

Clinical Features and Outcomes of Patients With Symptomatic Kaposi Sarcoma Herpesvirus (KSHV)-associated Inflammation: Prospective Characterization of KSHV Inflammatory Cytokine Syndrome (KICS)
- PMID: 26658701
- PMCID: PMC4772848
- DOI: 10.1093/cid/civ996
Clinical Features and Outcomes of Patients With Symptomatic Kaposi Sarcoma Herpesvirus (KSHV)-associated Inflammation: Prospective Characterization of KSHV Inflammatory Cytokine Syndrome (KICS)
Erratum in
-
Erratum.Clin Infect Dis. 2018 Mar 5;66(6):985. doi: 10.1093/cid/cix831. Clin Infect Dis. 2018. PMID: 29370384 Free PMC article. No abstract available.
Abstract
Background: Kaposi sarcoma herpesvirus (KSHV) is the cause of Kaposi sarcoma (KS), primary effusion lymphoma (PEL), and a form of Castleman disease (KSHV-MCD). Recently a KSHV-associated inflammatory cytokine syndrome (KICS) distinct from KSHV-MCD was reported.
Methods: We prospectively characterized the clinical, laboratory, virologic and immunologic features of KICS by evaluating symptomatic adults with KSHV using a prespecified definition. These features and overall survival were compared with controls from 2 prospectively characterized human immunodeficiency virus (HIV)-infected cohorts, including 1 with KSHV coinfection.
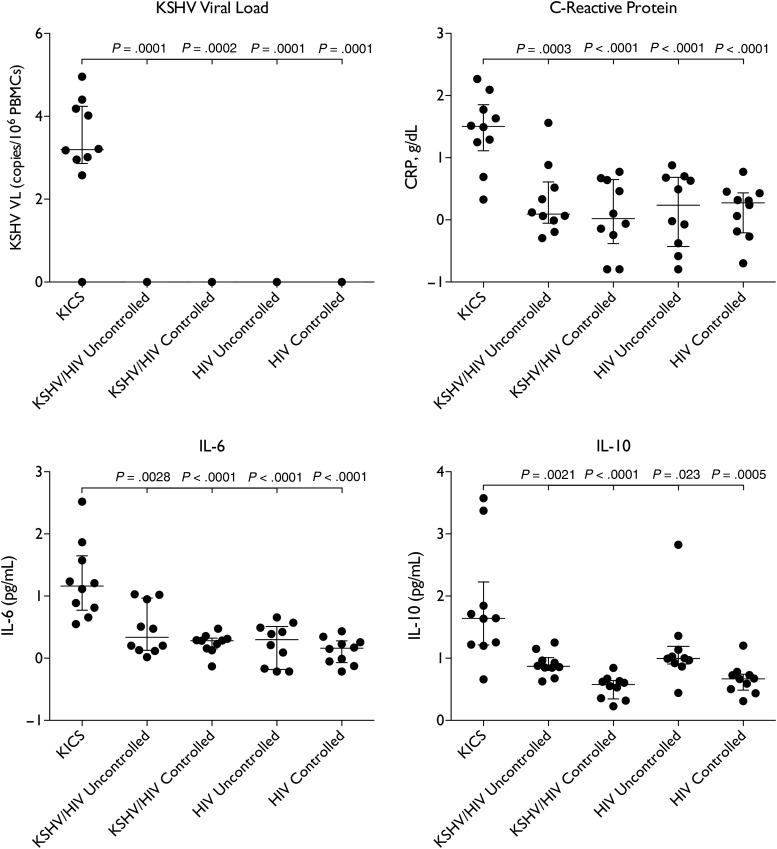
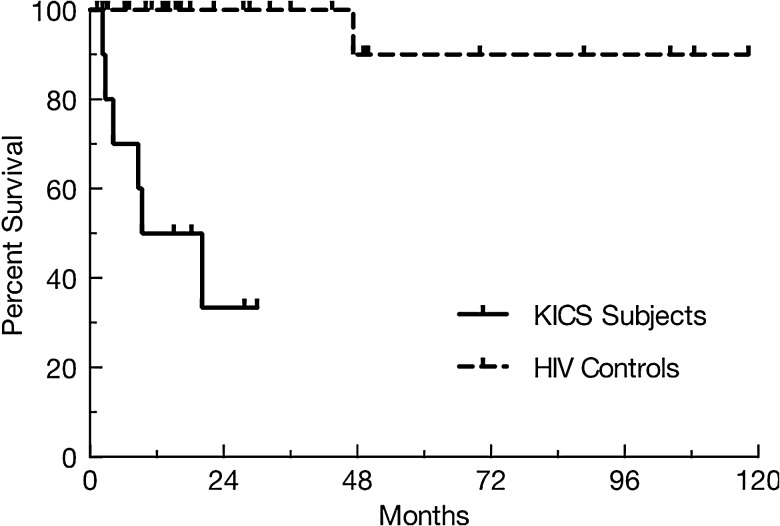
Results: All 10 KICS subjects were HIV infected males; 5 had HIV viral load (VL) suppressed <50 copies mL (median 72, range <50-74 375); all had KS and 2 also had PEL. All had multiple severe symptoms attributable to KICS: median number of symptoms 8 (6-11), median grade of worst symptom 3 (2-4). These included gastrointestinal disturbance (present in 9); edema (9); respiratory (6); and effusions (5). Laboratory abnormalities included anemia (all); hypoalbuminemia (all) and thrombocytopenia (6). None developed KSHV-MCD; 6 died with median survival from KICS diagnosis 13.6 months. KICS subjects compared with controls had more severe symptoms; lower hemoglobin and albumin; higher C-reactive protein; higher KSHV VL; elevated interleukin (IL)-6 and IL-10; and an increased risk of death (all P < .05). Anemia and hypoalbuminemia at presentation were independently associated with early death.
Conclusions: KICS subjects demonstrated diverse severe symptoms, a high rate of KSHV-associated tumors, high mortality, and a distinct IL-6/IL-10 signature. KICS may be an important unrecognized cause of morbidity and mortality, including symptoms previously ascribed to HIV. Exploration of KSHV-directed therapy is warranted.
Keywords: HIV; Human Herpesvirus 8 (HHV-8); IL-10; IL-6; Kaposi sarcoma herpesvirus (KSHV).
Published by Oxford University Press for the Infectious Diseases Society of America 2015. This work is written by (a) US Government employee(s) and is in the public domain in the US.
Figures

Similar articles
-
A Fatal Case of Kaposi Sarcoma Immune Reconstitution Syndrome (KS-IRIS) Complicated by Kaposi Sarcoma Inflammatory Cytokine Syndrome (KICS) or Multicentric Castleman Disease (MCD): A Case Report and Review.Am J Case Rep. 2020 Dec 3;21:e926433. doi: 10.12659/AJCR.926433. Am J Case Rep. 2020. PMID: 33268763 Free PMC article. Review.
-
Elevated IL-13 in effusions of patients with HIV and primary effusion lymphoma as compared with other Kaposi sarcoma herpesvirus-associated disorders.AIDS. 2021 Jan 1;35(1):53-62. doi: 10.1097/QAD.0000000000002692. AIDS. 2021. PMID: 33273183 Free PMC article.
-
An interleukin-6-related systemic inflammatory syndrome in patients co-infected with Kaposi sarcoma-associated herpesvirus and HIV but without Multicentric Castleman disease.Clin Infect Dis. 2010 Aug 1;51(3):350-8. doi: 10.1086/654798. Clin Infect Dis. 2010. PMID: 20583924 Free PMC article.
-
Inflammasome activation in patients with Kaposi sarcoma herpesvirus-associated diseases.Blood. 2024 Oct 3;144(14):1496-1507. doi: 10.1182/blood.2024024144. Blood. 2024. PMID: 38941593 Free PMC article.
-
KSHV-associated multicentric Castleman disease: A tangle of different entities requiring multitarget treatment strategies.Int J Cancer. 2015 Jul 15;137(2):251-61. doi: 10.1002/ijc.28923. Epub 2014 May 5. Int J Cancer. 2015. PMID: 24771491 Review.
Cited by
-
Evidence for altered host genetic factors in KSHV infection and KSHV-related disease development.Rev Med Virol. 2021 Mar;31(2):e2160. doi: 10.1002/rmv.2160. Epub 2020 Oct 11. Rev Med Virol. 2021. PMID: 33043529 Free PMC article. Review.
-
Case report: Multicentric Castleman disease as a manifestation of immune reconstitution inflammatory syndrome in Malawi.Front Oncol. 2022 Dec 12;12:969135. doi: 10.3389/fonc.2022.969135. eCollection 2022. Front Oncol. 2022. PMID: 36578926 Free PMC article.
-
Insight into the Epigenetics of Kaposi's Sarcoma-Associated Herpesvirus.Int J Mol Sci. 2023 Oct 6;24(19):14955. doi: 10.3390/ijms241914955. Int J Mol Sci. 2023. PMID: 37834404 Free PMC article. Review.
-
Activation and Evasion of Innate Immunity by Gammaherpesviruses.J Mol Biol. 2022 Mar 30;434(6):167214. doi: 10.1016/j.jmb.2021.167214. Epub 2021 Aug 23. J Mol Biol. 2022. PMID: 34437888 Free PMC article. Review.
-
A Fatal Case of Kaposi Sarcoma Immune Reconstitution Syndrome (KS-IRIS) Complicated by Kaposi Sarcoma Inflammatory Cytokine Syndrome (KICS) or Multicentric Castleman Disease (MCD): A Case Report and Review.Am J Case Rep. 2020 Dec 3;21:e926433. doi: 10.12659/AJCR.926433. Am J Case Rep. 2020. PMID: 33268763 Free PMC article. Review.
References
-
- Chang Y, Cesarman E, Pessin MS et al. . Identification of herpesvirus-like DNA sequences in AIDS-associated Kaposi's sarcoma. Science 1994; 266:1865–9. - PubMed
-
- Cesarman E, Chang Y, Moore PS, Said JW, Knowles DM. Kaposi's sarcoma-associated herpesvirus-like DNA sequences in AIDS-related body-cavity-based lymphomas. N Engl J Med 1995; 332:1186–91. - PubMed
-
- Soulier J, Grollet L, Oksenhendler E et al. . Kaposi's sarcoma-associated herpesvirus-like DNA sequences in multicentric Castleman's disease. Blood 1995; 86:1276–80. - PubMed
-
- Aoki Y, Tosato G, Fonville TW, Pittaluga S. Serum viral interleukin-6 in AIDS-related multicentric Castleman disease. Blood 2001; 97:2526. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
