

Association Between Dietary Factors and Mortality From Heart Disease, Stroke, and Type 2 Diabetes in the United States
- PMID: 28267855
- PMCID: PMC5852674
- DOI: 10.1001/jama.2017.0947
Association Between Dietary Factors and Mortality From Heart Disease, Stroke, and Type 2 Diabetes in the United States
Abstract
Importance: In the United States, national associations of individual dietary factors with specific cardiometabolic diseases are not well established.
Objective: To estimate associations of intake of 10 specific dietary factors with mortality due to heart disease, stroke, and type 2 diabetes (cardiometabolic mortality) among US adults.
Design, setting, and participants: A comparative risk assessment model incorporated data and corresponding uncertainty on population demographics and dietary habits from National Health and Nutrition Examination Surveys (1999-2002: n = 8104; 2009-2012: n = 8516); estimated associations of diet and disease from meta-analyses of prospective studies and clinical trials with validity analyses to assess potential bias; and estimated disease-specific national mortality from the National Center for Health Statistics.
Exposures: Consumption of 10 foods/nutrients associated with cardiometabolic diseases: fruits, vegetables, nuts/seeds, whole grains, unprocessed red meats, processed meats, sugar-sweetened beverages (SSBs), polyunsaturated fats, seafood omega-3 fats, and sodium.
Main outcomes and measures: Estimated absolute and percentage mortality due to heart disease, stroke, and type 2 diabetes in 2012. Disease-specific and demographic-specific (age, sex, race, and education) mortality and trends between 2002 and 2012 were also evaluated.
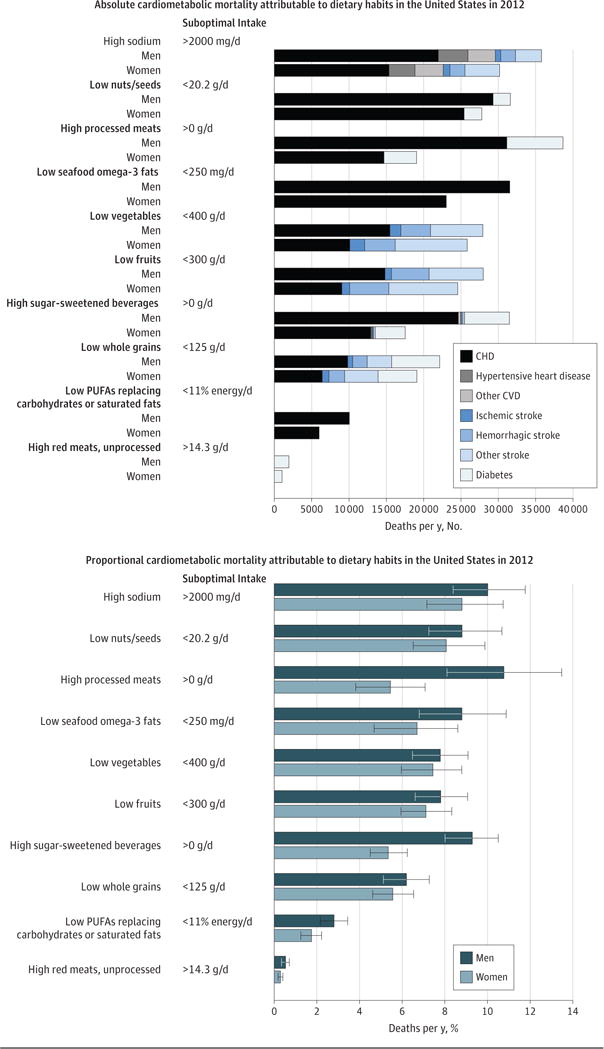
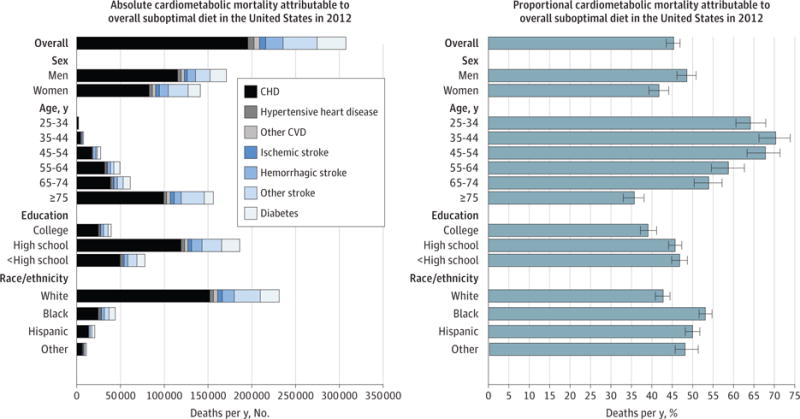
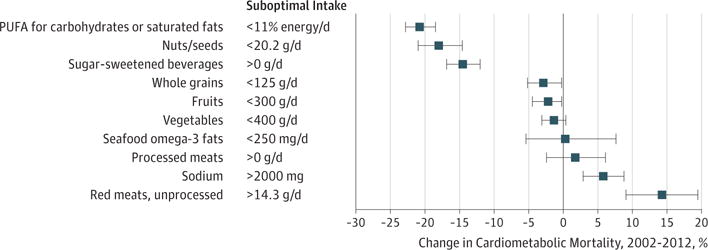
Results: In 2012, 702 308 cardiometabolic deaths occurred in US adults, including 506 100 from heart disease (371 266 coronary heart disease, 35 019 hypertensive heart disease, and 99 815 other cardiovascular disease), 128 294 from stroke (16 125 ischemic, 32 591 hemorrhagic, and 79 578 other), and 67 914 from type 2 diabetes. Of these, an estimated 318 656 (95% uncertainty interval [UI], 306 064-329 755; 45.4%) cardiometabolic deaths per year were associated with suboptimal intakes-48.6% (95% UI, 46.2%-50.9%) of cardiometabolic deaths in men and 41.8% (95% UI, 39.3%-44.2%) in women; 64.2% (95% UI, 60.6%-67.9%) at younger ages (25-34 years) and 35.7% (95% UI, 33.1%-38.1%) at older ages (≥75 years); 53.1% (95% UI, 51.6%-54.8%) among blacks, 50.0% (95% UI, 48.2%-51.8%) among Hispanics, and 42.8% (95% UI, 40.9%-44.5%) among whites; and 46.8% (95% UI, 44.9%-48.7%) among lower-, 45.7% (95% UI, 44.2%-47.4%) among medium-, and 39.1% (95% UI, 37.2%-41.2%) among higher-educated individuals. The largest numbers of estimated diet-related cardiometabolic deaths were related to high sodium (66 508 deaths in 2012; 9.5% of all cardiometabolic deaths), low nuts/seeds (59 374; 8.5%), high processed meats (57 766; 8.2%), low seafood omega-3 fats (54 626; 7.8%), low vegetables (53 410; 7.6%), low fruits (52 547; 7.5%), and high SSBs (51 694; 7.4%). Between 2002 and 2012, population-adjusted US cardiometabolic deaths per year decreased by 26.5%. The greatest decline was associated with insufficient polyunsaturated fats (-20.8% relative change [95% UI, -18.5% to -22.8%]), nuts/seeds (-18.0% [95% UI, -14.6% to -21.0%]), and excess SSBs (-14.5% [95% UI, -12.0% to -16.9%]). The greatest increase was associated with unprocessed red meats (+14.4% [95% UI, 9.1%-19.5%]).
Conclusions and relevance: Dietary factors were estimated to be associated with a substantial proportion of deaths from heart disease, stroke, and type 2 diabetes. These results should help identify priorities, guide public health planning, and inform strategies to alter dietary habits and improve health.
Conflict of interest statement
Figures
Comment in
-
Attributing Death to Diet: Precision Counts.JAMA. 2017 Mar 7;317(9):908-909. doi: 10.1001/jama.2017.0946. JAMA. 2017. PMID: 28267836 No abstract available.
Similar articles
-
Dietary Intake Among US Adults, 1999-2012.JAMA. 2016 Jun 21;315(23):2542-53. doi: 10.1001/jama.2016.7491. JAMA. 2016. PMID: 27327801 Free PMC article.
-
Cardiometabolic disease costs associated with suboptimal diet in the United States: A cost analysis based on a microsimulation model.PLoS Med. 2019 Dec 17;16(12):e1002981. doi: 10.1371/journal.pmed.1002981. eCollection 2019 Dec. PLoS Med. 2019. PMID: 31846453 Free PMC article.
-
The potential impact of food taxes and subsidies on cardiovascular disease and diabetes burden and disparities in the United States.BMC Med. 2017 Nov 27;15(1):208. doi: 10.1186/s12916-017-0971-9. BMC Med. 2017. PMID: 29178869 Free PMC article.
-
Etiologic effects and optimal intakes of foods and nutrients for risk of cardiovascular diseases and diabetes: Systematic reviews and meta-analyses from the Nutrition and Chronic Diseases Expert Group (NutriCoDE).PLoS One. 2017 Apr 27;12(4):e0175149. doi: 10.1371/journal.pone.0175149. eCollection 2017. PLoS One. 2017. PMID: 28448503 Free PMC article. Review.
-
Dietary Patterns and All-Cause Mortality: A Systematic Review [Internet].Alexandria (VA): USDA Nutrition Evidence Systematic Review; 2020 Jul. Alexandria (VA): USDA Nutrition Evidence Systematic Review; 2020 Jul. PMID: 35258870 Free Books & Documents. Review.
Cited by
-
Trends in Food Sources and Diet Quality Among US Children and Adults, 2003-2018.JAMA Netw Open. 2021 Apr 1;4(4):e215262. doi: 10.1001/jamanetworkopen.2021.5262. JAMA Netw Open. 2021. PMID: 33844000 Free PMC article.
-
Sodium-glucose co-transporter-2 inhibitors reduce the risk of new-onset stroke in patients with type 2 diabetes: A population-based cohort study.Front Cardiovasc Med. 2022 Aug 9;9:966708. doi: 10.3389/fcvm.2022.966708. eCollection 2022. Front Cardiovasc Med. 2022. PMID: 36035934 Free PMC article.
-
Variation in diet quality across sexual orientation in a cohort of U.S. women.Cancer Causes Control. 2021 Jun;32(6):645-651. doi: 10.1007/s10552-021-01418-0. Epub 2021 Apr 12. Cancer Causes Control. 2021. PMID: 33846853 Free PMC article.
-
Dietary policies and programs in the United States: A narrative review.Prev Med Rep. 2020 May 31;19:101135. doi: 10.1016/j.pmedr.2020.101135. eCollection 2020 Sep. Prev Med Rep. 2020. PMID: 32551216 Free PMC article. Review.
-
Dietary Macronutrient Intake and Cardiovascular Disease Risk and Mortality: A Systematic Review and Dose-Response Meta-Analysis of Prospective Cohort Studies.Nutrients. 2024 Jan 2;16(1):152. doi: 10.3390/nu16010152. Nutrients. 2024. PMID: 38201983 Free PMC article. Review.
References
-
- Forouzanfar MH, Alexander L, Anderson HR, et al. GBD 2013 Risk Factors Collaborators Global, regional, and national comparative risk assessment of 79 behavioural, environmental and occupational, and metabolic risks or clusters of risks in 188 countries, 1990-2013: a systematic analysis for the Global Burden of Disease Study 2013. Lancet. 2015;386(10010):2287–2323. - PMC - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
