

Cellular and Molecular Mechanisms Underlying Prostate Cancer Development: Therapeutic Implications
- PMID: 31366128
- PMCID: PMC6789661
- DOI: 10.3390/medicines6030082
Cellular and Molecular Mechanisms Underlying Prostate Cancer Development: Therapeutic Implications
Abstract
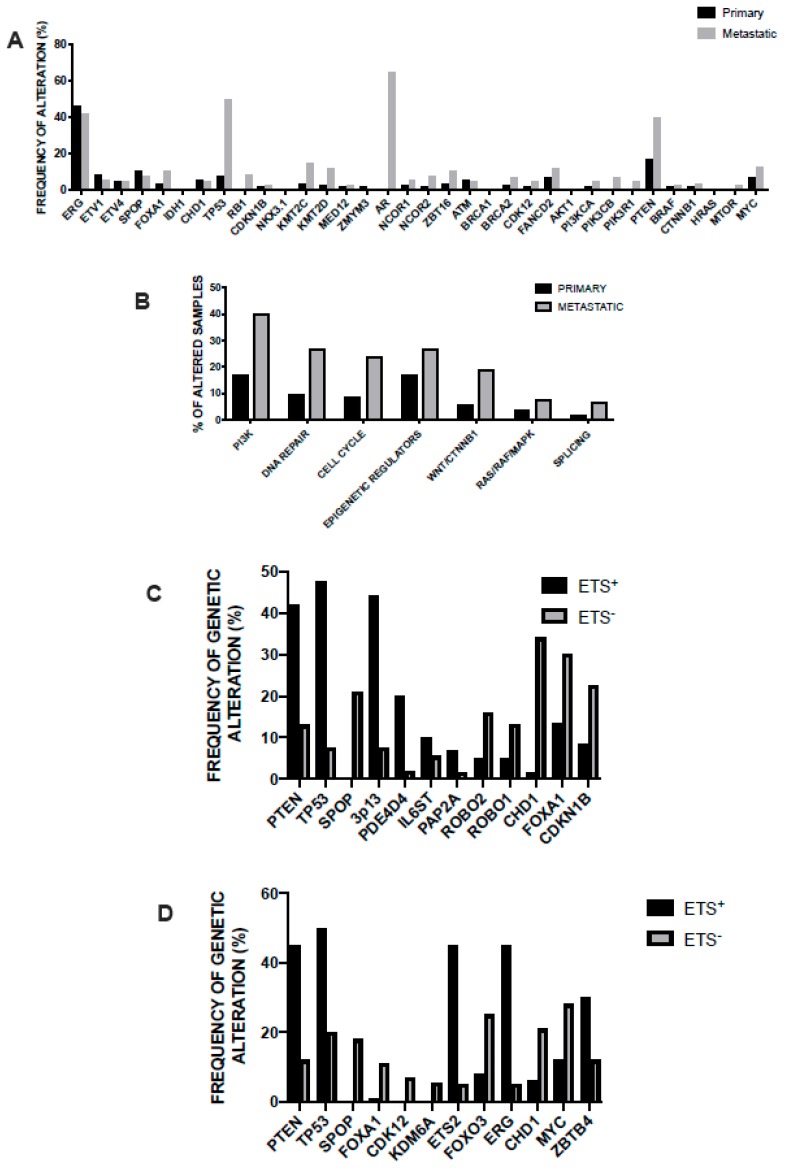
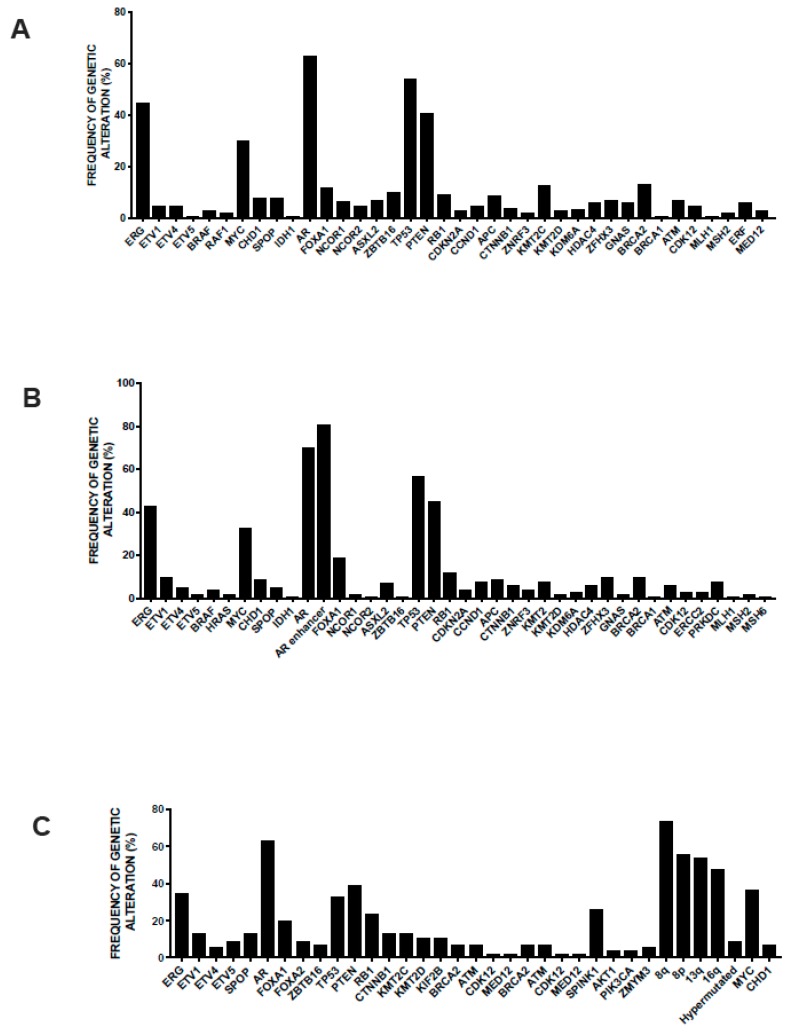
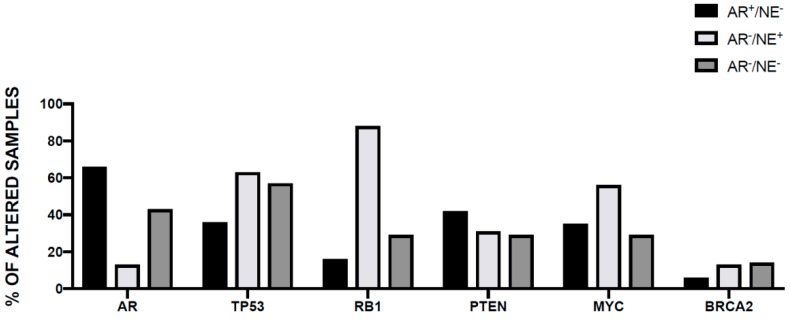
Prostate cancer is the most frequent nonskin cancer and second most common cause of cancer-related deaths in man. Prostate cancer is a clinically heterogeneous disease with many patients exhibiting an aggressive disease with progression, metastasis, and other patients showing an indolent disease with low tendency to progression. Three stages of development of human prostate tumors have been identified: intraepithelial neoplasia, adenocarcinoma androgen-dependent, and adenocarcinoma androgen-independent or castration-resistant. Advances in molecular technologies have provided a very rapid progress in our understanding of the genomic events responsible for the initial development and progression of prostate cancer. These studies have shown that prostate cancer genome displays a relatively low mutation rate compared with other cancers and few chromosomal loss or gains. The ensemble of these molecular studies has led to suggest the existence of two main molecular groups of prostate cancers: one characterized by the presence of ERG rearrangements (~50% of prostate cancers harbor recurrent gene fusions involving ETS transcription factors, fusing the 5' untranslated region of the androgen-regulated gene TMPRSS2 to nearly the coding sequence of the ETS family transcription factor ERG) and features of chemoplexy (complex gene rearrangements developing from a coordinated and simultaneous molecular event), and a second one characterized by the absence of ERG rearrangements and by the frequent mutations in the E3 ubiquitin ligase adapter SPOP and/or deletion of CDH1, a chromatin remodeling factor, and interchromosomal rearrangements and SPOP mutations are early events during prostate cancer development. During disease progression, genomic and epigenomic abnormalities accrued and converged on prostate cancer pathways, leading to a highly heterogeneous transcriptomic landscape, characterized by a hyperactive androgen receptor signaling axis.
Keywords: cancer stem cells; gene expression profiling; gene sequencing; prostate cancer; tumor xenotrasplantation assay.
Conflict of interest statement
The author declares no conflicts of interest.
Figures
Similar articles
-
Characterization of TMPRSS2-ETS gene aberrations in androgen-independent metastatic prostate cancer.Cancer Res. 2008 May 15;68(10):3584-90. doi: 10.1158/0008-5472.CAN-07-6154. Cancer Res. 2008. PMID: 18483239 Free PMC article.
-
TMPRSS2- driven ERG expression in vivo increases self-renewal and maintains expression in a castration resistant subpopulation.PLoS One. 2012;7(7):e41668. doi: 10.1371/journal.pone.0041668. Epub 2012 Jul 30. PLoS One. 2012. PMID: 22860005 Free PMC article.
-
Comprehensive assessment of TMPRSS2 and ETS family gene aberrations in clinically localized prostate cancer.Mod Pathol. 2007 May;20(5):538-44. doi: 10.1038/modpathol.3800769. Epub 2007 Mar 2. Mod Pathol. 2007. PMID: 17334343
-
Recent advances in prostate cancer research: large-scale genomic analyses reveal novel driver mutations and DNA repair defects.F1000Res. 2018 Aug 2;7:F1000 Faculty Rev-1173. doi: 10.12688/f1000research.14499.1. eCollection 2018. F1000Res. 2018. PMID: 30135717 Free PMC article. Review.
-
Recurrent gene fusions in prostate cancer: their clinical implications and uses.Curr Urol Rep. 2013 Jun;14(3):214-22. doi: 10.1007/s11934-013-0321-1. Curr Urol Rep. 2013. PMID: 23625457 Review.
Cited by
-
Design and Evaluation of 223Ra-Labeled and Anti-PSMA Targeted NaA Nanozeolites for Prostate Cancer Therapy-Part I.Materials (Basel). 2020 Sep 2;13(17):3875. doi: 10.3390/ma13173875. Materials (Basel). 2020. PMID: 32887308 Free PMC article.
-
Multidrug Resistance of Cancer Cells and the Vital Role of P-Glycoprotein.Life (Basel). 2022 Jun 15;12(6):897. doi: 10.3390/life12060897. Life (Basel). 2022. PMID: 35743927 Free PMC article. Review.
-
Clinical values of expression signature of circCDR1AS and circHIAT1 in prostate cancer: Two circRNAs with regulatory function in androgen receptor (AR) and PI3K/AKT signaling pathways.J Clin Lab Anal. 2022 Feb;36(2):e24220. doi: 10.1002/jcla.24220. Epub 2022 Jan 10. J Clin Lab Anal. 2022. PMID: 35007362 Free PMC article.
-
BRCA Mutations in Ovarian and Prostate Cancer: Bench to Bedside.Cancers (Basel). 2022 Aug 11;14(16):3888. doi: 10.3390/cancers14163888. Cancers (Basel). 2022. PMID: 36010882 Free PMC article. Review.
-
Prostate cancer racial, socioeconomic, geographic disparities: targeting the genomic landscape and splicing events in search for diagnostic, prognostic and therapeutic targets.Am J Cancer Res. 2021 Apr 15;11(4):1012-1030. eCollection 2021. Am J Cancer Res. 2021. PMID: 33948343 Free PMC article. Review.
References
-
- Mellinger G.T. Prognosis of prostatic carcinoma. Recent Results Cancer Res. 1977;60:61–72. - PubMed
-
- Bailar J.C., Mellinger G.T., Gleason D.F. Survival rates of patients with prostatic cancer, tumor stage, and differentiation-preliminary report. Cancer Chemother. Rep. 1966;50:129–136. - PubMed
-
- Gleason D.F. Histological grading and staging of prostatic carcinoma. In: Tannenbaum M., editor. Urologic Pathology: The Prostate. Lea and Feibiger; Philadelphia, PA, USA: 1977. p. 171.
-
- Epstein J.I., Zelefsky M.J., Sjoberg D.D., Nelson J.B., Egevad L., Magi-Galluzzi C., Vickers A.J., Parwani A.V., Reuter V.E., Fine S.W., et al. A contemporary prostate cancer grading system: A validated alternative to the Gleason score. Eur. Urol. 2016;69:428–435. doi: 10.1016/j.eururo.2015.06.046. - DOI - PMC - PubMed
Publication types
LinkOut - more resources
Full Text Sources
Other Literature Sources
Miscellaneous
