

Long-term findings from COMFORT-II, a phase 3 study of ruxolitinib vs best available therapy for myelofibrosis
- PMID: 27211272
- PMCID: PMC5399157
- DOI: 10.1038/leu.2016.148
Long-term findings from COMFORT-II, a phase 3 study of ruxolitinib vs best available therapy for myelofibrosis
Erratum in
-
Long-term findings from COMFORT-II, a phase 3 study of ruxolitinib vs best available therapy for myelofibrosis.Leukemia. 2017 Mar;31(3):775. doi: 10.1038/leu.2016.323. Leukemia. 2017. PMID: 28248313 Free PMC article. No abstract available.
Abstract
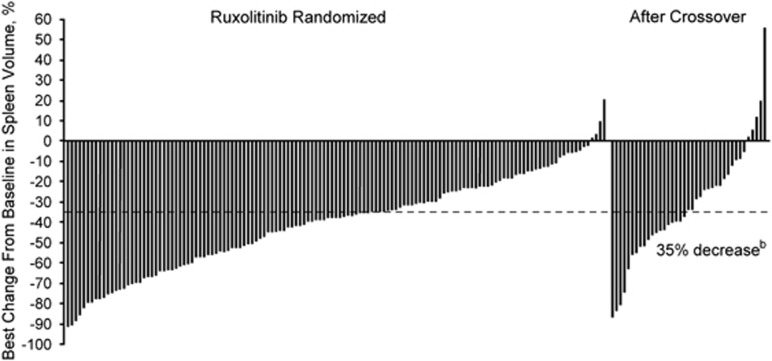
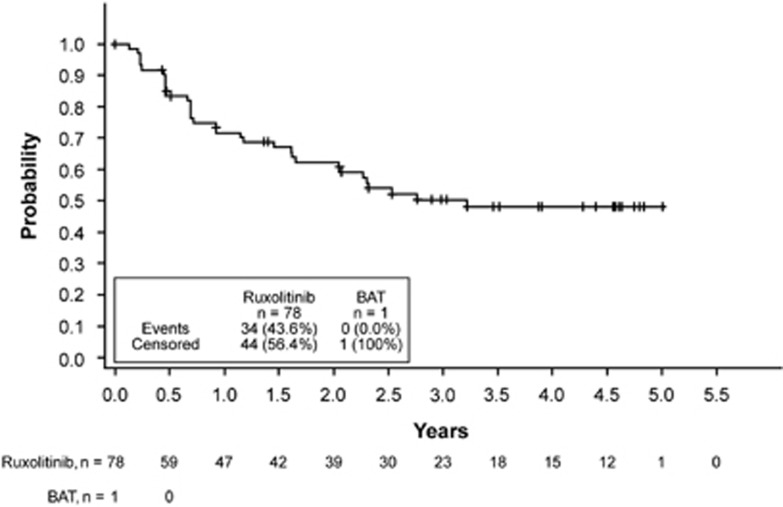
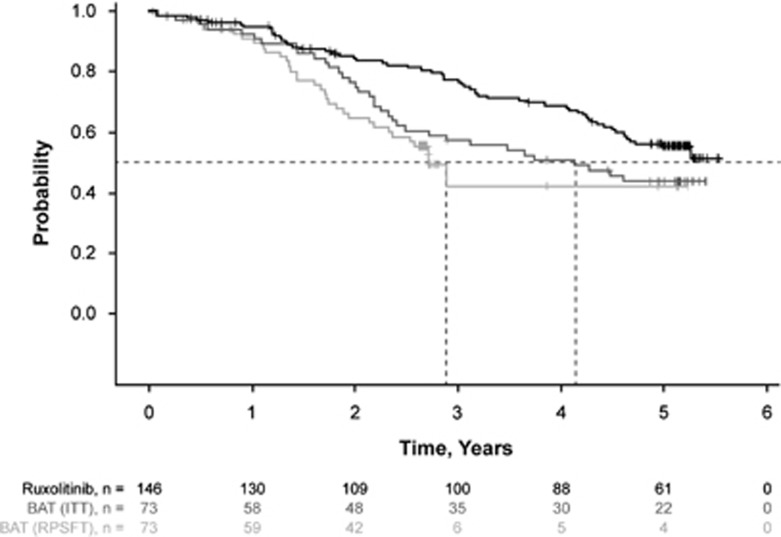
Ruxolitinib is a Janus kinase (JAK) (JAK1/JAK2) inhibitor that has demonstrated superiority over placebo and best available therapy (BAT) in the Controlled Myelofibrosis Study with Oral JAK Inhibitor Treatment (COMFORT) studies. COMFORT-II was a randomized (2:1), open-label phase 3 study in patients with myelofibrosis; patients randomized to BAT could crossover to ruxolitinib upon protocol-defined disease progression or after the primary end point, confounding long-term comparisons. At week 48, 28% (41/146) of patients randomized to ruxolitinib achieved ⩾35% decrease in spleen volume (primary end point) compared with no patients on BAT (P<0.001). Among the 78 patients (53.4%) in the ruxolitinib arm who achieved ⩾35% reductions in spleen volume at any time, the probability of maintaining response was 0.48 (95% confidence interval (CI), 0.35-0.60) at 5 years (median, 3.2 years). Median overall survival was not reached in the ruxolitinib arm and was 4.1 years in the BAT arm. There was a 33% reduction in risk of death with ruxolitinib compared with BAT by intent-to-treat analysis (hazard ratio (HR)=0.67; 95% CI, 0.44-1.02; P=0.06); the crossover-corrected HR was 0.44 (95% CI, 0.18-1.04; P=0.06). There was no unexpected increased incidence of adverse events with longer exposure. This final analysis showed that spleen volume reductions with ruxolitinib were maintained with continued therapy and may be associated with survival benefits.
Conflict of interest statement
CNH has received research support from Novartis, Cell Therapeutics, Gilead and Baxaltra through the institution; has received personal fees from Novartis, Shire, Gilead and Baxaltra; and has received grant and non-financial support from Novartis outside the submitted work. AMV has received grant and personal fees from Novartis during the conduct of the study. J-JK has received travel grant, and research funding paid to the institution from Novartis; has acted as a consultant to Novartis and Incyte. HKA-A has received research funding from Novartis and Celgene; acted as a consultant to Novartis; and has received honoraria from Novartis and Celgene. HG has received honoraria from Novartis, Celgene and AOP Orphan Pharmaceuticals; and has two licensed patents: EP 13.18.6939.8 and 13.18.4632.1. FC has received personal fees from Novartis, CTI-Baxter and Sanofi. MMJ and KS are employees of Incyte. MM and VS are employees of and own stock in Novartis. PG is an employee of Novartis.
Figures
Similar articles
-
A pooled analysis of overall survival in COMFORT-I and COMFORT-II, 2 randomized phase III trials of ruxolitinib for the treatment of myelofibrosis.Haematologica. 2015 Sep;100(9):1139-45. doi: 10.3324/haematol.2014.119545. Epub 2015 Jun 11. Haematologica. 2015. PMID: 26069290 Free PMC article. Clinical Trial.
-
Long-term treatment with ruxolitinib for patients with myelofibrosis: 5-year update from the randomized, double-blind, placebo-controlled, phase 3 COMFORT-I trial.J Hematol Oncol. 2017 Feb 22;10(1):55. doi: 10.1186/s13045-017-0417-z. J Hematol Oncol. 2017. PMID: 28228106 Free PMC article. Clinical Trial.
-
Three-year efficacy, safety, and survival findings from COMFORT-II, a phase 3 study comparing ruxolitinib with best available therapy for myelofibrosis.Blood. 2013 Dec 12;122(25):4047-53. doi: 10.1182/blood-2013-02-485888. Epub 2013 Oct 30. Blood. 2013. PMID: 24174625 Clinical Trial.
-
Ruxolitinib for the treatment of myelofibrosis: a NICE single technology appraisal.Pharmacoeconomics. 2013 Oct;31(10):841-52. doi: 10.1007/s40273-013-0083-0. Pharmacoeconomics. 2013. PMID: 23996108 Review.
-
Ruxolitinib for myelofibrosis--an update of its clinical effects.Clin Lymphoma Myeloma Leuk. 2013 Dec;13(6):638-45. doi: 10.1016/j.clml.2013.09.006. Epub 2013 Oct 2. Clin Lymphoma Myeloma Leuk. 2013. PMID: 24238036 Free PMC article. Review.
Cited by
-
JAK2 in Myeloproliferative Neoplasms: Still a Protagonist.Pharmaceuticals (Basel). 2022 Jan 28;15(2):160. doi: 10.3390/ph15020160. Pharmaceuticals (Basel). 2022. PMID: 35215273 Free PMC article. Review.
-
Addition of Navitoclax to Ongoing Ruxolitinib Therapy for Patients With Myelofibrosis With Progression or Suboptimal Response: Phase II Safety and Efficacy.J Clin Oncol. 2022 May 20;40(15):1671-1680. doi: 10.1200/JCO.21.02188. Epub 2022 Feb 18. J Clin Oncol. 2022. PMID: 35180010 Free PMC article. Clinical Trial.
-
Targeting few to help hundreds: JAK, MAPK and ROCK pathways as druggable targets in atypical chronic myeloid leukemia.Mol Cancer. 2018 Feb 19;17(1):40. doi: 10.1186/s12943-018-0774-4. Mol Cancer. 2018. PMID: 29455651 Free PMC article. Review.
-
Long-term effects of ruxolitinib versus best available therapy on bone marrow fibrosis in patients with myelofibrosis.J Hematol Oncol. 2018 Mar 15;11(1):42. doi: 10.1186/s13045-018-0585-5. J Hematol Oncol. 2018. PMID: 29544547 Free PMC article.
-
Management of myelofibrosis after ruxolitinib failure.Leuk Lymphoma. 2020 Aug;61(8):1797-1809. doi: 10.1080/10428194.2020.1749606. Epub 2020 Apr 16. Leuk Lymphoma. 2020. PMID: 32297800 Free PMC article.
References
-
- Vannucchi AM. Management of myelofibrosis. Hematol Am Soc Hematol Educ Program 2011; 2011: 222–230. - PubMed
-
- Vainchenker W, Delhommeau F, Constantinescu SN, Bernard OA. New mutations and pathogenesis of myeloproliferative neoplasms. Blood 2011; 188: 1723–1735. - PubMed
-
- Cervantes F, Dupriez B, Pereira A, PassamontiF, Reilly JT, Morra E et al. New prognostic scoring system for primary myelofibrosis based on a study of the International Working Group for Myelofibrosis Research and Treatment. Blood 2009; 113: 2895–2901. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Research Materials
Miscellaneous
