

Global, regional, and national life expectancy, all-cause mortality, and cause-specific mortality for 249 causes of death, 1980-2015: a systematic analysis for the Global Burden of Disease Study 2015
- PMID: 27733281
- PMCID: PMC5388903
- DOI: 10.1016/S0140-6736(16)31012-1
Global, regional, and national life expectancy, all-cause mortality, and cause-specific mortality for 249 causes of death, 1980-2015: a systematic analysis for the Global Burden of Disease Study 2015
Erratum in
-
Department of Error.Lancet. 2017 Jan 7;389(10064):e1. doi: 10.1016/S0140-6736(16)32605-8. Epub 2017 Jan 6. Lancet. 2017. PMID: 28091379 Free PMC article. No abstract available.
Abstract
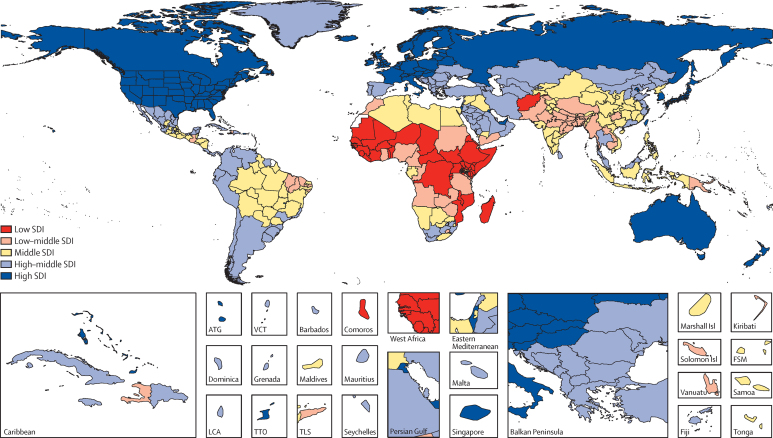
Background: Improving survival and extending the longevity of life for all populations requires timely, robust evidence on local mortality levels and trends. The Global Burden of Disease 2015 Study (GBD 2015) provides a comprehensive assessment of all-cause and cause-specific mortality for 249 causes in 195 countries and territories from 1980 to 2015. These results informed an in-depth investigation of observed and expected mortality patterns based on sociodemographic measures.
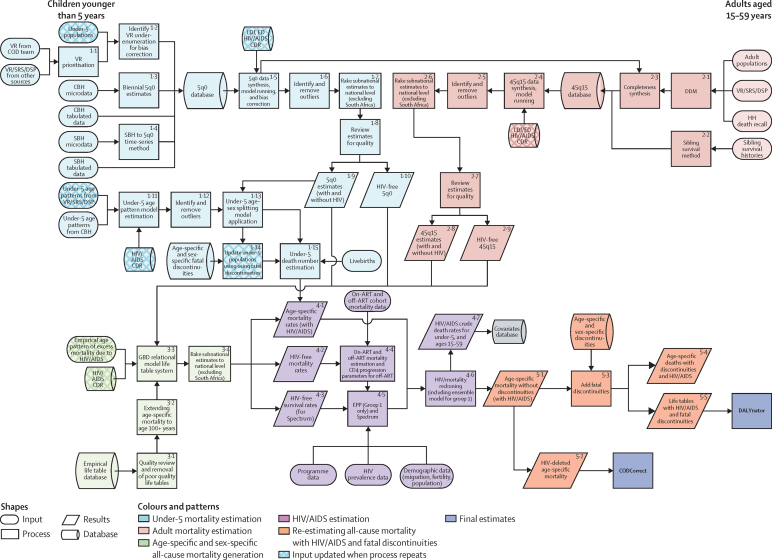
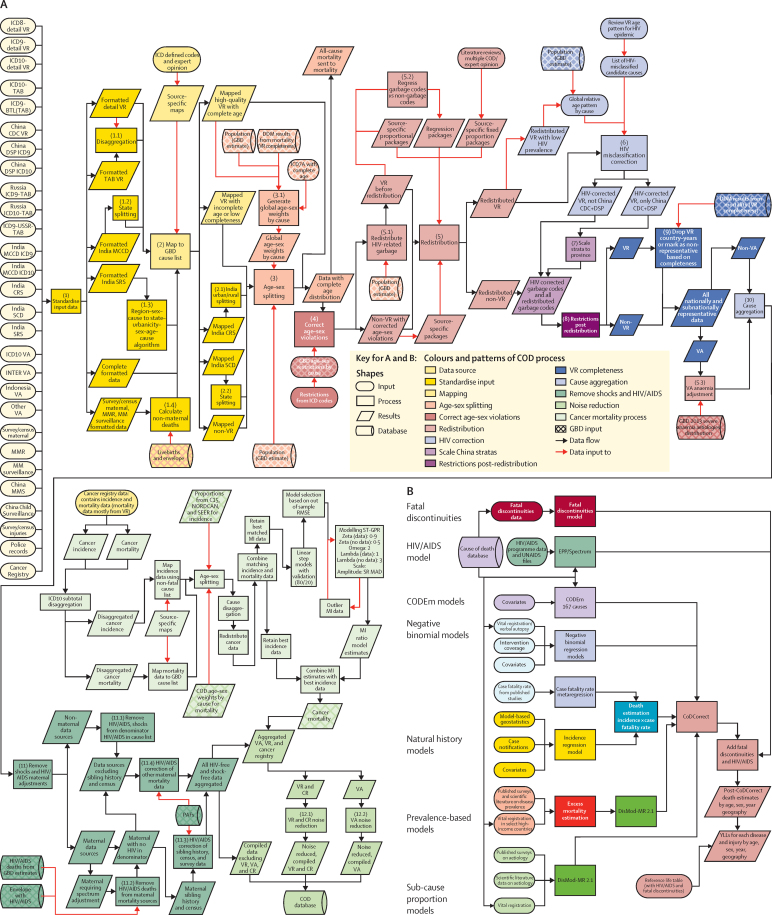
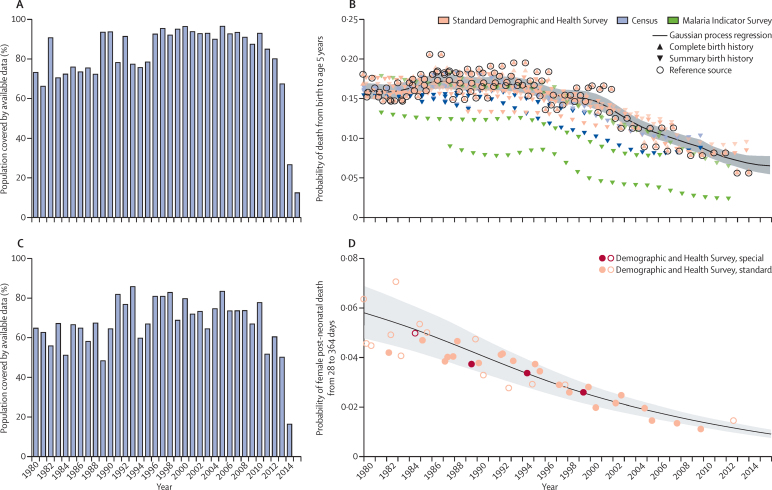
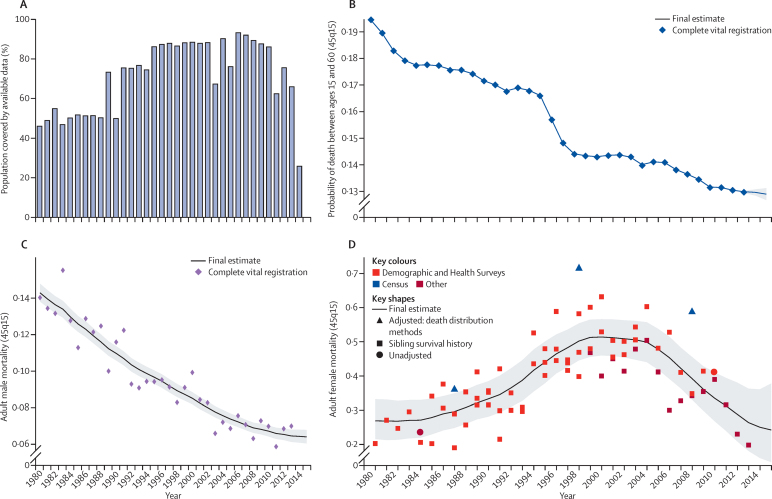
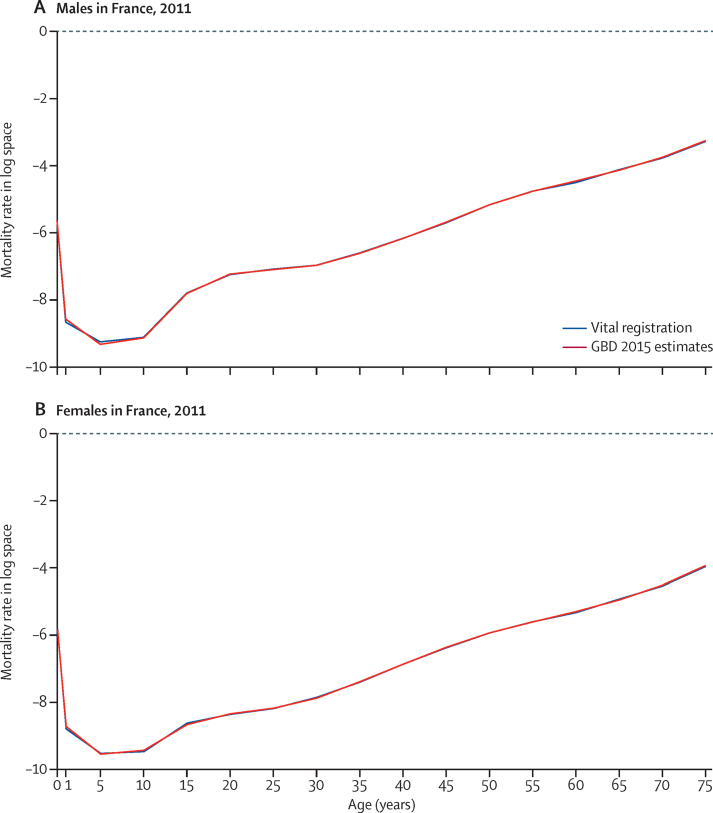
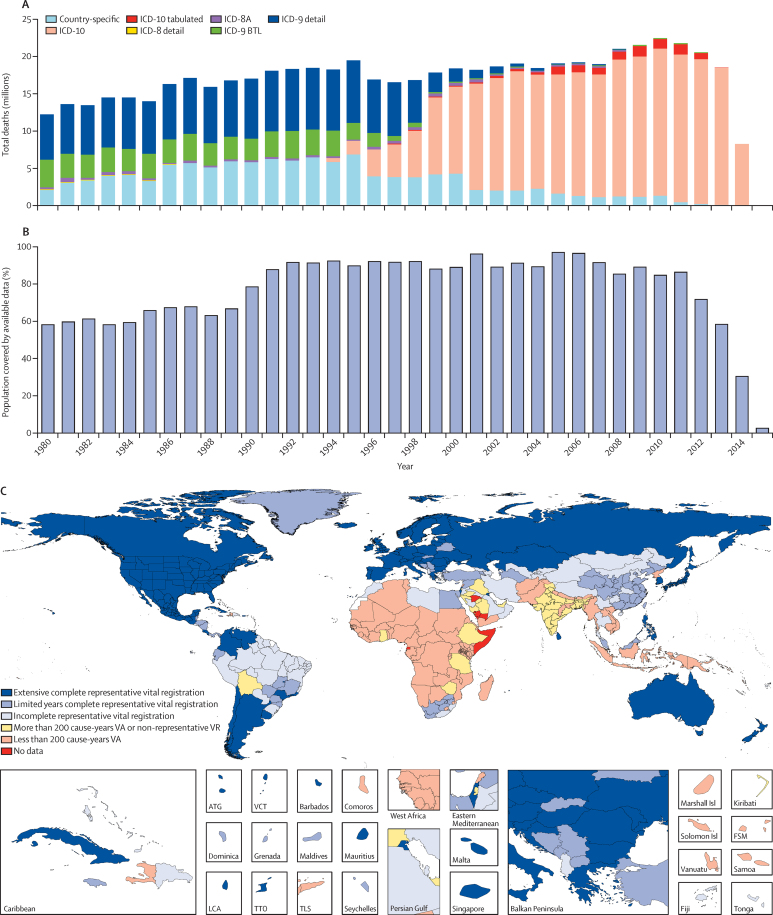
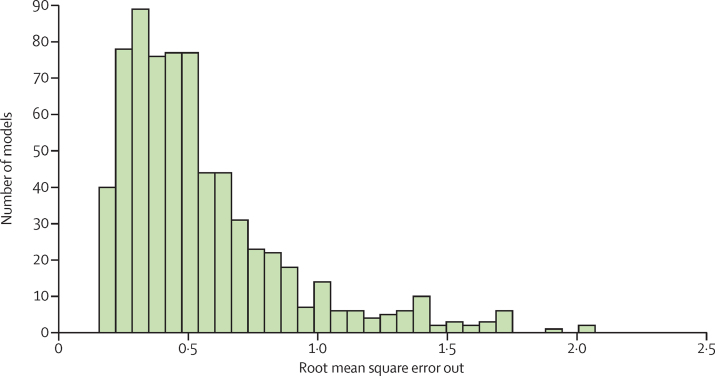
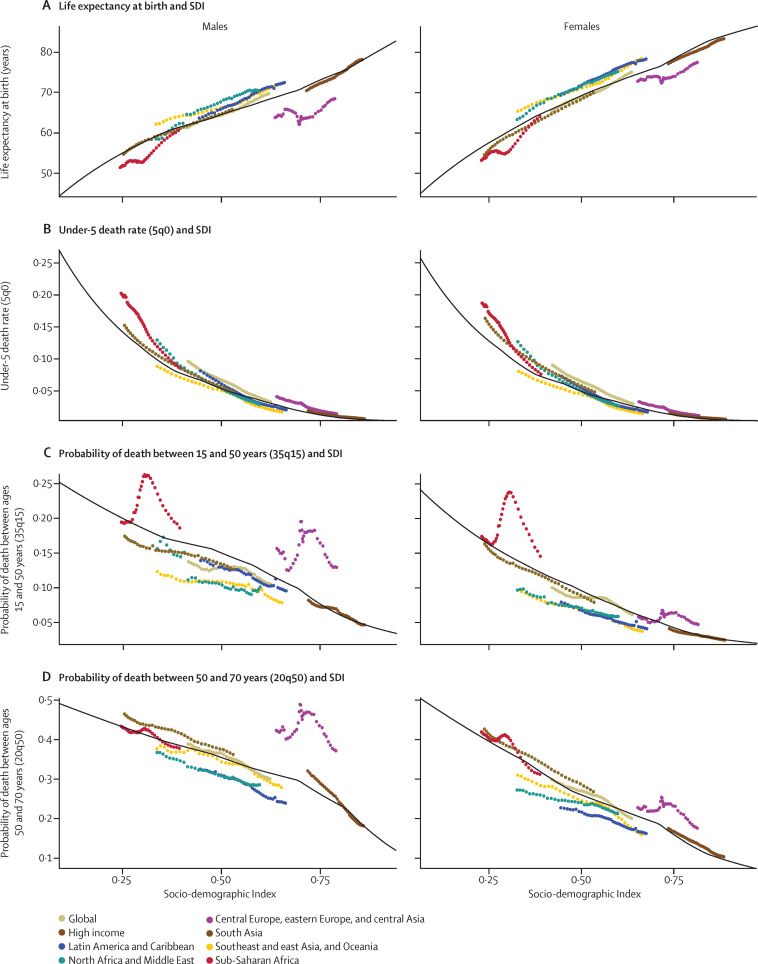
Methods: We estimated all-cause mortality by age, sex, geography, and year using an improved analytical approach originally developed for GBD 2013 and GBD 2010. Improvements included refinements to the estimation of child and adult mortality and corresponding uncertainty, parameter selection for under-5 mortality synthesis by spatiotemporal Gaussian process regression, and sibling history data processing. We also expanded the database of vital registration, survey, and census data to 14 294 geography-year datapoints. For GBD 2015, eight causes, including Ebola virus disease, were added to the previous GBD cause list for mortality. We used six modelling approaches to assess cause-specific mortality, with the Cause of Death Ensemble Model (CODEm) generating estimates for most causes. We used a series of novel analyses to systematically quantify the drivers of trends in mortality across geographies. First, we assessed observed and expected levels and trends of cause-specific mortality as they relate to the Socio-demographic Index (SDI), a summary indicator derived from measures of income per capita, educational attainment, and fertility. Second, we examined factors affecting total mortality patterns through a series of counterfactual scenarios, testing the magnitude by which population growth, population age structures, and epidemiological changes contributed to shifts in mortality. Finally, we attributed changes in life expectancy to changes in cause of death. We documented each step of the GBD 2015 estimation processes, as well as data sources, in accordance with Guidelines for Accurate and Transparent Health Estimates Reporting (GATHER).
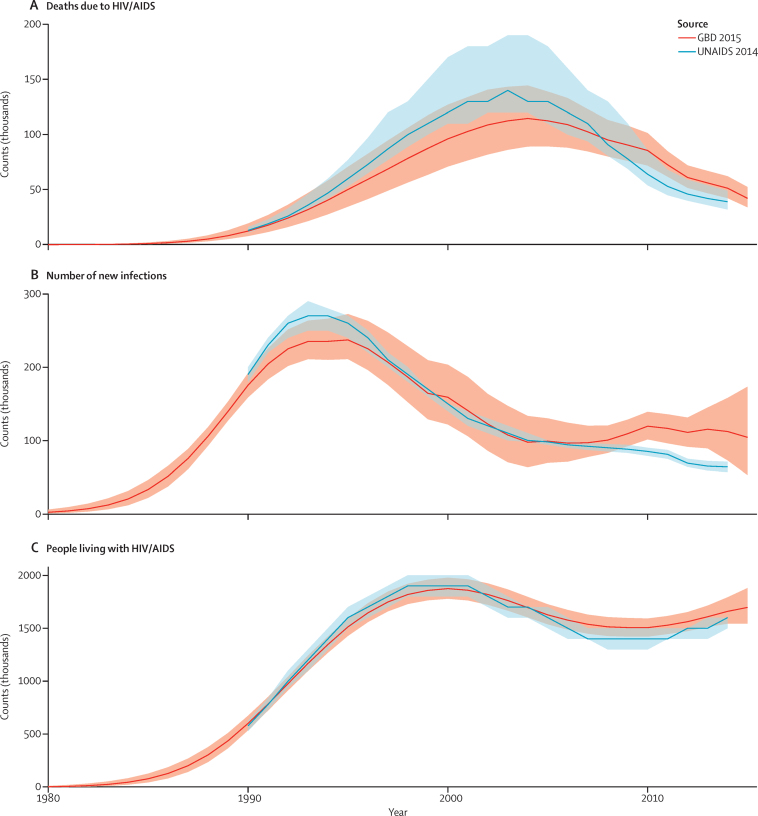
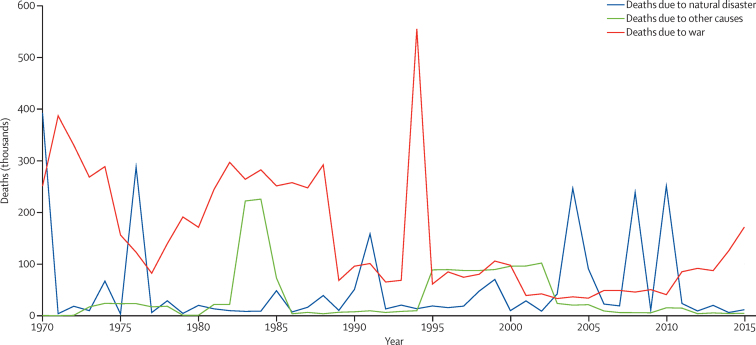
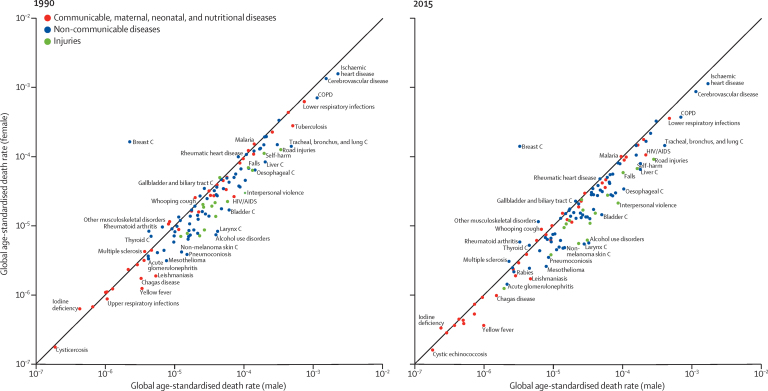
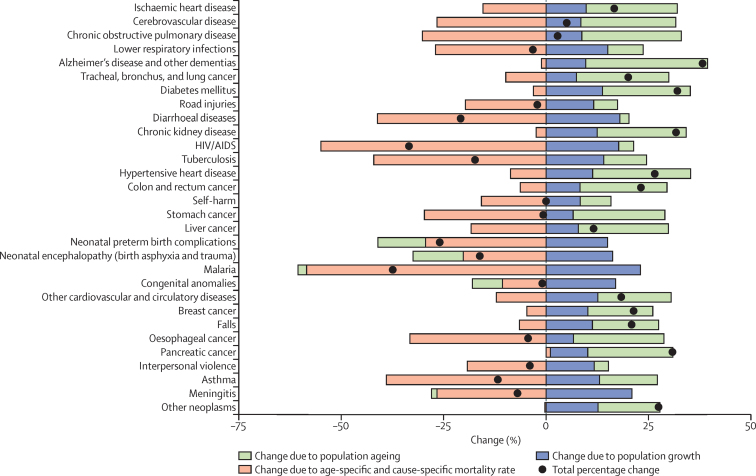
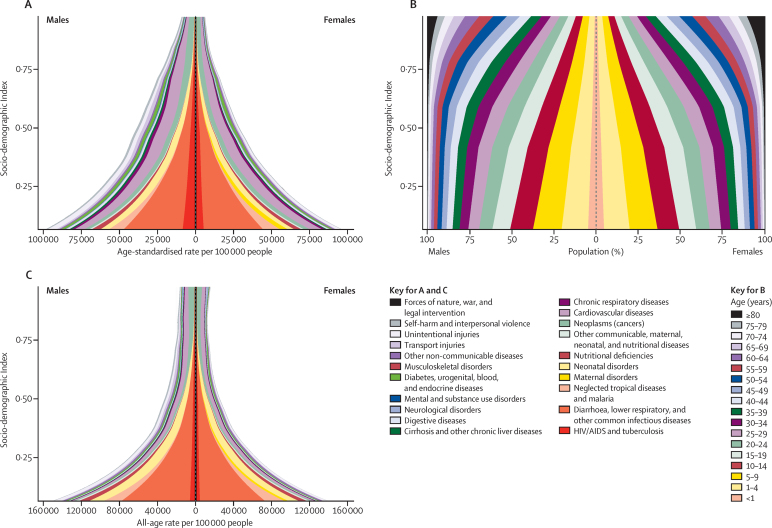
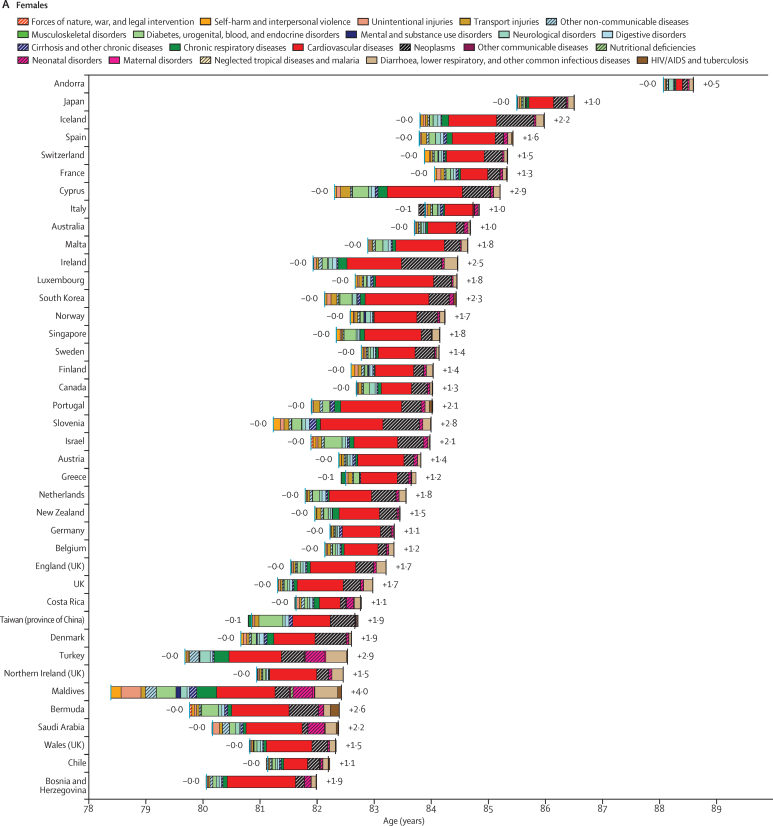
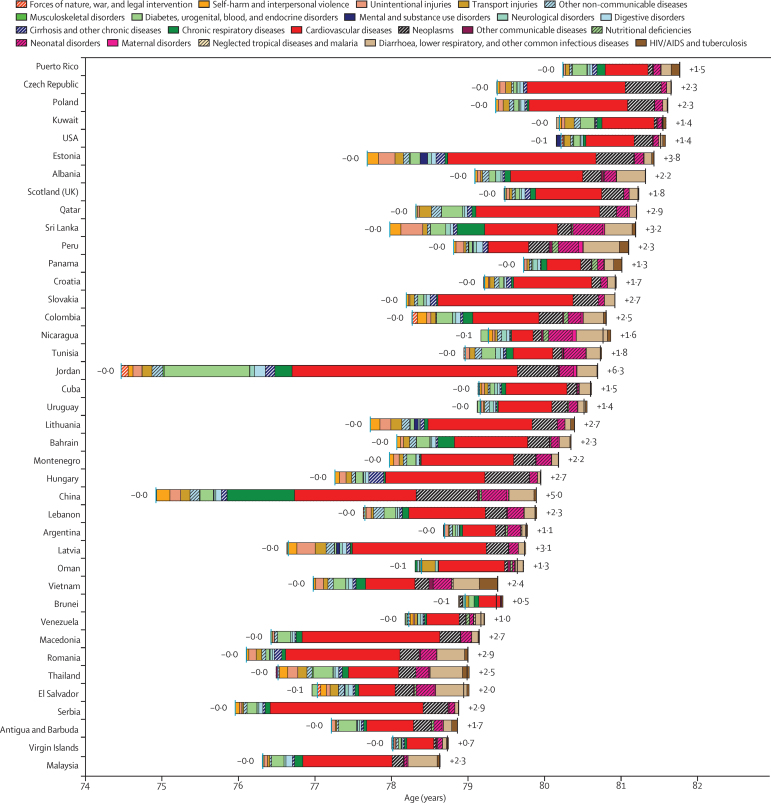
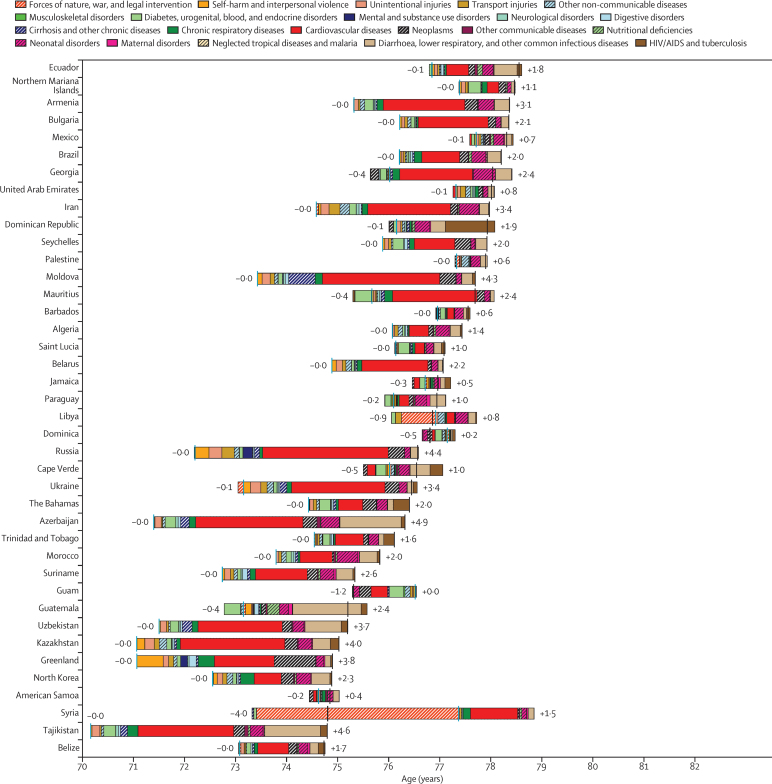
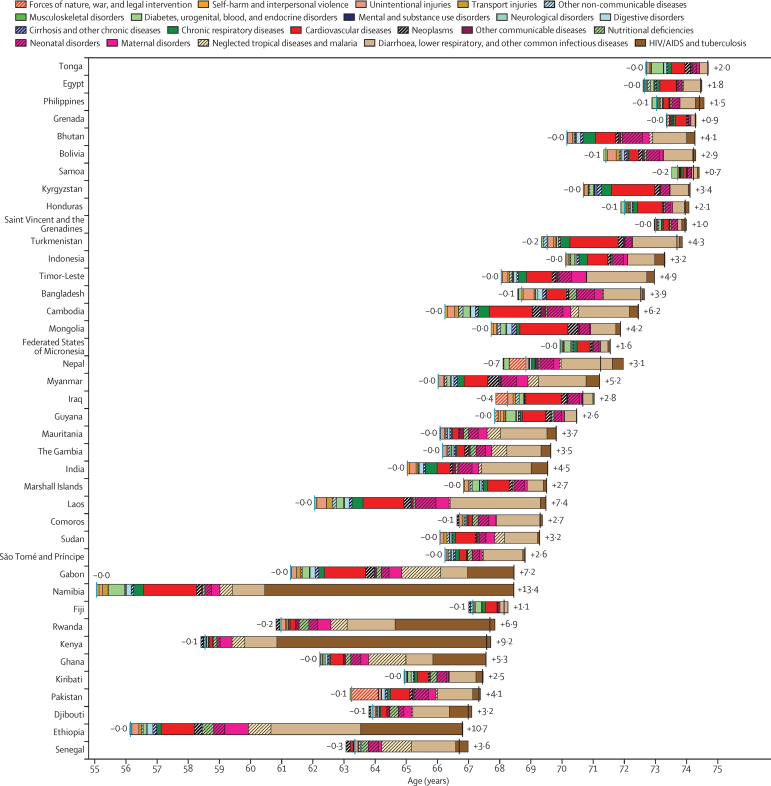
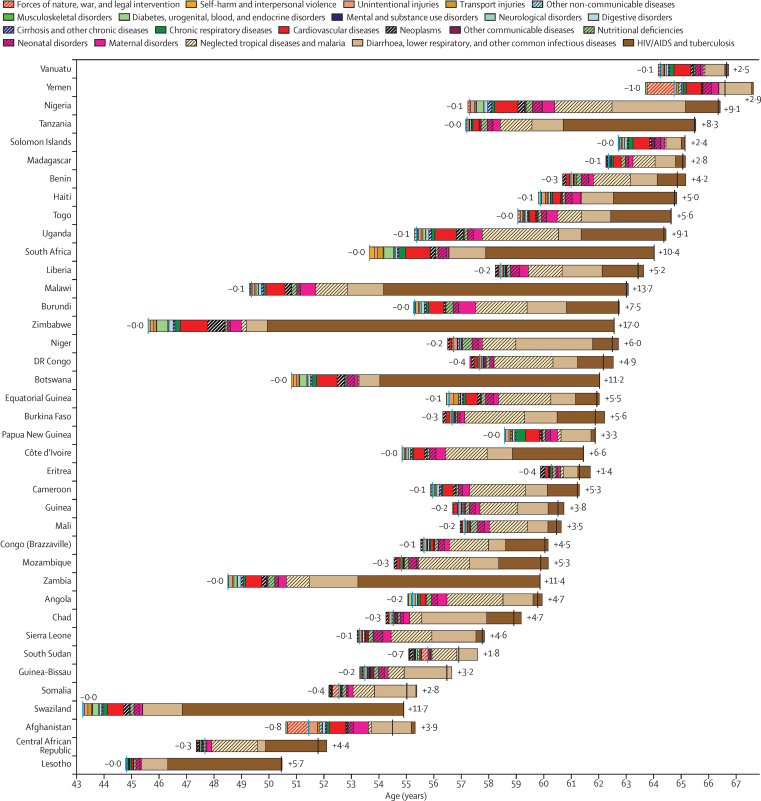
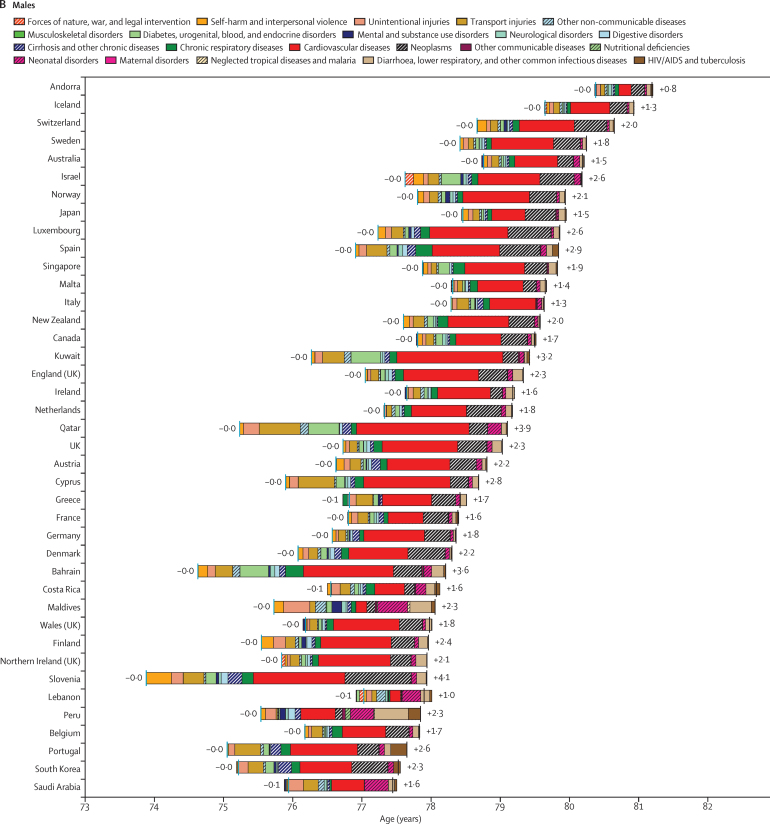
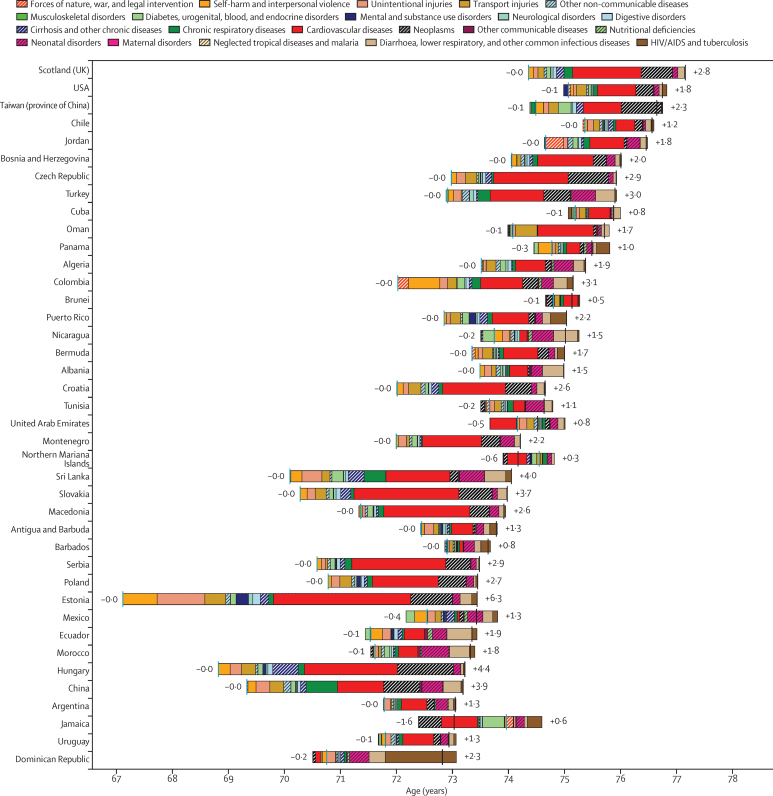
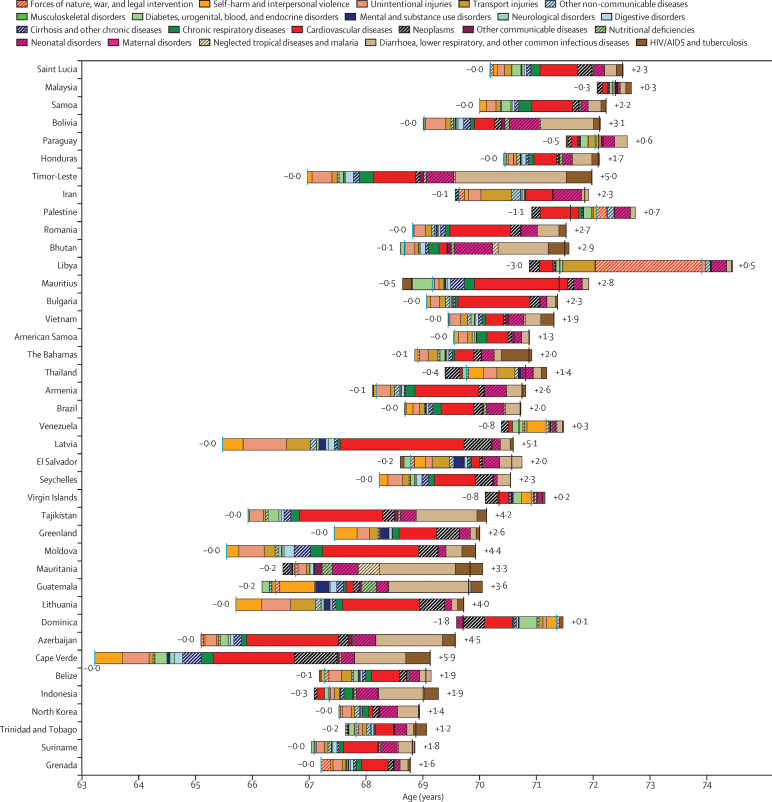
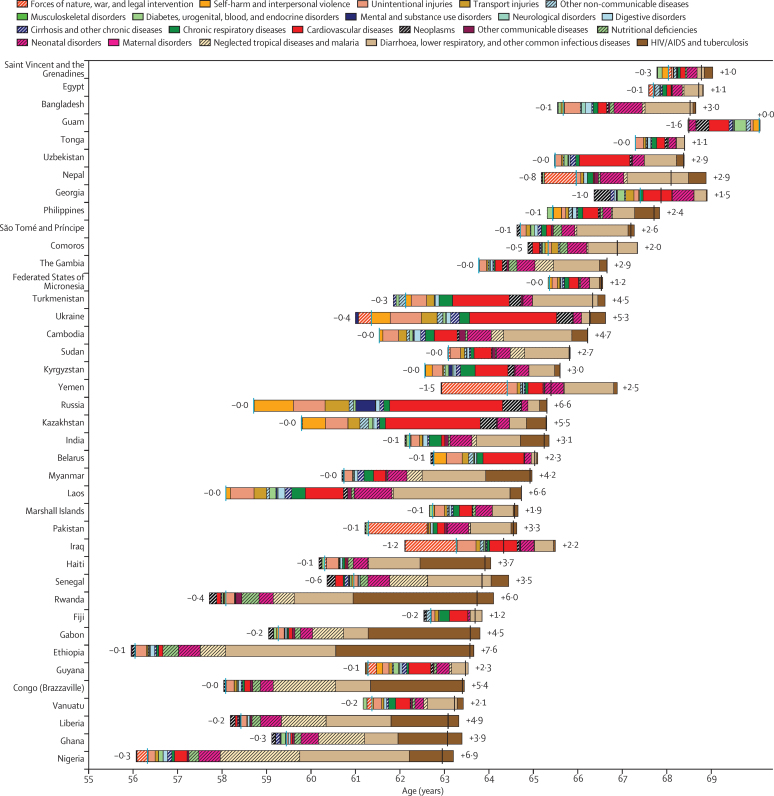
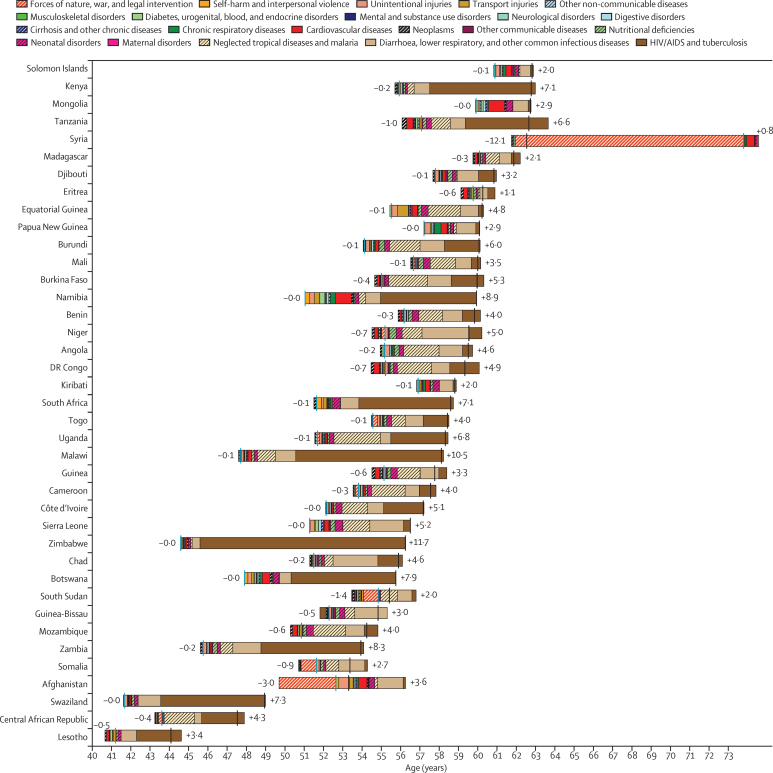
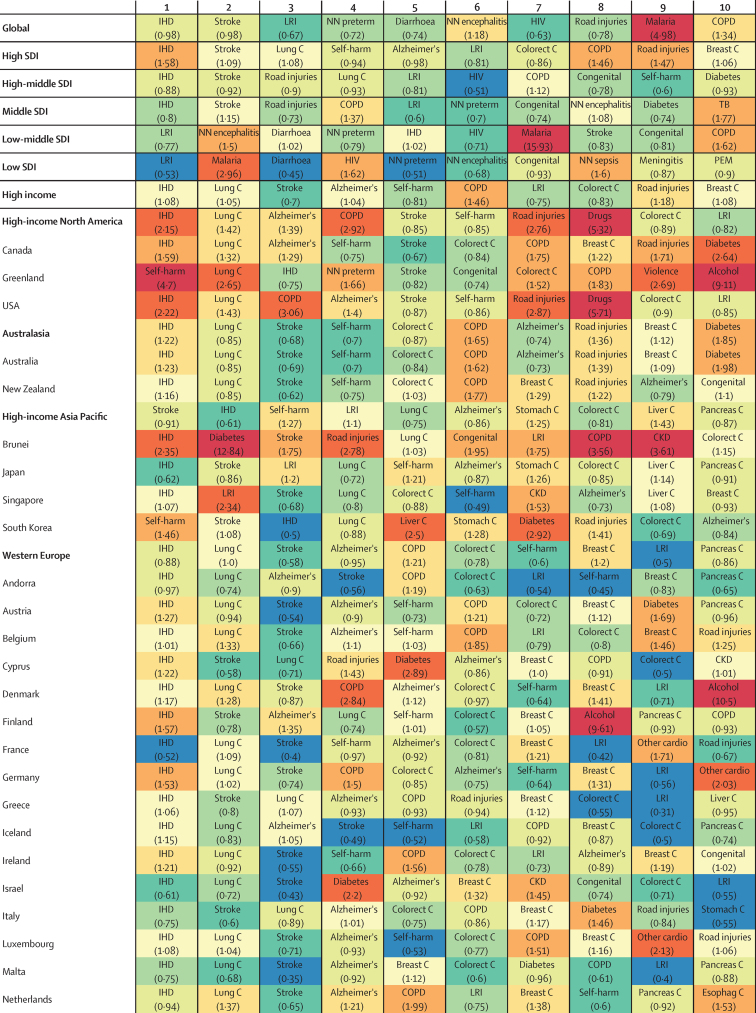
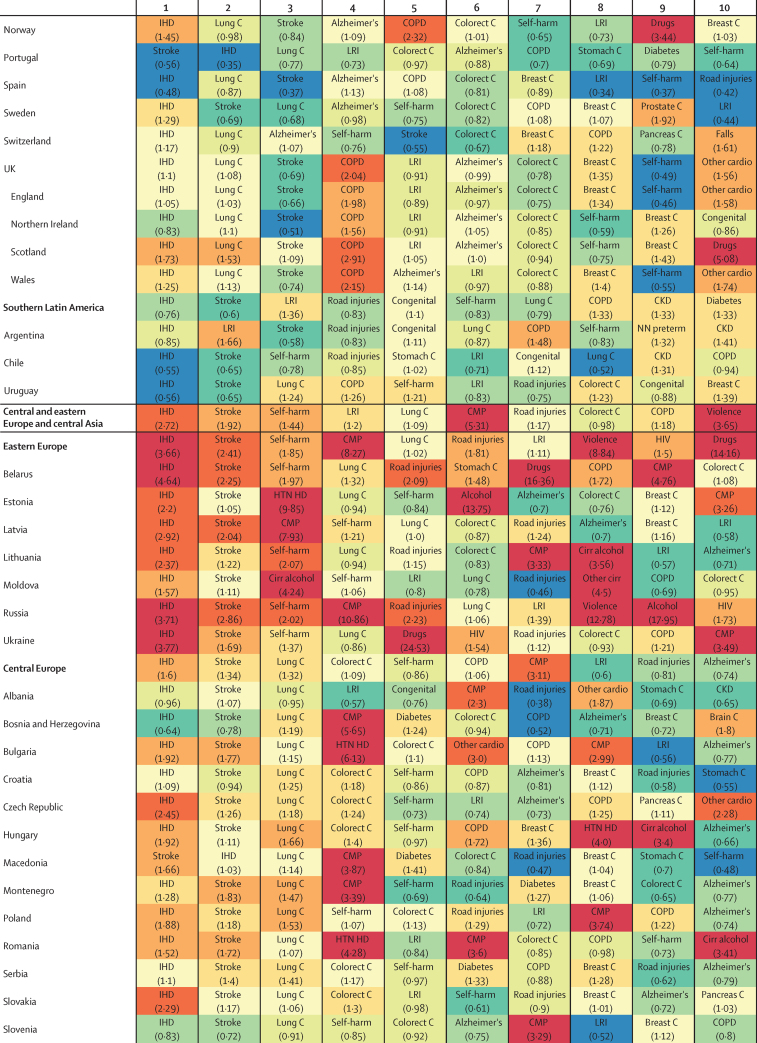
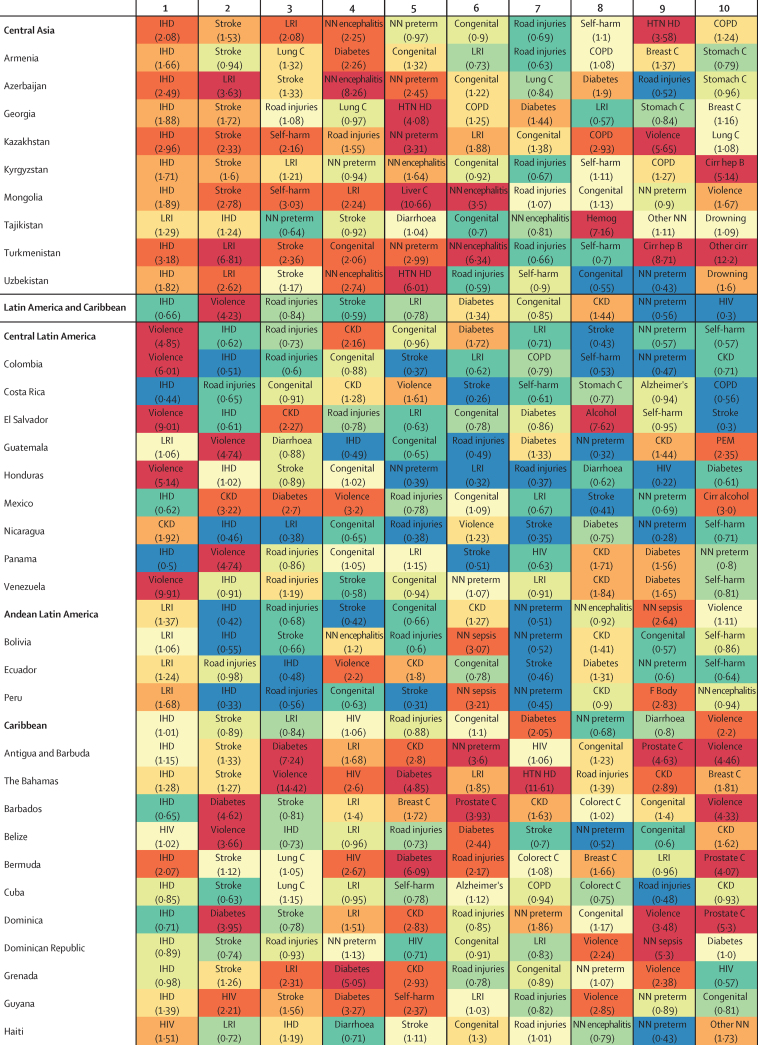
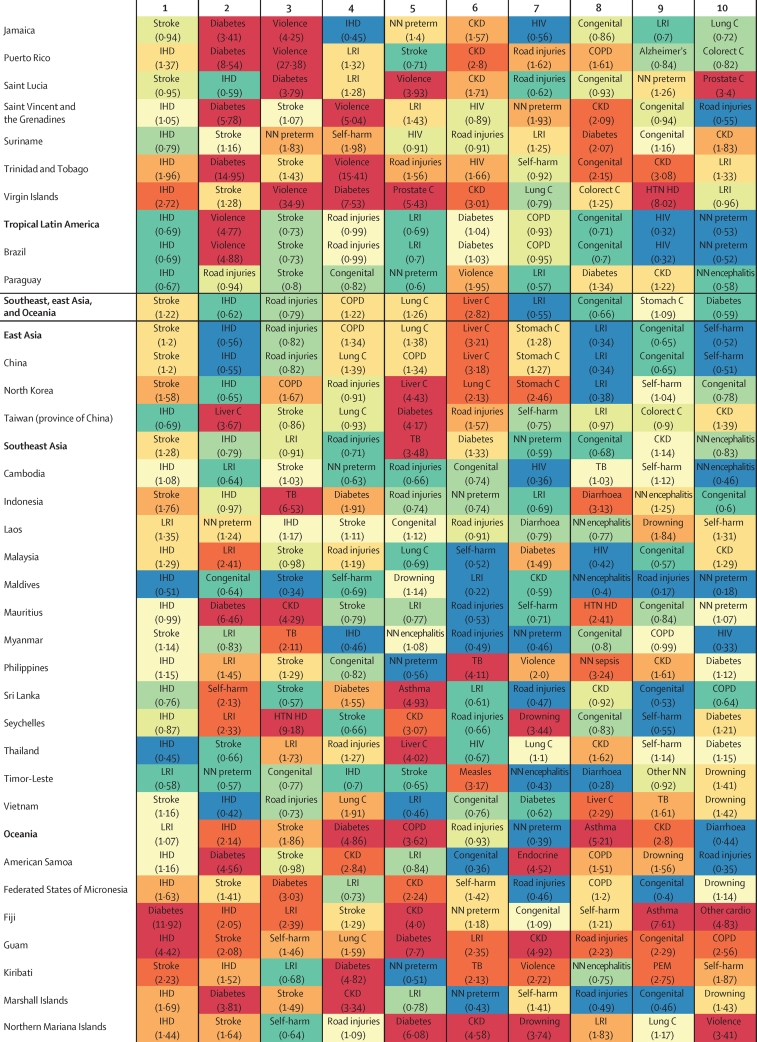
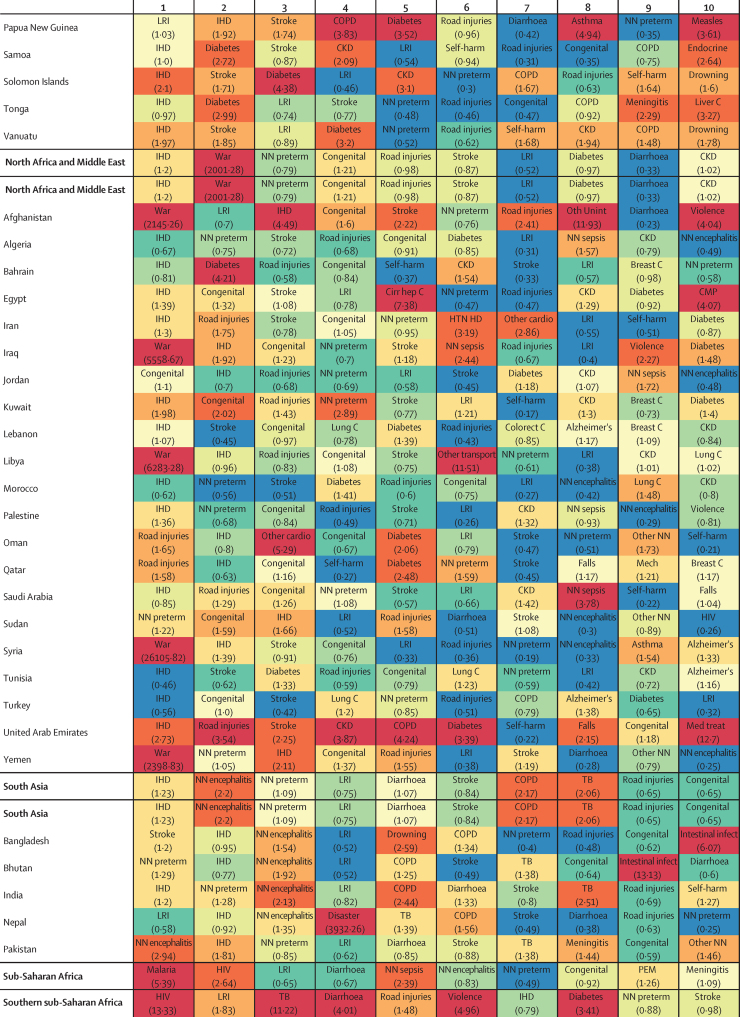
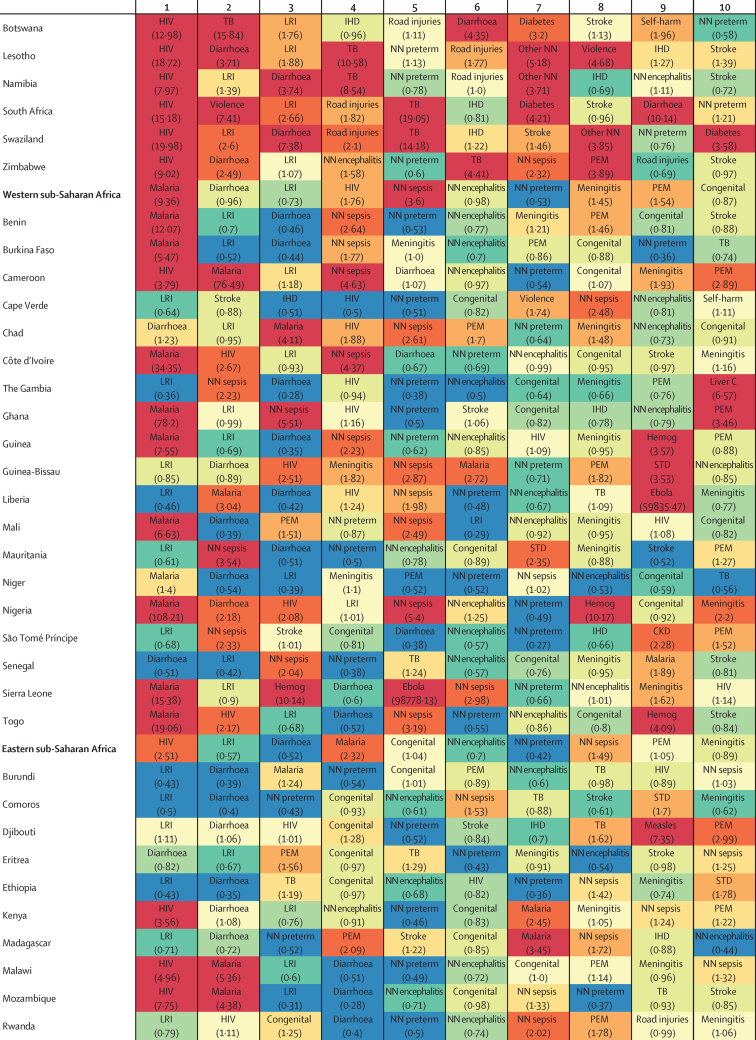
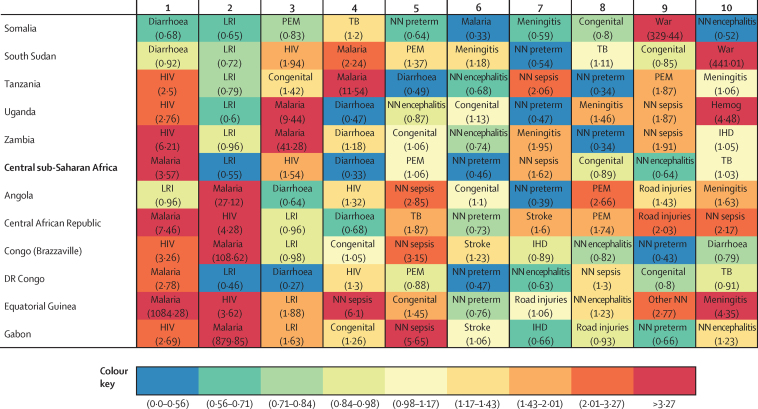
Findings: Globally, life expectancy from birth increased from 61·7 years (95% uncertainty interval 61·4-61·9) in 1980 to 71·8 years (71·5-72·2) in 2015. Several countries in sub-Saharan Africa had very large gains in life expectancy from 2005 to 2015, rebounding from an era of exceedingly high loss of life due to HIV/AIDS. At the same time, many geographies saw life expectancy stagnate or decline, particularly for men and in countries with rising mortality from war or interpersonal violence. From 2005 to 2015, male life expectancy in Syria dropped by 11·3 years (3·7-17·4), to 62·6 years (56·5-70·2). Total deaths increased by 4·1% (2·6-5·6) from 2005 to 2015, rising to 55·8 million (54·9 million to 56·6 million) in 2015, but age-standardised death rates fell by 17·0% (15·8-18·1) during this time, underscoring changes in population growth and shifts in global age structures. The result was similar for non-communicable diseases (NCDs), with total deaths from these causes increasing by 14·1% (12·6-16·0) to 39·8 million (39·2 million to 40·5 million) in 2015, whereas age-standardised rates decreased by 13·1% (11·9-14·3). Globally, this mortality pattern emerged for several NCDs, including several types of cancer, ischaemic heart disease, cirrhosis, and Alzheimer's disease and other dementias. By contrast, both total deaths and age-standardised death rates due to communicable, maternal, neonatal, and nutritional conditions significantly declined from 2005 to 2015, gains largely attributable to decreases in mortality rates due to HIV/AIDS (42·1%, 39·1-44·6), malaria (43·1%, 34·7-51·8), neonatal preterm birth complications (29·8%, 24·8-34·9), and maternal disorders (29·1%, 19·3-37·1). Progress was slower for several causes, such as lower respiratory infections and nutritional deficiencies, whereas deaths increased for others, including dengue and drug use disorders. Age-standardised death rates due to injuries significantly declined from 2005 to 2015, yet interpersonal violence and war claimed increasingly more lives in some regions, particularly in the Middle East. In 2015, rotaviral enteritis (rotavirus) was the leading cause of under-5 deaths due to diarrhoea (146 000 deaths, 118 000-183 000) and pneumococcal pneumonia was the leading cause of under-5 deaths due to lower respiratory infections (393 000 deaths, 228 000-532 000), although pathogen-specific mortality varied by region. Globally, the effects of population growth, ageing, and changes in age-standardised death rates substantially differed by cause. Our analyses on the expected associations between cause-specific mortality and SDI show the regular shifts in cause of death composition and population age structure with rising SDI. Country patterns of premature mortality (measured as years of life lost [YLLs]) and how they differ from the level expected on the basis of SDI alone revealed distinct but highly heterogeneous patterns by region and country or territory. Ischaemic heart disease, stroke, and diabetes were among the leading causes of YLLs in most regions, but in many cases, intraregional results sharply diverged for ratios of observed and expected YLLs based on SDI. Communicable, maternal, neonatal, and nutritional diseases caused the most YLLs throughout sub-Saharan Africa, with observed YLLs far exceeding expected YLLs for countries in which malaria or HIV/AIDS remained the leading causes of early death.
Interpretation: At the global scale, age-specific mortality has steadily improved over the past 35 years; this pattern of general progress continued in the past decade. Progress has been faster in most countries than expected on the basis of development measured by the SDI. Against this background of progress, some countries have seen falls in life expectancy, and age-standardised death rates for some causes are increasing. Despite progress in reducing age-standardised death rates, population growth and ageing mean that the number of deaths from most non-communicable causes are increasing in most countries, putting increased demands on health systems.
Funding: Bill & Melinda Gates Foundation.
Copyright © 2016 The Author(s). Published by Elsevier Ltd. This is an Open Access article under the CC BY license. Published by Elsevier Ltd.. All rights reserved.
Figures
Comment in
-
Expanding GBD collaboration-call for experts in health financing and health systems.Lancet. 2017 Jan 7;389(10064):18-19. doi: 10.1016/S0140-6736(16)32569-7. Epub 2016 Dec 16. Lancet. 2017. PMID: 27989559 No abstract available.
Comment on
-
Global Burden of Disease Study 2015 provides GPS for global health 2030.Lancet. 2016 Oct 8;388(10053):1448-1449. doi: 10.1016/S0140-6736(16)31743-3. Lancet. 2016. PMID: 27733278 No abstract available.
-
Longer lives and unfinished agendas on child survival.Lancet. 2016 Oct 8;388(10053):1450-1452. doi: 10.1016/S0140-6736(16)31744-5. Lancet. 2016. PMID: 27733279 No abstract available.
Similar articles
-
Global, regional, and national age-sex specific mortality for 264 causes of death, 1980-2016: a systematic analysis for the Global Burden of Disease Study 2016.Lancet. 2017 Sep 16;390(10100):1151-1210. doi: 10.1016/S0140-6736(17)32152-9. Lancet. 2017. PMID: 28919116 Free PMC article.
-
Global, regional, and national age-sex-specific mortality for 282 causes of death in 195 countries and territories, 1980-2017: a systematic analysis for the Global Burden of Disease Study 2017.Lancet. 2018 Nov 10;392(10159):1736-1788. doi: 10.1016/S0140-6736(18)32203-7. Epub 2018 Nov 8. Lancet. 2018. PMID: 30496103 Free PMC article.
-
Forecasting life expectancy, years of life lost, and all-cause and cause-specific mortality for 250 causes of death: reference and alternative scenarios for 2016-40 for 195 countries and territories.Lancet. 2018 Nov 10;392(10159):2052-2090. doi: 10.1016/S0140-6736(18)31694-5. Epub 2018 Oct 16. Lancet. 2018. PMID: 30340847 Free PMC article.
-
Excess Mortality from Mental, Neurological, and Substance Use Disorders in the Global Burden of Disease Study 2010.In: Patel V, Chisholm D, Dua T, Laxminarayan R, Medina-Mora ME, editors. Mental, Neurological, and Substance Use Disorders: Disease Control Priorities, Third Edition (Volume 4). Washington (DC): The International Bank for Reconstruction and Development / The World Bank; 2016 Mar 14. Chapter 3. In: Patel V, Chisholm D, Dua T, Laxminarayan R, Medina-Mora ME, editors. Mental, Neurological, and Substance Use Disorders: Disease Control Priorities, Third Edition (Volume 4). Washington (DC): The International Bank for Reconstruction and Development / The World Bank; 2016 Mar 14. Chapter 3. PMID: 27227239 Free Books & Documents. Review.
-
Global, regional, and national incidence, prevalence, and years lived with disability for 301 acute and chronic diseases and injuries in 188 countries, 1990-2013: a systematic analysis for the Global Burden of Disease Study 2013.Lancet. 2015 Aug 22;386(9995):743-800. doi: 10.1016/S0140-6736(15)60692-4. Epub 2015 Jun 7. Lancet. 2015. PMID: 26063472 Free PMC article. Review.
Cited by
-
Particulate Matter-Induced Emerging Health Effects Associated with Oxidative Stress and Inflammation.Antioxidants (Basel). 2024 Oct 17;13(10):1256. doi: 10.3390/antiox13101256. Antioxidants (Basel). 2024. PMID: 39456509 Free PMC article. Review.
-
The economic burden of pneumonia in children under five in Uganda.Vaccine X. 2021 Apr 2;8:100095. doi: 10.1016/j.jvacx.2021.100095. eCollection 2021 Aug. Vaccine X. 2021. PMID: 34036262 Free PMC article.
-
Activity of daily living upon admission is an independent predictor of in-hospital mortality in older patients with community-acquired pneumonia.BMC Infect Dis. 2021 Apr 1;21(1):314. doi: 10.1186/s12879-021-06006-w. BMC Infect Dis. 2021. PMID: 33794779 Free PMC article.
-
Mortality and Lithium-Protective Effects after First-Episode Mania Diagnosis in Bipolar Disorder: A Nationwide Retrospective Cohort Study in Taiwan.Psychother Psychosom. 2024;93(1):36-45. doi: 10.1159/000535777. Epub 2024 Jan 9. Psychother Psychosom. 2024. PMID: 38194936 Free PMC article.
-
Febrile Illness Evaluation in a Broad Range of Endemicities (FIEBRE): protocol for a multisite prospective observational study of the causes of fever in Africa and Asia.BMJ Open. 2020 Jul 21;10(7):e035632. doi: 10.1136/bmjopen-2019-035632. BMJ Open. 2020. PMID: 32699131 Free PMC article.
References
-
- Roulson J, Benbow EW, Hasleton PS. Discrepancies between clinical and autopsy diagnosis and the value of post mortem histology; a meta-analysis and review. Histopathology. 2005;47:551–559. - PubMed
Publication types
MeSH terms
Grants and funding
- welcome trust/International
- MR/K00669X/1/MRC_/Medical Research Council/United Kingdom
- P30 AG047845/AG/NIA NIH HHS/United States
- MC_PC_13043/MRC_/Medical Research Council/United Kingdom
- MR/K006525/1/MRC_/Medical Research Council/United Kingdom
- MC_U147585827/MRC_/Medical Research Council/United Kingdom
- WT_/Wellcome Trust/United Kingdom
- MC_U137686858/MRC_/Medical Research Council/United Kingdom
- L30 CA130678/CA/NCI NIH HHS/United States
- 095066/WT_/Wellcome Trust/United Kingdom
- G0400491/MRC_/Medical Research Council/United Kingdom
- MC_U147585819/MRC_/Medical Research Council/United Kingdom
- MC_UU_12011/1/MRC_/Medical Research Council/United Kingdom
- 201900/WT_/Wellcome Trust/United Kingdom
- K99 CA201542/CA/NCI NIH HHS/United States
- MC_UP_A620_1014/MRC_/Medical Research Council/United Kingdom
- R43 FD006302/FD/FDA HHS/United States
- NIHR/CS/010/014/DH_/Department of Health/United Kingdom
- RP-PG-0407-10184/DH_/Department of Health/United Kingdom
- MC_U147585824/MRC_/Medical Research Council/United Kingdom
LinkOut - more resources
Full Text Sources
Other Literature Sources
Miscellaneous
