

Glial activation and inflammation along the Alzheimer's disease continuum
- PMID: 30791945
- PMCID: PMC6383268
- DOI: 10.1186/s12974-019-1399-2
Glial activation and inflammation along the Alzheimer's disease continuum
Abstract
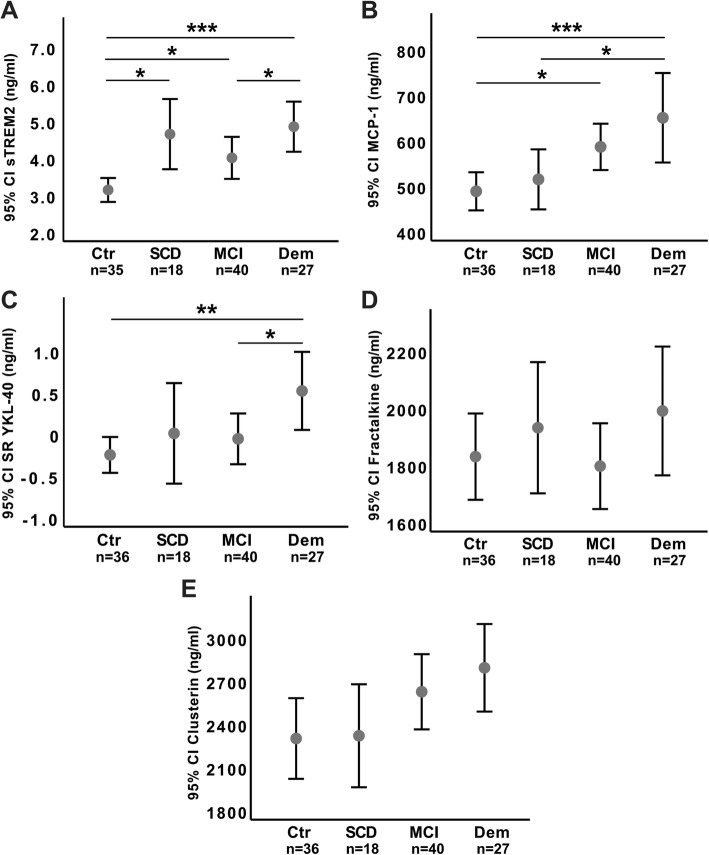
Background: Neuronal and glial cell interaction is essential for synaptic homeostasis and may be affected in Alzheimer's disease (AD). We measured cerebrospinal fluid (CSF) neuronal and glia markers along the AD continuum, to reveal putative protective or harmful stage-dependent patterns of activation.
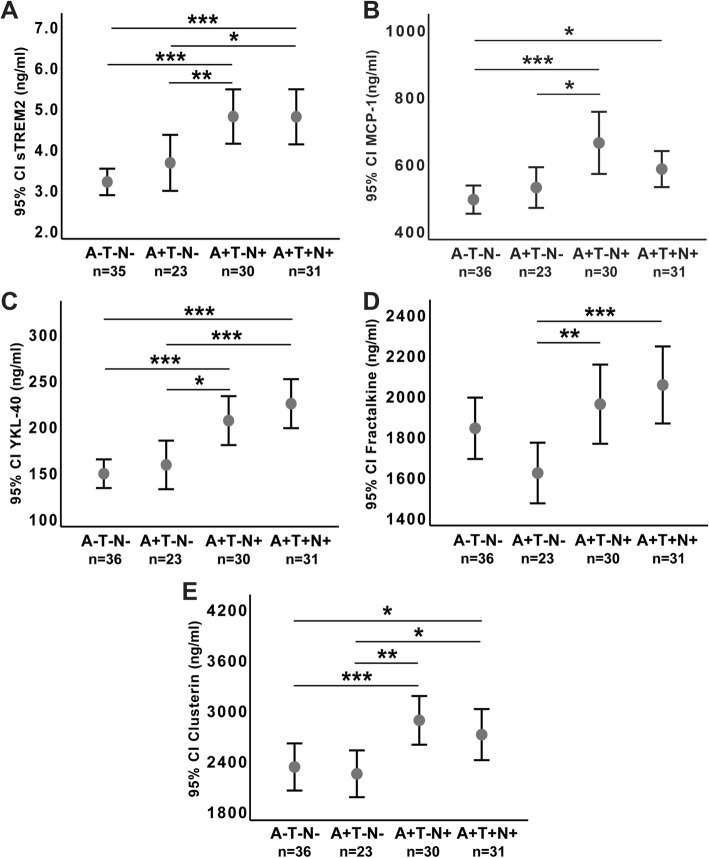
Methods: We included healthy controls (n = 36) and Aβ-positive (Aβ+) cases (as defined by pathological CSF amyloid beta 1-42 (Aβ42)) with either subjective cognitive decline (SCD, n = 19), mild cognitive impairment (MCI, n = 39), or AD dementia (n = 27). The following CSF markers were measured: a microglial activation marker-soluble triggering receptor expressed on myeloid cells 2 (sTREM2), a marker of microglial inflammatory reaction-monocyte chemoattractant protein-1 (MCP-1), two astroglial activation markers-chitinase-3-like protein 1 (YKL-40) and clusterin, a neuron-microglia communication marker-fractalkine, and the CSF AD biomarkers (Aβ42, phosphorylated tau (P-tau), total tau (T-tau)). Using ANOVA with planned comparisons, or Kruskal-Wallis tests with Dunn's pairwise comparisons, CSF levels were compared between clinical groups and between stages of biomarker severity using CSF biomarkers for classification based on amyloid pathology (A), tau pathology (T), and neurodegeneration (N) giving rise to the A/T/N score.
Results: Compared to healthy controls, sTREM2 was increased in SCD (p < .01), MCI (p < .05), and AD dementia cases (p < .001) and increased in AD dementia compared to MCI cases (p < .05). MCP-1 was increased in MCI (p < .05) and AD dementia compared to both healthy controls (p < .001) and SCD cases (p < .01). YKL-40 was increased in dementia compared to healthy controls (p < .01) and MCI (p < .05). All of the CSF activation markers were increased in subjects with pathological CSF T-tau (A+T-N+ and A+T+N+), compared to subjects without neurodegeneration (A-T-N- and A+T-N-).
Discussion: Microglial activation as indicated by increased sTREM2 is present already at the preclinical SCD stage; increased MCP-1 and astroglial activation markers (YKL-40 and clusterin) were noted only at the MCI and AD dementia stages, respectively, and in Aβ+ cases (A+) with pathological T-tau (N+). Possible different effects of early and later glial activation need to be explored.
Keywords: Apolipoprotein J; CX3CL1; Cerebrospinal fluid; Chitinase-3-like protein 1; Clusterin; ELISA; Early diagnosis; Fractalkine; MCP-1; Microglia; Monocyte chemoattractant protein-1; Neuroinflammation; YKL-40; sTREM2.
Conflict of interest statement
Ethics approval and consent to participate
The project has been considered by the Norwegian Regional Ethics Committee (approval number for the DDI project: 2013/115, approval number for the genetic analysis (APGEM): 2014/1164, approval number for the biobank: 2011/1051). The local data protection officer at Akershus University Hospital has also approved the study with the according approval number 13-056, 14-156 and 13-088. Data handling was in accordance with local and national regulations, with security precautions for storage and regulated biobank facilities. Both sexes are equally included, patients and controls give informed consent to participate in the study. The DDI has a patient and caregiver representative in the steering group. User participation is ensured with open meetings and written information.
Consent for publication
Not applicable.
Competing interests
Dr. Aarsland has received research support and/or honoraria from Astra-Zeneca, H. Lundbeck, Novartis Pharmaceuticals, and GE Health and serves as paid consultant for H. Lundbeck, Eisai, Heptares, and Axovant. Dag Aarsland is a Royal Society Wolfson Research Merit Award Holder and would like to thank the Wolfson Foundation and the Royal Society for their support. Dr. Fladby is inventor and co-founder of Inventor Pre Diagnostics A/S. All other authors declare that they have no competing interests.
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Figures
Similar articles
-
Longitudinal cerebrospinal fluid measurements show glial hypo- and hyperactivation in predementia Alzheimer's disease.J Neuroinflammation. 2023 Dec 13;20(1):298. doi: 10.1186/s12974-023-02973-w. J Neuroinflammation. 2023. PMID: 38093257 Free PMC article.
-
Different pattern of CSF glial markers between dementia with Lewy bodies and Alzheimer's disease.Sci Rep. 2019 May 24;9(1):7803. doi: 10.1038/s41598-019-44173-8. Sci Rep. 2019. PMID: 31127154 Free PMC article.
-
CSF YKL-40 and pTau181 are related to different cerebral morphometric patterns in early AD.Neurobiol Aging. 2016 Feb;38:47-55. doi: 10.1016/j.neurobiolaging.2015.10.022. Epub 2015 Nov 2. Neurobiol Aging. 2016. PMID: 26827642
-
Diagnostic function of the neuroinflammatory biomarker YKL-40 in Alzheimer's disease and other neurodegenerative diseases.Expert Rev Proteomics. 2017 Apr;14(4):285-299. doi: 10.1080/14789450.2017.1304217. Epub 2017 Mar 20. Expert Rev Proteomics. 2017. PMID: 28281838 Review.
-
CSF and blood biomarkers for the diagnosis of Alzheimer's disease: a systematic review and meta-analysis.Lancet Neurol. 2016 Jun;15(7):673-684. doi: 10.1016/S1474-4422(16)00070-3. Epub 2016 Apr 8. Lancet Neurol. 2016. PMID: 27068280 Review.
Cited by
-
Sirtuins promote brain homeostasis, preventing Alzheimer's disease through targeting neuroinflammation.Front Physiol. 2022 Aug 15;13:962769. doi: 10.3389/fphys.2022.962769. eCollection 2022. Front Physiol. 2022. PMID: 36045741 Free PMC article. Review.
-
Greater Diffusion Restriction in White Matter in Preclinical Alzheimer Disease.Ann Neurol. 2022 Jun;91(6):864-877. doi: 10.1002/ana.26353. Epub 2022 Mar 30. Ann Neurol. 2022. PMID: 35285067 Free PMC article.
-
Changes in glial cell phenotypes precede overt neurofibrillary tangle formation, correlate with markers of cortical cell damage, and predict cognitive status of individuals at Braak III-IV stages.Acta Neuropathol Commun. 2022 May 9;10(1):72. doi: 10.1186/s40478-022-01370-3. Acta Neuropathol Commun. 2022. PMID: 35534858 Free PMC article.
-
Prognostic prediction of subjective cognitive decline in major depressive disorder based on immune biomarkers: a prospective observational study.BMC Psychiatry. 2023 Jan 19;23(1):54. doi: 10.1186/s12888-022-04513-x. BMC Psychiatry. 2023. PMID: 36658505 Free PMC article.
-
"Amyloid-beta accumulation cycle" as a prevention and/or therapy target for Alzheimer's disease.Aging Cell. 2020 Mar;19(3):e13109. doi: 10.1111/acel.13109. Epub 2020 Jan 25. Aging Cell. 2020. PMID: 31981470 Free PMC article. Review.
References
-
- Jessen F, Amariglio RE, van Boxtel M, Breteler M, Ceccaldi M, Chetelat G, et al. A conceptual framework for research on subjective cognitive decline in preclinical Alzheimer's disease. Alzheimer's & dementia : the journal of the Alzheimer's Association. 2014;10(6):844–852. doi: 10.1016/j.jalz.2014.01.001. - DOI - PMC - PubMed
-
- Albert MS, DeKosky ST, Dickson D, Dubois B, Feldman HH, Fox NC, et al. The diagnosis of mild cognitive impairment due to Alzheimer's disease: recommendations from the National Institute on Aging-Alzheimer's Association workgroups on diagnostic guidelines for Alzheimer's disease. Alzheimer's & dementia : the journal of the Alzheimer's Association. 2011;7(3):270–279. doi: 10.1016/j.jalz.2011.03.008. - DOI - PMC - PubMed
-
- Sperling RA, Aisen PS, Beckett LA, Bennett DA, Craft S, Fagan AM, et al. Toward defining the preclinical stages of Alzheimer's disease: recommendations from the National Institute on Aging-Alzheimer's Association workgroups on diagnostic guidelines for Alzheimer's disease. Alzheimer's & Dementia : the journal of the Alzheimer's Association. 2011;7(3):280–292. doi: 10.1016/j.jalz.2011.03.003. - DOI - PMC - PubMed
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
Miscellaneous
