

Cumulative Incidence of Cancer Among Persons With HIV in North America: A Cohort Study
- PMID: 26436616
- PMCID: PMC4711936
- DOI: 10.7326/M14-2768
Cumulative Incidence of Cancer Among Persons With HIV in North America: A Cohort Study
Abstract
Background: Cancer is increasingly common among persons with HIV.
Objective: To examine calendar trends in cumulative cancer incidence and hazard rate by HIV status.
Design: Cohort study.
Setting: North American AIDS Cohort Collaboration on Research and Design during 1996 to 2009.
Participants: 86 620 persons with HIV and 196 987 uninfected adults.
Measurements: Cancer type-specific cumulative incidence by age 75 years and calendar trends in cumulative incidence and hazard rates, each by HIV status.
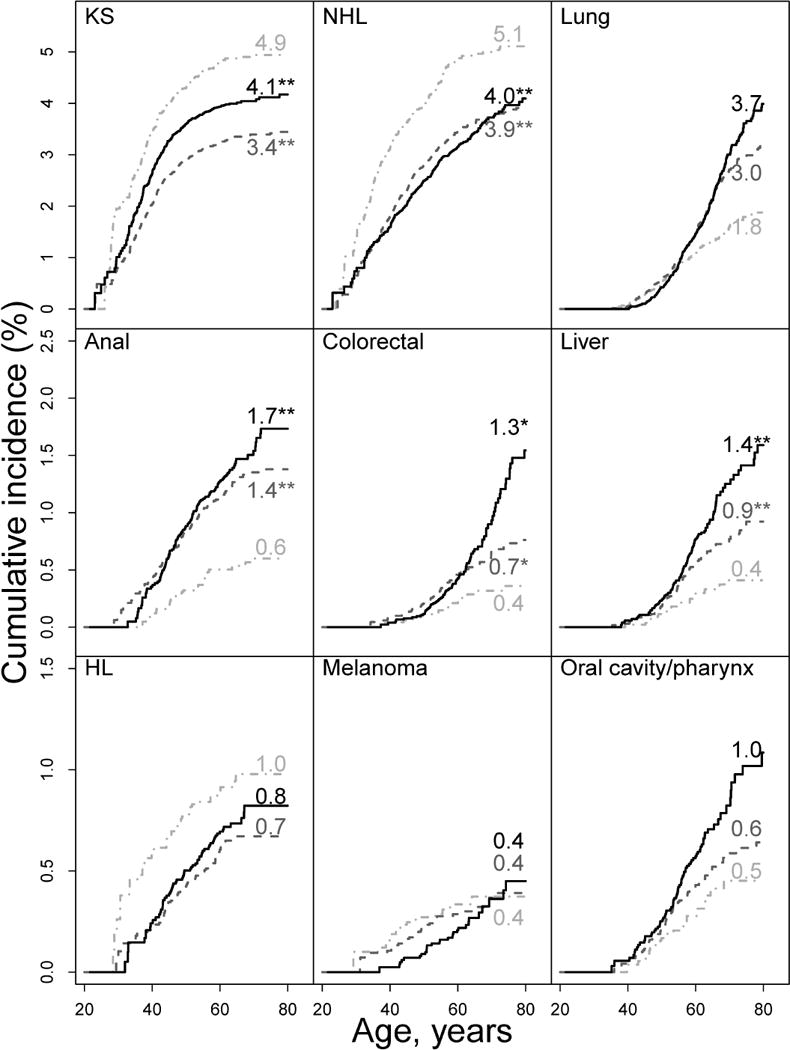
Results: Cumulative incidences of cancer by age 75 years for persons with and without HIV, respectively, were as follows: Kaposi sarcoma, 4.4% and 0.01%; non-Hodgkin lymphoma, 4.5% and 0.7%; lung cancer, 3.4% and 2.8%; anal cancer, 1.5% and 0.05%; colorectal cancer, 1.0% and 1.5%; liver cancer, 1.1% and 0.4%; Hodgkin lymphoma, 0.9% and 0.09%; melanoma, 0.5% and 0.6%; and oral cavity/pharyngeal cancer, 0.8% and 0.8%. Among persons with HIV, calendar trends in cumulative incidence and hazard rate decreased for Kaposi sarcoma and non-Hodgkin lymphoma. For anal, colorectal, and liver cancer, increasing cumulative incidence, but not hazard rate trends, were due to the decreasing mortality rate trend (-9% per year), allowing greater opportunity to be diagnosed. Despite decreasing hazard rate trends for lung cancer, Hodgkin lymphoma, and melanoma, cumulative incidence trends were not seen because of the compensating effect of the declining mortality rate.
Limitation: Secular trends in screening, smoking, and viral co-infections were not evaluated.
Conclusion: Cumulative cancer incidence by age 75 years, approximating lifetime risk in persons with HIV, may have clinical utility in this population. The high cumulative incidences by age 75 years for Kaposi sarcoma, non-Hodgkin lymphoma, and lung cancer support early and sustained antiretroviral therapy and smoking cessation.
Figures

Comment in
-
Older patients with HIV should be offered cancer screening, study recommends.BMJ. 2015 Oct 5;351:h5262. doi: 10.1136/bmj.h5262. BMJ. 2015. PMID: 26443627 No abstract available.
Similar articles
-
Cancer risk in the Swiss HIV Cohort Study: associations with immunodeficiency, smoking, and highly active antiretroviral therapy.J Natl Cancer Inst. 2005 Mar 16;97(6):425-32. doi: 10.1093/jnci/dji072. J Natl Cancer Inst. 2005. PMID: 15770006
-
Cancer risk in HIV-infected people in the USA from 1996 to 2012: a population-based, registry-linkage study.Lancet HIV. 2017 Nov;4(11):e495-e504. doi: 10.1016/S2352-3018(17)30125-X. Epub 2017 Aug 10. Lancet HIV. 2017. PMID: 28803888 Free PMC article.
-
Trends and risk of lung cancer among people living with HIV in the USA: a population-based registry linkage study.Lancet HIV. 2022 Oct;9(10):e700-e708. doi: 10.1016/S2352-3018(22)00219-3. Lancet HIV. 2022. PMID: 36179753 Free PMC article.
-
Epidemiology of HIV-associated malignancies.Cancer Treat Res. 2001;104:1-18. doi: 10.1007/978-1-4615-1601-9_1. Cancer Treat Res. 2001. PMID: 11191124 Review. No abstract available.
-
Human immunodeficiency virus infection, aging, and cancer.J Clin Epidemiol. 2001 Dec;54 Suppl 1:S29-34. doi: 10.1016/s0895-4356(01)00444-9. J Clin Epidemiol. 2001. PMID: 11750207 Review.
Cited by
-
Comparison of anal pre-cancer screening strategies among men who have sex with men.Int J STD AIDS. 2023 Feb;34(2):87-97. doi: 10.1177/09564624221137974. Epub 2022 Nov 15. Int J STD AIDS. 2023. PMID: 36380689 Free PMC article.
-
Evaluation of mean corpuscular volume among anemic people with HIV in North America following ART initiation.AIDS Res Ther. 2024 Aug 7;21(1):52. doi: 10.1186/s12981-024-00641-4. AIDS Res Ther. 2024. PMID: 39113038 Free PMC article.
-
Understanding the role of Toll-like receptors in lung cancer immunity and immunotherapy.Front Immunol. 2022 Oct 31;13:1033483. doi: 10.3389/fimmu.2022.1033483. eCollection 2022. Front Immunol. 2022. PMID: 36389785 Free PMC article. Review.
-
Evidence for Persistent Monocyte and Immune Dysregulation After Prolonged Viral Suppression Despite Normalization of Monocyte Subsets, sCD14 and sCD163 in HIV-Infected Individuals.Pathog Immun. 2019 Dec 17;4(2):324-362. doi: 10.20411/pai.v4i2.336. eCollection 2019. Pathog Immun. 2019. PMID: 31893252 Free PMC article.
-
Comparing Cancer Incidence in an Observational Cohort of Medicaid Beneficiaries With and Without HIV, 2001-2015.J Acquir Immune Defic Syndr. 2024 Jan 1;95(1):26-34. doi: 10.1097/QAI.0000000000003318. J Acquir Immune Defic Syndr. 2024. PMID: 37831615 Free PMC article.
References
-
- Wada N, Jacobson LP, Cohen M, French A, Phair J, Munoz A. Cause-specific life expectancies after 35 years of age for human immunodeficiency syndrome-infected and human immunodeficiency syndrome-negative individuals followed simultaneously in long-term cohort studies, 1984–2008. Am J Epidemiol. 2013;177(2):116–25. - PMC - PubMed
-
- Justice AC. HIV and aging: time for a new paradigm. Curr HIV/AIDS Rep. 2010;7(2):69–76. - PubMed
-
- Guiguet M, Boue F, Cadranel J, Lang JM, Rosenthal E, Costagliola D. Effect of immunodeficiency, HIV viral load, and antiretroviral therapy on the risk of individual malignancies (FHDH-ANRS CO4): a prospective cohort study. Lancet Oncol. 2009;10(12):1152–9. - PubMed
Publication types
MeSH terms
Grants and funding
- R56 DA004334/DA/NIDA NIH HHS/United States
- U01 DA036935/DA/NIDA NIH HHS/United States
- U01 AI038855/AI/NIAID NIH HHS/United States
- ZIA CP010214-06/ImNIH/Intramural NIH HHS/United States
- U01-AI34989/AI/NIAID NIH HHS/United States
- P30 AI027767/AI/NIAID NIH HHS/United States
- U01 AI035042/AI/NIAID NIH HHS/United States
- U01 DA036297/DA/NIDA NIH HHS/United States
- R01 AA016893/AA/NIAAA NIH HHS/United States
- R01-CA165937/CA/NCI NIH HHS/United States
- U01-AI38855/AI/NIAID NIH HHS/United States
- CBR-86906/CAPMC/ CIHR/Canada
- P30 MH062246/MH/NIMH NIH HHS/United States
- R01-AA16893/AA/NIAAA NIH HHS/United States
- U01 AI069434/AI/NIAID NIH HHS/United States
- R24-AI067039/AI/NIAID NIH HHS/United States
- U01 AI037984/AI/NIAID NIH HHS/United States
- Z01 CP010176-08/ImNIH/Intramural NIH HHS/United States
- U01-HD32632/HD/NICHD NIH HHS/United States
- R01 DA011602/DA/NIDA NIH HHS/United States
- K23 EY013707/EY/NEI NIH HHS/United States
- U01-AI34993/AI/NIAID NIH HHS/United States
- P30-MH62246/MH/NIMH NIH HHS/United States
- K23-EY013707/EY/NEI NIH HHS/United States
- R56-AI102622/AI/NIAID NIH HHS/United States
- R01 CA165937/CA/NCI NIH HHS/United States
- TGF-96118/CAPMC/ CIHR/Canada
- U01 AI031834/AI/NIAID NIH HHS/United States
- HCP-97105/CAPMC/ CIHR/Canada
- K01-AI071754/AI/NIAID NIH HHS/United States
- P30 AI094189/AI/NIAID NIH HHS/United States
- U01-AI38858/AI/NIAID NIH HHS/United States
- U01 AI035004/AI/NIAID NIH HHS/United States
- UM1 AI069432/AI/NIAID NIH HHS/United States
- G12 MD007583/MD/NIMHD NIH HHS/United States
- P30 AI054999/AI/NIAID NIH HHS/United States
- R01-DA04334/DA/NIDA NIH HHS/United States
- T32 AI007140/AI/NIAID NIH HHS/United States
- U01-AI35040/AI/NIAID NIH HHS/United States
- U01-AI37984/AI/NIAID NIH HHS/United States
- U10-EY08052/EY/NEI NIH HHS/United States
- U54 MD007587/MD/NIMHD NIH HHS/United States
- R01 DA004334/DA/NIDA NIH HHS/United States
- U01-AI35004/AI/NIAID NIH HHS/United States
- U01-AI68636/AI/NIAID NIH HHS/United States
- UL1 RR024131/RR/NCRR NIH HHS/United States
- P30-AI036219/AI/NIAID NIH HHS/United States
- U01 AI034989/AI/NIAID NIH HHS/United States
- U01-AI68634/AI/NIAID NIH HHS/United States
- U01 AI037613/AI/NIAID NIH HHS/United States
- U01-AI69432/AI/NIAID NIH HHS/United States
- P30-AI094189/AI/NIAID NIH HHS/United States
- UM1 AI068634/AI/NIAID NIH HHS/United States
- U01-AI35042/AI/NIAID NIH HHS/United States
- CBR-94036/CAPMC/ CIHR/Canada
- U54-MD007587/MD/NIMHD NIH HHS/United States
- U01 AI035041/AI/NIAID NIH HHS/United States
- R24 AI067039/AI/NIAID NIH HHS/United States
- U01-AI37613/AI/NIAID NIH HHS/United States
- KL2-TR000421/TR/NCATS NIH HHS/United States
- U01-AI069918/AI/NIAID NIH HHS/United States
- U01-AA013566/AA/NIAAA NIH HHS/United States
- UM1 AI035043/AI/NIAID NIH HHS/United States
- U01 AI069432/AI/NIAID NIH HHS/United States
- U01-AI42590/AI/NIAID NIH HHS/United States
- K01 AI071754/AI/NIAID NIH HHS/United States
- P30-AI50410/AI/NIAID NIH HHS/United States
- N02CP55504/CP/NCI NIH HHS/United States
- U01 AI038858/AI/NIAID NIH HHS/United States
- F31 DA035713/DA/NIDA NIH HHS/United States
- MO1-RR-00052/RR/NCRR NIH HHS/United States
- R01-DA12568/DA/NIDA NIH HHS/United States
- U10 EY008057/EY/NEI NIH HHS/United States
- UL1-RR024131/RR/NCRR NIH HHS/United States
- U01 AI068636/AI/NIAID NIH HHS/United States
- U01-AI31834/AI/NIAID NIH HHS/United States
- U01 AI034994/AI/NIAID NIH HHS/United States
- U01-AI69434/AI/NIAID NIH HHS/United States
- M01 RR000052/RR/NCRR NIH HHS/United States
- Z01-CP010214/CP/NCI NIH HHS/United States
- K24-DA00432/DA/NIDA NIH HHS/United States
- U10 EY008052/EY/NEI NIH HHS/United States
- F31-DA037788/DA/NIDA NIH HHS/United States
- P30-AI27757/AI/NIAID NIH HHS/United States
- U01 AA020790/AA/NIAAA NIH HHS/United States
- K24-AI065298/AI/NIAID NIH HHS/United States
- P30 AI027763/AI/NIAID NIH HHS/United States
- K01 AI093197/AI/NIAID NIH HHS/United States
- U01 AI069918/AI/NIAID NIH HHS/United States
- UL1-TR000083/TR/NCATS NIH HHS/United States
- U01-AA020790/AA/NIAAA NIH HHS/United States
- K24 AI118591/AI/NIAID NIH HHS/United States
- U01-AI35041/AI/NIAID NIH HHS/United States
- U01 AA013566/AA/NIAAA NIH HHS/United States
- U01 AI035043/AI/NIAID NIH HHS/United States
- UL1 TR000083/TR/NCATS NIH HHS/United States
- P30 AI027757/AI/NIAID NIH HHS/United States
- N01RR52085/RR/NCRR NIH HHS/United States
- U01-AI35039/AI/NIAID NIH HHS/United States
- R01 DA012568/DA/NIDA NIH HHS/United States
- U10-EY08067/EY/NEI NIH HHS/United States
- G12- MD007583/MD/NIMHD NIH HHS/United States
- KL2 TR000421/TR/NCATS NIH HHS/United States
- P30-AI27767/AI/NIAID NIH HHS/United States
- U01 AI035040/AI/NIAID NIH HHS/United States
- R56 AI102622/AI/NIAID NIH HHS/United States
- K01-AI093197/AI/NIAID NIH HHS/United States
- U01 AI034993/AI/NIAID NIH HHS/United States
- R01-DA11602/DA/NIDA NIH HHS/United States
- U01-DA036935/DA/NIDA NIH HHS/United States
- U01-AI34994/AI/NIAID NIH HHS/United States
- U01 AI035039/AI/NIAID NIH HHS/United States
- U24-AA020794/AA/NIAAA NIH HHS/United States
- U10-EY08057/EY/NEI NIH HHS/United States
- U10 EY008067/EY/NEI NIH HHS/United States
- P30 AI036219/AI/NIAID NIH HHS/United States
- Z01 CP010176/ImNIH/Intramural NIH HHS/United States
- U24 AA020794/AA/NIAAA NIH HHS/United States
- P30-AI027763/AI/NIAID NIH HHS/United States
- U01 AI068634/AI/NIAID NIH HHS/United States
- P30 AI050410/AI/NIAID NIH HHS/United States
- UM1-AI35043/AI/NIAID NIH HHS/United States
- U01 HD032632/HD/NICHD NIH HHS/United States
- U01 AI042590/AI/NIAID NIH HHS/United States
- P30-AI54999/AI/NIAID NIH HHS/United States