

Combined Ex Vivo Hypothermic and Normothermic Perfusion for Assessment of High-risk Deceased Donor Human Kidneys for Transplantation
- PMID: 29952816
- PMCID: PMC6365241
- DOI: 10.1097/TP.0000000000002299
Combined Ex Vivo Hypothermic and Normothermic Perfusion for Assessment of High-risk Deceased Donor Human Kidneys for Transplantation
Abstract
Background: Despite careful clinical examination, procurement biopsy and assessment on hypothermic machine perfusion, a significant number of potentially useable deceased donor kidneys will be discarded because they are deemed unsuitable for transplantation. Ex vivo normothermic perfusion (EVNP) may be useful as a means to further assess high-risk kidneys to determine suitability for transplantation.
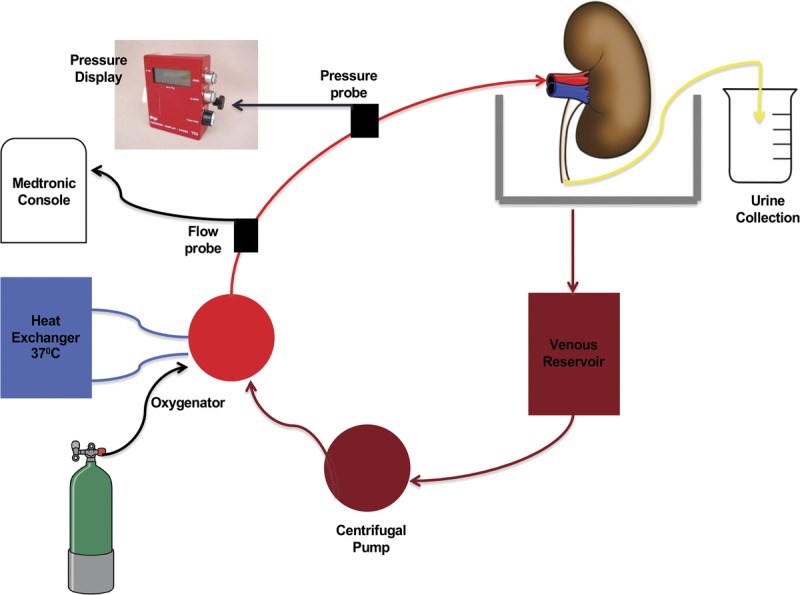
Methods: From June 2014 to October 2015, 7 kidneys (mean donor age, 54.3 years and Kidney Donor Profile Index, 79%) that were initially procured with the intention to transplant were discarded based on a combination of clinical findings, suboptimal biopsies, long cold ischemia time (CIT) and/or poor hypothermic perfusion parameters. They were subsequently placed on EVNP using oxygenated packed red blood cells and supplemental nutrition for a period of 3 hours. Continuous hemodynamic and functional parameters were assessed.
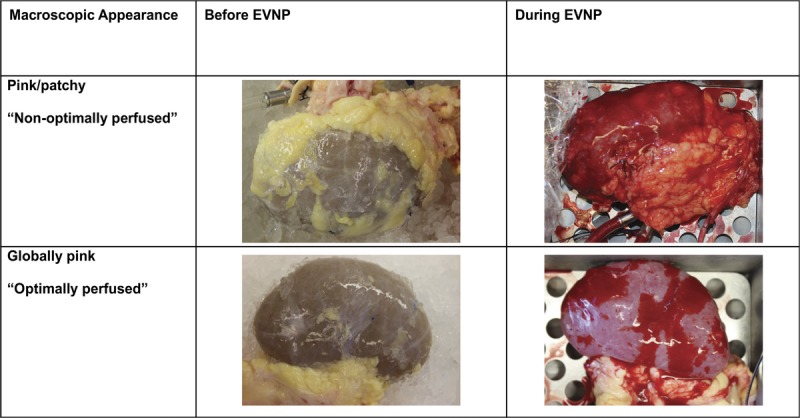
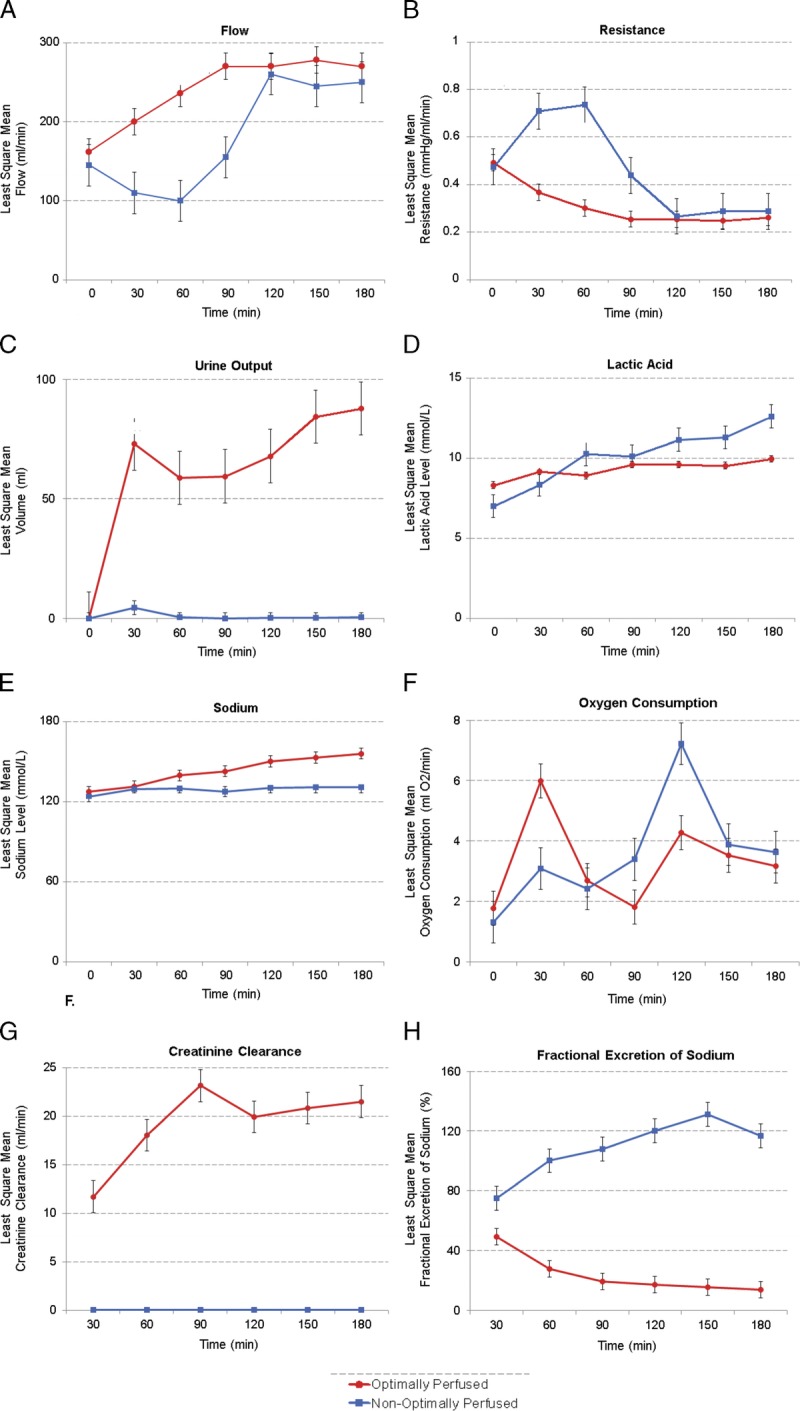
Results: After a mean CIT of 43.7 hours, all 7 kidneys appeared viable on EVNP with progressively increasing renal blood flow over the 3-hour period of perfusion. Five of the 7 kidneys had excellent macroscopic appearance, rapid increase in blood flow to 200 to 250 mL/min, urine output of 40 to 260 mL/h and increasing creatinine clearance.
Conclusions: Favorable perfusion characteristics and immediate function after a 3-hour course of EVNP suggests that high-risk kidneys subjected to long CIT may have been considered for transplantation. The combined use of ex vivo hypothermic and normothermic perfusion may be a useful strategy to more adequately assess and preserve high-risk kidneys deemed unsuitable for transplantation. A clinical trial will be necessary to validate the usefulness of this approach.
Conflict of interest statement
R.V.P. is a member of the clinical advisory board for XOR Laboratories, Toronto, Canada. All the other authors declare no conflicts of interest.
Figures
Comment in
-
Re: Combined Ex Vivo Hypothermic and Normothermic Perfusion for Assessment of High-Risk Deceased Donor Human Kidneys for Transplantation.J Urol. 2019 Aug;202(2):199-200. doi: 10.1097/JU.0000000000000300. Epub 2019 Jul 8. J Urol. 2019. PMID: 31021290 No abstract available.
Similar articles
-
Ex vivo normothermic perfusion for quality assessment of marginal donor kidney transplants.Br J Surg. 2015 Oct;102(11):1433-40. doi: 10.1002/bjs.9894. Epub 2015 Aug 27. Br J Surg. 2015. PMID: 26313559
-
Protocol of a randomised controlled, open-label trial of ex vivo normothermic perfusion versus static cold storage in donation after circulatory death renal transplantation.BMJ Open. 2017 Jan 23;7(1):e012237. doi: 10.1136/bmjopen-2016-012237. BMJ Open. 2017. PMID: 28115329 Free PMC article. Clinical Trial.
-
Successful Transplantation of Human Kidneys Deemed Untransplantable but Resuscitated by Ex Vivo Normothermic Machine Perfusion.Am J Transplant. 2016 Nov;16(11):3282-3285. doi: 10.1111/ajt.13906. Epub 2016 Jul 13. Am J Transplant. 2016. PMID: 27273794 Free PMC article.
-
Normothermic machine perfusion of the kidney: better conditioning and repair?Transpl Int. 2015 Jun;28(6):657-64. doi: 10.1111/tri.12319. Epub 2014 May 8. Transpl Int. 2015. PMID: 24629095 Review.
-
Pulsatile perfusion of kidney allografts.Curr Opin Organ Transplant. 2009 Aug;14(4):365-9. doi: 10.1097/mot.0b013e32832dbd1c. Curr Opin Organ Transplant. 2009. PMID: 19610170 Review.
Cited by
-
Assessment of hemodynamic and blood parameters that may reflect macroscopic quality of porcine kidneys during normothermic machine perfusion using whole blood.World J Urol. 2024 Aug 7;42(1):471. doi: 10.1007/s00345-024-05139-2. World J Urol. 2024. PMID: 39110171 Free PMC article.
-
Brief Normothermic Machine Perfusion Rejuvenates Discarded Human Kidneys.Transplant Direct. 2019 Oct 8;5(11):e502. doi: 10.1097/TXD.0000000000000944. eCollection 2019 Nov. Transplant Direct. 2019. PMID: 31773055 Free PMC article.
-
The Kidney Donor Profile Index (KDPI) Correlates With Histopathologic Findings in Post-reperfusion Baseline Biopsies and Predicts Kidney Transplant Outcome.Front Med (Lausanne). 2022 Apr 29;9:875206. doi: 10.3389/fmed.2022.875206. eCollection 2022. Front Med (Lausanne). 2022. PMID: 35573025 Free PMC article.
-
Kidney Perfusion as an Organ Quality Assessment Tool-Are We Counting Our Chickens Before They Have Hatched?J Clin Med. 2020 Mar 23;9(3):879. doi: 10.3390/jcm9030879. J Clin Med. 2020. PMID: 32210197 Free PMC article. Review.
-
US deceased kidney transplantation: Estimated GFR, donor age and KDPI association with graft survival.EClinicalMedicine. 2021 Jun 23;37:100980. doi: 10.1016/j.eclinm.2021.100980. eCollection 2021 Jul. EClinicalMedicine. 2021. PMID: 34386752 Free PMC article.
References
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
