

Cancer Stem Cell Plasticity Drives Therapeutic Resistance
- PMID: 26742077
- PMCID: PMC4728455
- DOI: 10.3390/cancers8010008
Cancer Stem Cell Plasticity Drives Therapeutic Resistance
Abstract
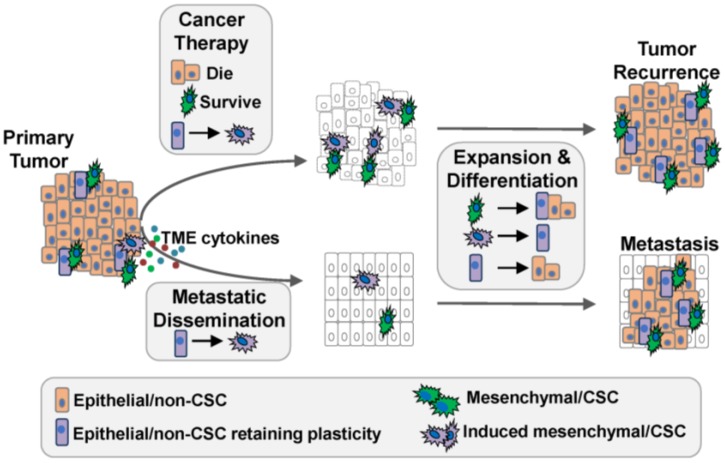
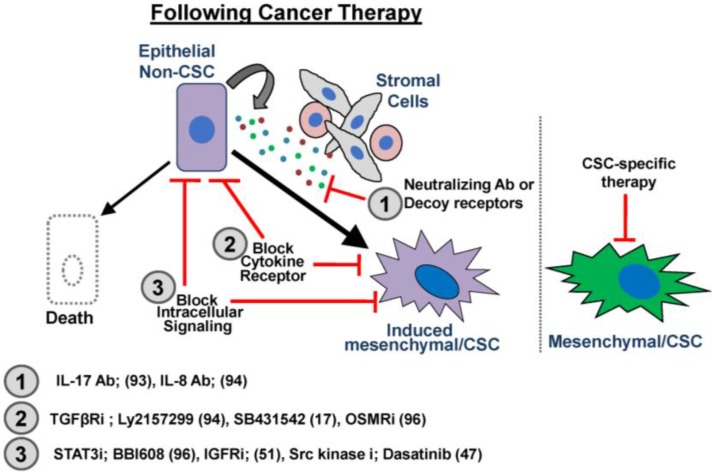
The connection between epithelial-mesenchymal (E-M) plasticity and cancer stem cell (CSC) properties has been paradigm-shifting, linking tumor cell invasion and metastasis with therapeutic recurrence. However, despite their importance, the molecular pathways involved in generating invasive, metastatic, and therapy-resistant CSCs remain poorly understood. The enrichment of cells with a mesenchymal/CSC phenotype following therapy has been interpreted in two different ways. The original interpretation posited that therapy kills non-CSCs while sparing pre-existing CSCs. However, evidence is emerging that suggests non-CSCs can be induced into a transient, drug-tolerant, CSC-like state by chemotherapy. The ability to transition between distinct cell states may be as critical for the survival of tumor cells following therapy as it is for metastatic progression. Therefore, inhibition of the pathways that promote E-M and CSC plasticity may suppress tumor recurrence following chemotherapy. Here, we review the emerging appreciation for how plasticity confers therapeutic resistance and tumor recurrence.
Keywords: cancer stem cells; cellular plasticity; cytokines; epithelial-mesenchymal; therapeutic resistance; tumor microenvironment.
Figures
Similar articles
-
Linking Tumor Microenvironment to Plasticity of Cancer Stem Cells: Mechanisms and Application in Cancer Therapy.Front Oncol. 2021 Jun 28;11:678333. doi: 10.3389/fonc.2021.678333. eCollection 2021. Front Oncol. 2021. PMID: 34262865 Free PMC article. Review.
-
Epithelial-to-mesenchymal plasticity of cancer stem cells: therapeutic targets in hepatocellular carcinoma.J Hematol Oncol. 2016 Aug 30;9(1):74. doi: 10.1186/s13045-016-0307-9. J Hematol Oncol. 2016. PMID: 27578206 Free PMC article. Review.
-
Cancer Stem Cell Plasticity - A Deadly Deal.Front Mol Biosci. 2020 Apr 30;7:79. doi: 10.3389/fmolb.2020.00079. eCollection 2020. Front Mol Biosci. 2020. PMID: 32426371 Free PMC article. Review.
-
Cancer stem-like cells enriched with CD29 and CD44 markers exhibit molecular characteristics with epithelial-mesenchymal transition in squamous cell carcinoma.Arch Dermatol Res. 2013 Jan;305(1):35-47. doi: 10.1007/s00403-012-1260-2. Epub 2012 Jun 28. Arch Dermatol Res. 2013. PMID: 22740085
-
Cellular Plasticity-Targeted Therapy in Head and Neck Cancers.J Dent Res. 2018 Jun;97(6):654-664. doi: 10.1177/0022034518756351. Epub 2018 Feb 27. J Dent Res. 2018. PMID: 29486673 Review.
Cited by
-
LATS1 and LATS2 suppress breast cancer progression by maintaining cell identity and metabolic state.Life Sci Alliance. 2018 Oct 30;1(5):e201800171. doi: 10.26508/lsa.201800171. eCollection 2018 Oct. Life Sci Alliance. 2018. PMID: 30456386 Free PMC article.
-
Cellular, transcriptomic and isoform heterogeneity of breast cancer cell line revealed by full-length single-cell RNA sequencing.Comput Struct Biotechnol J. 2020 Mar 19;18:676-685. doi: 10.1016/j.csbj.2020.03.005. eCollection 2020. Comput Struct Biotechnol J. 2020. PMID: 32257051 Free PMC article.
-
The Role of the Renin-Angiotensin System in the Cancer Stem Cell Niche.J Histochem Cytochem. 2021 Dec;69(12):835-847. doi: 10.1369/00221554211026295. Epub 2021 Jun 24. J Histochem Cytochem. 2021. PMID: 34165363 Free PMC article. Review.
-
Wnt/β-Catenin Pathway Activation Mediates Adaptive Resistance to BRAF Inhibition in Colorectal Cancer.Mol Cancer Ther. 2018 Apr;17(4):806-813. doi: 10.1158/1535-7163.MCT-17-0561. Epub 2017 Nov 22. Mol Cancer Ther. 2018. PMID: 29167314 Free PMC article.
-
Emerging role of tumor cell plasticity in modifying therapeutic response.Signal Transduct Target Ther. 2020 Oct 7;5(1):228. doi: 10.1038/s41392-020-00313-5. Signal Transduct Target Ther. 2020. PMID: 33028808 Free PMC article. Review.
References
-
- Guarneri V., Broglio K., Kau S.W., Cristofanilli M., Buzdar A.U., Valero V., Buchholz T., Meric F., Middleton L., Hortobagyi G.N., et al. Prognostic value of pathologic complete response after primary chemotherapy in relation to hormone receptor status and other factors. J. Clin. Oncol. 2006;24:1037–1044. doi: 10.1200/JCO.2005.02.6914. - DOI - PubMed
-
- Kuerer H.M., Newman L.A., Smith T.L., Ames F.C., Hunt K.K., Dhingra K., Theriault R.L., Singh G., Binkley S.M., Sneige N., et al. Clinical course of breast cancer patients with complete pathologic primary tumor and axillary lymph node response to doxorubicin-based neoadjuvant chemotherapy. J. Clin. Oncol. 1999;17:460–469. - PubMed
-
- Liedtke C., Mazouni C., Hess K.R., Andre F., Tordai A., Mejia J.A., Symmans W.F., Gonzalez-Angulo A.M., Hennessy B., Green M., et al. Response to neoadjuvant therapy and long-term survival in patients with triple-negative breast cancer. J. Clin. Oncol. 2008;26:1275–1281. doi: 10.1200/JCO.2007.14.4147. - DOI - PubMed
Publication types
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
