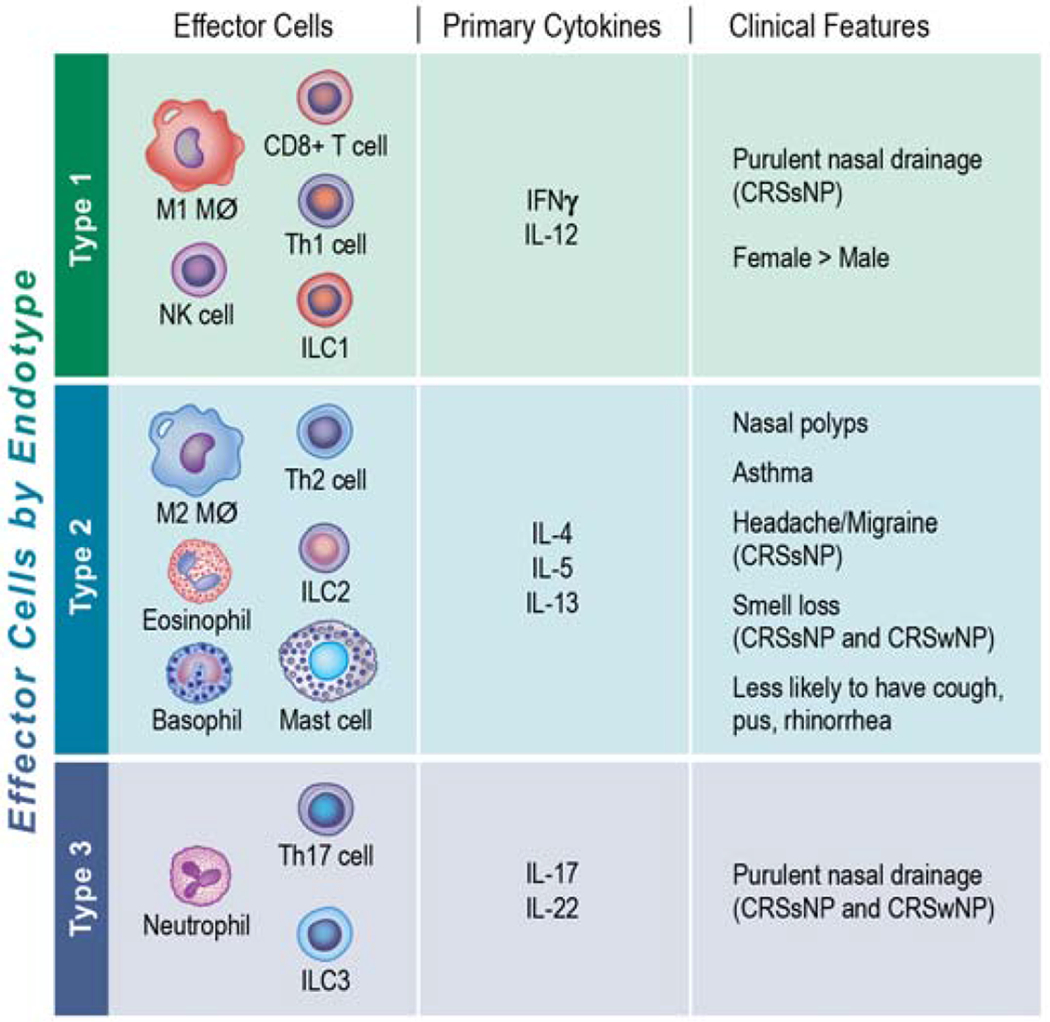
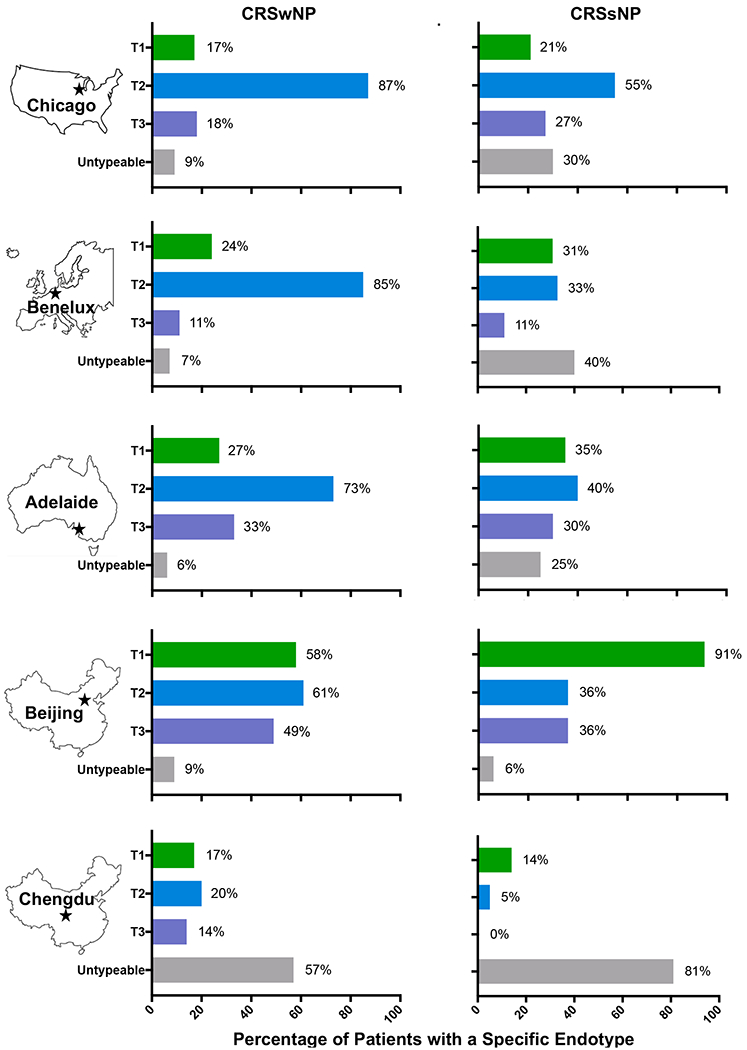
Results: Currently, there are no clinically validated tools that determine the best therapeutic modality for CRS patients with or without nasal polyps (CRSwNP or CRSsNP). Patients with CRS can be classified into three endotypes based on the presence of type 1, type 2, or type 3 inflammation. CRS endotypes can be influenced by age and geographic location. Clinical application however may be limited since endotyping current requires basic research laboratory support. Clinical symptoms may also predict inflammatory endotypes with smell loss being indicative of type 2 inflammation. Numbers of tissue and/or peripheral eosinophils as well as levels of IgE may predict disease severity in CRSwNP but not necessarily treatment responses. Unique clinical phenotypes or biomarkers are especially lacking that predict type 1 or type 3 inflammation in CRSwNP or type 1, type 2, or type 3 inflammation in CRSsNP.
Conclusion: While significant progress has been made in characterizing endotypes, phenotypes, and biomarkers in CRS, additional studies are needed to determine if and how these factors could assist physicians in providing more individualized clinical care.
Copyright © 2020 American College of Allergy, Asthma & Immunology. Published by Elsevier Inc. All rights reserved.
Figures
Similar articles
-
Inflammatory endotypes of chronic rhinosinusitis based on cluster analysis of biomarkers.J Allergy Clin Immunol. 2016 May;137(5):1449-1456.e4. doi: 10.1016/j.jaci.2015.12.1324. Epub 2016 Mar 4. J Allergy Clin Immunol. 2016. PMID: 26949058
-
Associations Between Inflammatory Endotypes and Clinical Presentations in Chronic Rhinosinusitis.J Allergy Clin Immunol Pract. 2019 Nov-Dec;7(8):2812-2820.e3. doi: 10.1016/j.jaip.2019.05.009. Epub 2019 May 22. J Allergy Clin Immunol Pract. 2019. PMID: 31128376 Free PMC article.
-
Chronic Rhinosinusitis-Could Phenotyping or Endotyping Aid Therapy?Am J Rhinol Allergy. 2019 Jan;33(1):83-93. doi: 10.1177/1945892418807590. Epub 2018 Oct 24. Am J Rhinol Allergy. 2019. PMID: 30353741 Review.
-
Diverse Endotypes of Chronic Rhinosinusitis and Clinical Implications.Clin Rev Allergy Immunol. 2023 Dec;65(3):420-432. doi: 10.1007/s12016-023-08976-y. Epub 2024 Jan 4. Clin Rev Allergy Immunol. 2023. PMID: 38175322 Review.
-
Mechanisms and biomarkers of inflammatory endotypes in chronic rhinosinusitis without nasal polyps.J Allergy Clin Immunol. 2021 Apr;147(4):1306-1317. doi: 10.1016/j.jaci.2020.11.037. Epub 2020 Dec 14. J Allergy Clin Immunol. 2021. PMID: 33326802 Free PMC article.
Cited by
-
Particulate matter exposure is associated with increased inflammatory cytokines and eosinophils in chronic rhinosinusitis.Allergy. 2024 May;79(5):1219-1229. doi: 10.1111/all.16006. Epub 2024 Jan 5. Allergy. 2024. PMID: 38180309
-
Significance of leukocyte-specific transcript 1 levels in nasal mucosal tissue to predict recurrence of nasal polyps.Braz J Otorhinolaryngol. 2023 Mar-Apr;89(2):321-328. doi: 10.1016/j.bjorl.2022.11.004. Epub 2022 Dec 12. Braz J Otorhinolaryngol. 2023. PMID: 36754676 Free PMC article.
-
The Role of Proprotein Convertases in Upper Airway Remodeling.Mol Cells. 2022 Jun 30;45(6):353-361. doi: 10.14348/molcells.2022.0019. Mol Cells. 2022. PMID: 35611689 Free PMC article. Review.
-
The interplay of inflammation and remodeling in the pathogenesis of chronic rhinosinusitis: current understanding and future directions.Front Immunol. 2023 Sep 12;14:1238673. doi: 10.3389/fimmu.2023.1238673. eCollection 2023. Front Immunol. 2023. PMID: 37771597 Free PMC article. Review.
-
Stratified approaches for using biomarkers in phenotyping for the management of severe asthma in India.Lung India. 2022 Jan-Feb;39(1):65-69. doi: 10.4103/lungindia.lungindia_129_21. Lung India. 2022. PMID: 34975055 Free PMC article. Review.
References
-
- Dietz de Loos D, Lourijsen ES, Wildeman MAM, Freling NJM, Wolvers MDJ, Reitsma S, et al. Prevalence of chronic rhinosinusitis in the general population based on sinus radiology and symptomatology. J Allergy Clin Immunol 2019; 143:1207–14. - PubMed
-
- Fokkens WJ, Lund VJ, Mullol J, Bachert C, Alobid I, Baroody F, et al. European Position Paper on Rhinosinusitis and Nasal Polyps 2012. Rhinol Suppl 2012; 23:3 p preceding table of contents, 1-298. - PubMed
-
- Rudmik L Economics of Chronic Rhinosinusitis. Curr Allergy Asthma Rep 2017; 17:20. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
