

Outcome of cardiac surgery in patients with congenital heart disease in England between 1997 and 2015
- PMID: 28628610
- PMCID: PMC5476245
- DOI: 10.1371/journal.pone.0178963
Outcome of cardiac surgery in patients with congenital heart disease in England between 1997 and 2015
Abstract
Background: The number of patients with congenital heart disease (CHD) is increasing worldwide and most of them will require cardiac surgery, once or more, during their lifetime. The total volume of cardiac surgery in CHD patients at a national level and the associated mortality and predictors of death associated with surgery are not known. We aimed to investigate the surgical volume and associated mortality in CHD patients in England.
Methods: Using a national hospital episode statistics database, we identified all CHD patients undergoing cardiac surgery in England between 1997 and 2015.
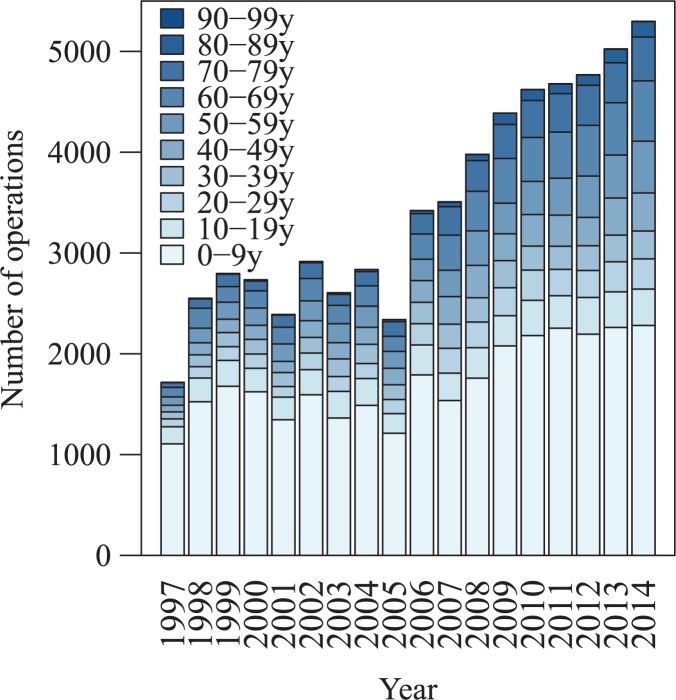
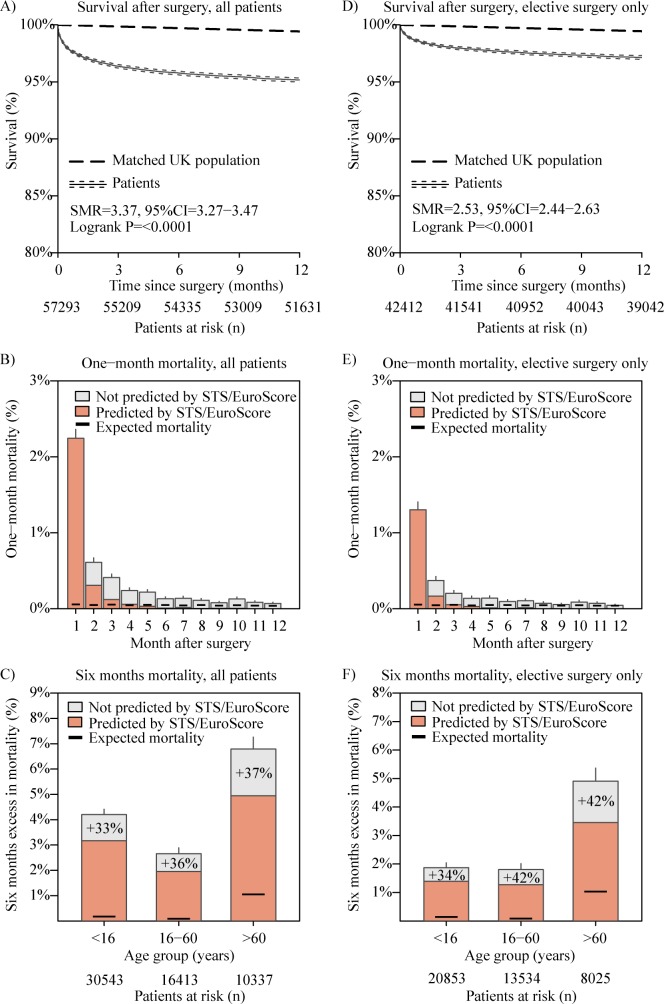
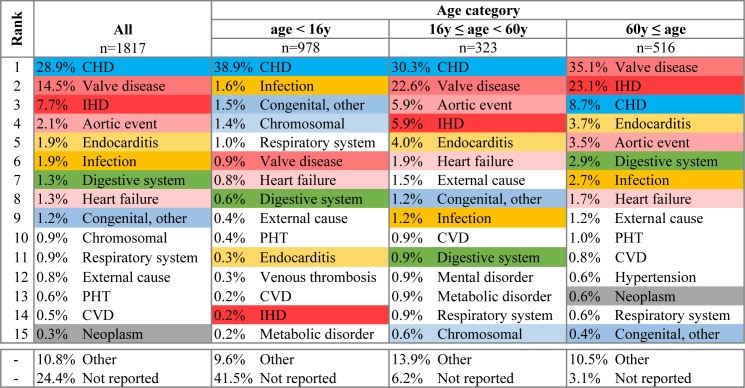
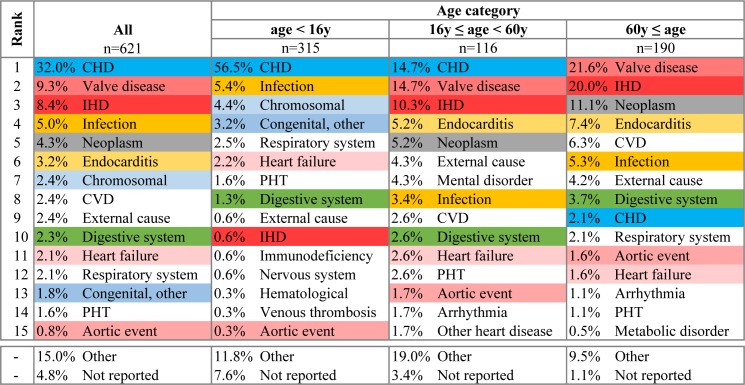
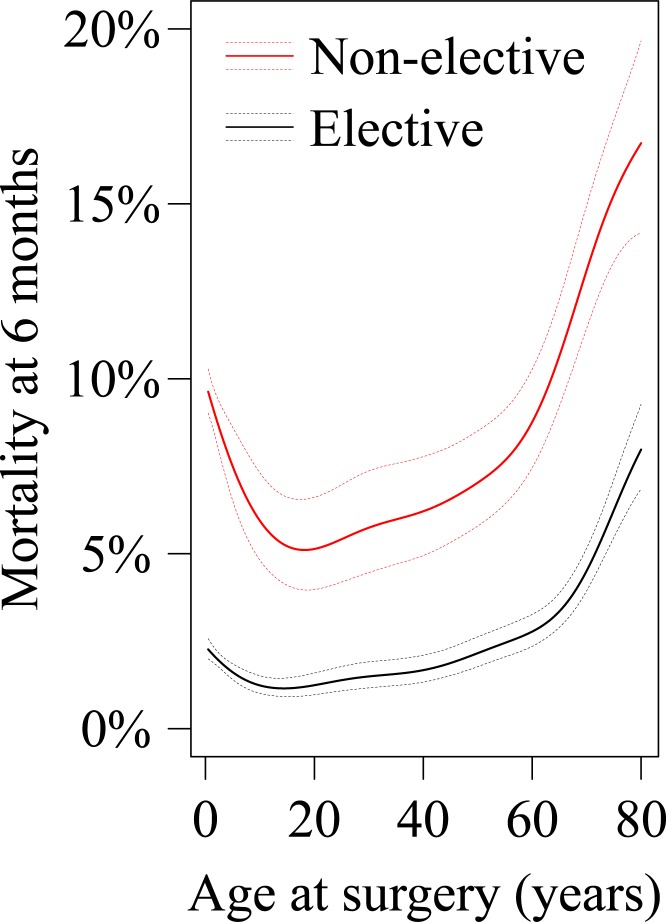
Results: We evaluated 57,293 patients (median age 11.9years, 46.7% being adult, 56.7% female). There was a linear increase in the number of operations performed per year from 1,717 in 1997 to 5,299 performed in 2014. The most common intervention at the last surgical event was an aortic valve procedure (9,276; 16.2%), followed by repair of atrial septal defect (9,154; 16.0%), ventricular septal defect (7,746; 13.5%), tetralogy of Fallot (3,523; 6.1%) and atrioventricular septal defect (3,330; 5.8%) repair. Associated mortality remained raised up to six months following cardiac surgery. Several parameters were predictive of post-operative mortality, including age, complexity of surgery, need for emergency surgery and socioeconomic status. The relationship of age with mortality was "U"-shaped, and mortality was highest amongst youngest children and adults above 60 years of age.
Conclusions: The number of cardiac operations performed in CHD patients in England has been increasing, particularly in adults. Mortality remains raised up to 6-months after surgery and was highest amongst young children and seniors.
Conflict of interest statement
Figures
Similar articles
-
28 years' experience with transatrial-transpulmonary repair of atrioventricular septal defect with tetralogy of Fallot.Ann Thorac Surg. 2008 May;85(5):1686-9. doi: 10.1016/j.athoracsur.2007.11.030. Ann Thorac Surg. 2008. PMID: 18442566
-
Outcome after repair of atrioventricular septal defect with tetralogy of Fallot.J Thorac Cardiovasc Surg. 2012 Feb;143(2):338-43. doi: 10.1016/j.jtcvs.2011.05.031. Epub 2011 Sep 8. J Thorac Cardiovasc Surg. 2012. PMID: 21855095
-
Atrial tachyarrhythmias and the Cox-maze procedure in congenital heart disease.Congenit Heart Dis. 2013 Sep-Oct;8(5):434-9. doi: 10.1111/chd.12031. Epub 2012 Dec 27. Congenit Heart Dis. 2013. PMID: 23280242
-
Current status of cardiovascular surgery in Japan 2013 and 2014: A report based on the Japan Cardiovascular Surgery Database. 2: Congenital heart surgery.Gen Thorac Cardiovasc Surg. 2018 Jan;66(1):4-7. doi: 10.1007/s11748-017-0841-6. Epub 2017 Nov 13. Gen Thorac Cardiovasc Surg. 2018. PMID: 29134535 Review.
-
Current readings: long-term management of patients undergoing successful pediatric cardiac surgery.Semin Thorac Cardiovasc Surg. 2014 Summer;26(2):132-44. doi: 10.1053/j.semtcvs.2014.08.002. Epub 2014 Aug 7. Semin Thorac Cardiovasc Surg. 2014. PMID: 25441004 Review.
Cited by
-
The state of cardiac surgery in Ethiopia.JTCVS Open. 2023 Mar 9;14:261-269. doi: 10.1016/j.xjon.2023.03.001. eCollection 2023 Jun. JTCVS Open. 2023. PMID: 37425461 Free PMC article.
-
Predictors of major adverse events and complications after ventricular septal defects surgical closure in children less than 10 kg.J Cardiothorac Surg. 2022 Sep 7;17(1):232. doi: 10.1186/s13019-022-01985-6. J Cardiothorac Surg. 2022. PMID: 36071526 Free PMC article.
-
Model-driven survival prediction after congenital heart surgery.Interdiscip Cardiovasc Thorac Surg. 2023 Sep 2;37(3):ivad089. doi: 10.1093/icvts/ivad089. Interdiscip Cardiovasc Thorac Surg. 2023. PMID: 37279735 Free PMC article.
-
Cerebral oxygenation during pediatric congenital cardiac surgery and its association with outcome: a retrospective observational study.Can J Anaesth. 2020 Sep;67(9):1170-1181. doi: 10.1007/s12630-020-01733-1. Epub 2020 Jun 15. Can J Anaesth. 2020. PMID: 32557197 Free PMC article.
-
Use of Fresh-frozen Plasma in Newborn Infants.Newborn (Clarksville). 2022 Jul-Sep;1(3):271-277. doi: 10.5005/jp-journals-11002-0039. Epub 2022 Jul 10. Newborn (Clarksville). 2022. PMID: 36339329 Free PMC article.
References
-
- Diller G-P, Kempny A, Alonso-Gonzalez R, Swan L, Uebing A, et al. (2015) Survival Prospects and Circumstances of Death in Contemporary Adult Congenital Heart Disease Patients Under Follow-Up at a Large Tertiary Centre. Circulation 132: 2118–2125. doi: 10.1161/CIRCULATIONAHA.115.017202 - DOI - PubMed
-
- Kogon B, Oster M (2014) Assessing surgical risk for adults with congenital heart disease: are pediatric scoring systems appropriate? J Thorac Cardiovasc Surg 147: 666–671. doi: 10.1016/j.jtcvs.2013.09.053 - DOI - PubMed
-
- Lacour-Gayet F, Clarke D, Jacobs J, Comas J, Daebritz S, et al. (2004) The Aristotle score: a complexity-adjusted method to evaluate surgical results. Eur J Cardiothorac Surg 25: 911–924. doi: 10.1016/j.ejcts.2004.03.027 - DOI - PubMed
-
- Jacobs ML, O'Brien SM, Jacobs JP, Mavroudis C, Lacour-Gayet F, et al. (2013) An empirically based tool for analyzing morbidity associated with operations for congenital heart disease. J Thorac Cardiovasc Surg 145: 1046–1057.e1041. doi: 10.1016/j.jtcvs.2012.06.029 - DOI - PMC - PubMed
-
- Jenkins KJ, Gauvreau K, Newburger JW, Spray TL, Moller JH, et al. (2002) Consensus-based method for risk adjustment for surgery for congenital heart disease. J Thorac Cardiovasc Surg 123: 110–118. - PubMed
MeSH terms
Supplementary concepts
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
