

Mechanism by Which Caloric Restriction Improves Insulin Sensitivity in Sedentary Obese Adults
- PMID: 26324180
- PMCID: PMC4686951
- DOI: 10.2337/db15-0675
Mechanism by Which Caloric Restriction Improves Insulin Sensitivity in Sedentary Obese Adults
Abstract
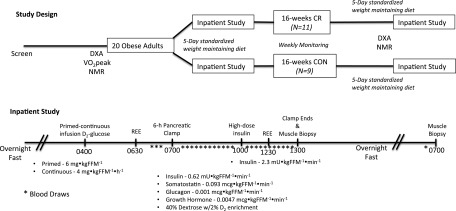
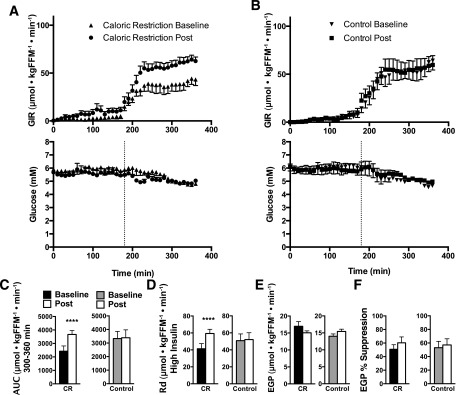
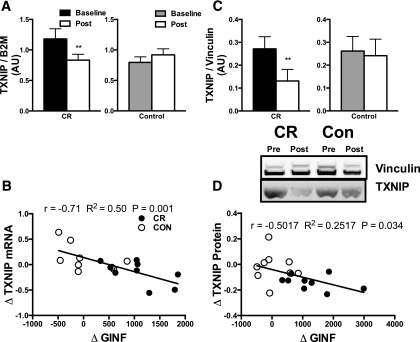
Caloric restriction (CR) improves insulin sensitivity and reduces the incidence of diabetes in obese individuals. The underlying mechanisms whereby CR improves insulin sensitivity are not clear. We evaluated the effect of 16 weeks of CR on whole-body insulin sensitivity by pancreatic clamp before and after CR in 11 obese participants (BMI = 35 kg/m(2)) compared with 9 matched control subjects (BMI = 34 kg/m(2)). Compared with the control subjects, CR increased the glucose infusion rate needed to maintain euglycemia during hyperinsulinemia, indicating enhancement of peripheral insulin sensitivity. This improvement in insulin sensitivity was not accompanied by changes in skeletal muscle mitochondrial oxidative capacity or oxidant emissions, nor were there changes in skeletal muscle ceramide, diacylglycerol, or amino acid metabolite levels. However, CR lowered insulin-stimulated thioredoxin-interacting protein (TXNIP) levels and enhanced nonoxidative glucose disposal. These results support a role for TXNIP in mediating the improvement in peripheral insulin sensitivity after CR.
© 2016 by the American Diabetes Association. Readers may use this article as long as the work is properly cited, the use is educational and not for profit, and the work is not altered.
Figures

Comment in
-
Cutting Calories and TXNIP From the Skeletal Muscle to Restore Insulin Sensitivity.Diabetes. 2016 Jan;65(1):16-8. doi: 10.2337/dbi15-0021. Diabetes. 2016. PMID: 26696635 Free PMC article. No abstract available.
Similar articles
-
Cutting Calories and TXNIP From the Skeletal Muscle to Restore Insulin Sensitivity.Diabetes. 2016 Jan;65(1):16-8. doi: 10.2337/dbi15-0021. Diabetes. 2016. PMID: 26696635 Free PMC article. No abstract available.
-
Effect of gender on lipid-induced insulin resistance in obese subjects.Eur J Endocrinol. 2008 Jan;158(1):61-8. doi: 10.1530/EJE-07-0493. Eur J Endocrinol. 2008. PMID: 18166818 Clinical Trial.
-
Caloric restriction and intermittent fasting alter hepatic lipid droplet proteome and diacylglycerol species and prevent diabetes in NZO mice.Biochim Biophys Acta. 2015 May;1851(5):566-76. doi: 10.1016/j.bbalip.2015.01.013. Epub 2015 Jan 31. Biochim Biophys Acta. 2015. PMID: 25645620
-
A review of the molecular pathways mediating the improvement in diabetes mellitus following caloric restriction.J Cell Physiol. 2019 Jun;234(6):8436-8442. doi: 10.1002/jcp.27760. Epub 2018 Nov 13. J Cell Physiol. 2019. PMID: 30426486 Review.
-
Mitochondrial Adaptation in Skeletal Muscle: Impact of Obesity, Caloric Restriction, and Dietary Compounds.Curr Nutr Rep. 2024 Sep;13(3):500-515. doi: 10.1007/s13668-024-00555-7. Epub 2024 Jul 8. Curr Nutr Rep. 2024. PMID: 38976215 Free PMC article. Review.
Cited by
-
The effects of caloric restriction on adipose tissue and metabolic health are sex- and age-dependent.Elife. 2023 Apr 25;12:e88080. doi: 10.7554/eLife.88080. Elife. 2023. PMID: 37096321 Free PMC article.
-
Short Sleep Duration Disrupts Glucose Metabolism: Can Exercise Turn Back the Clock?Exerc Sport Sci Rev. 2024 Jul 1;52(3):77-86. doi: 10.1249/JES.0000000000000339. Epub 2024 Apr 12. Exerc Sport Sci Rev. 2024. PMID: 38608214 Review.
-
Interleukin-2 improves insulin sensitivity through hypothalamic sympathetic activation in obese mice.J Neuroinflammation. 2024 Oct 4;21(1):250. doi: 10.1186/s12974-024-03244-y. J Neuroinflammation. 2024. PMID: 39367382 Free PMC article.
-
Polyphenol-Rich Leaf of Annona squamosa Stimulates Insulin Release from BRIN-BD11 Cells and Isolated Mouse Islets, Reduces (CH2O)n Digestion and Absorption, and Improves Glucose Tolerance and GLP-1 (7-36) Levels in High-Fat-Fed Rats.Metabolites. 2022 Oct 20;12(10):995. doi: 10.3390/metabo12100995. Metabolites. 2022. PMID: 36295897 Free PMC article.
-
Diet induced insulin resistance is due to induction of PTEN expression.Res Sq [Preprint]. 2024 Jun 27:rs.3.rs-4021885. doi: 10.21203/rs.3.rs-4021885/v1. Res Sq. 2024. PMID: 38978604 Free PMC article. Preprint.
References
-
- Kelley DE, He J, Menshikova EV, Ritov VB. Dysfunction of mitochondria in human skeletal muscle in type 2 diabetes. Diabetes 2002;51:2944–2950 - PubMed
-
- Goodpaster BH, Thaete FL, Simoneau JA, Kelley DE. Subcutaneous abdominal fat and thigh muscle composition predict insulin sensitivity independently of visceral fat. Diabetes 1997;46:1579–1585 - PubMed
Publication types
MeSH terms
Substances
Grants and funding
- R01 DK049230/DK/NIDDK NIH HHS/United States
- R01 DK041973/DK/NIDDK NIH HHS/United States
- R01 DK059615/DK/NIDDK NIH HHS/United States
- UL1-TR-000135/TR/NCATS NIH HHS/United States
- T32-DK-007352/DK/NIDDK NIH HHS/United States
- R24-DK-090963/DK/NIDDK NIH HHS/United States
- T32 DK007198/DK/NIDDK NIH HHS/United States
- R24 DK090963/DK/NIDDK NIH HHS/United States
- P30 DK050456/DK/NIDDK NIH HHS/United States
- DK-50456/DK/NIDDK NIH HHS/United States
- KL2 TR000136/TR/NCATS NIH HHS/United States
- KL2 RR024151/RR/NCRR NIH HHS/United States
- U24 DK100469/DK/NIDDK NIH HHS/United States
- R01-DK-41973/DK/NIDDK NIH HHS/United States
- T32-DK-007198/DK/NIDDK NIH HHS/United States
- UL1 TR000135/TR/NCATS NIH HHS/United States
- Howard Hughes Medical Institute/United States
- R01-DK-49230/DK/NIDDK NIH HHS/United States
- T32 DK007352/DK/NIDDK NIH HHS/United States
- KL2-RR-024151/RR/NCRR NIH HHS/United States
- U24-DK-100469/DK/NIDDK NIH HHS/United States
- KL2-TR-000136-07/TR/NCATS NIH HHS/United States
- R56 DK041973/DK/NIDDK NIH HHS/United States
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
