

Factors associated with CD8+ T-cell activation in HIV-1-infected patients on long-term antiretroviral therapy
- PMID: 25072610
- PMCID: PMC4167746
- DOI: 10.1097/QAI.0000000000000286
Factors associated with CD8+ T-cell activation in HIV-1-infected patients on long-term antiretroviral therapy
Abstract
Background: Abnormal levels of CD8 T-cell activation persist in HIV-1-infected patients on suppressive antiretroviral therapy (ART) and may be deleterious.
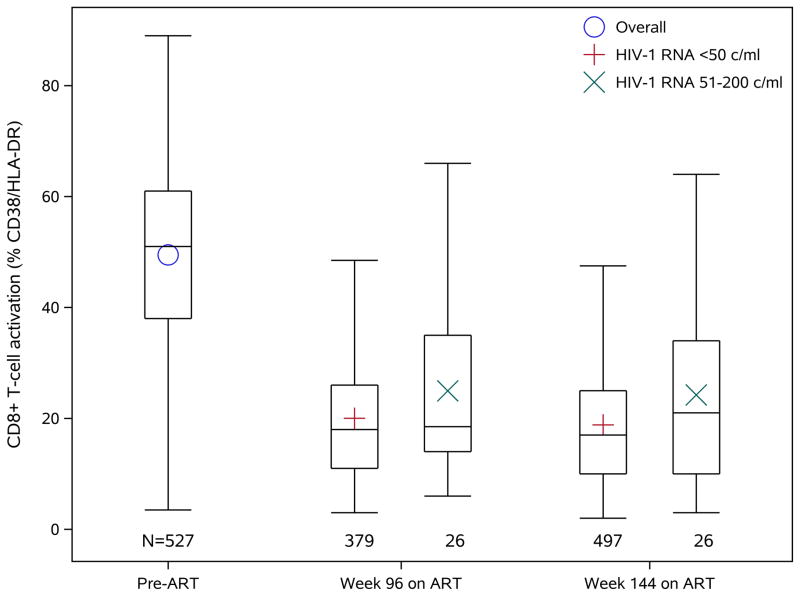
Methods: CD8 T-cell activation (% coexpressing CD38/HLA-DR) was analyzed on blood specimens from 833 HIV-1-infected patients on ART for ≥96 weeks with concurrent plasma HIV RNA (vRNA) ≤200 copies per milliliter. Factors associated with CD8 T-cell activation were assessed using generalized estimating equations to incorporate longitudinal measurements (median 4/participant).
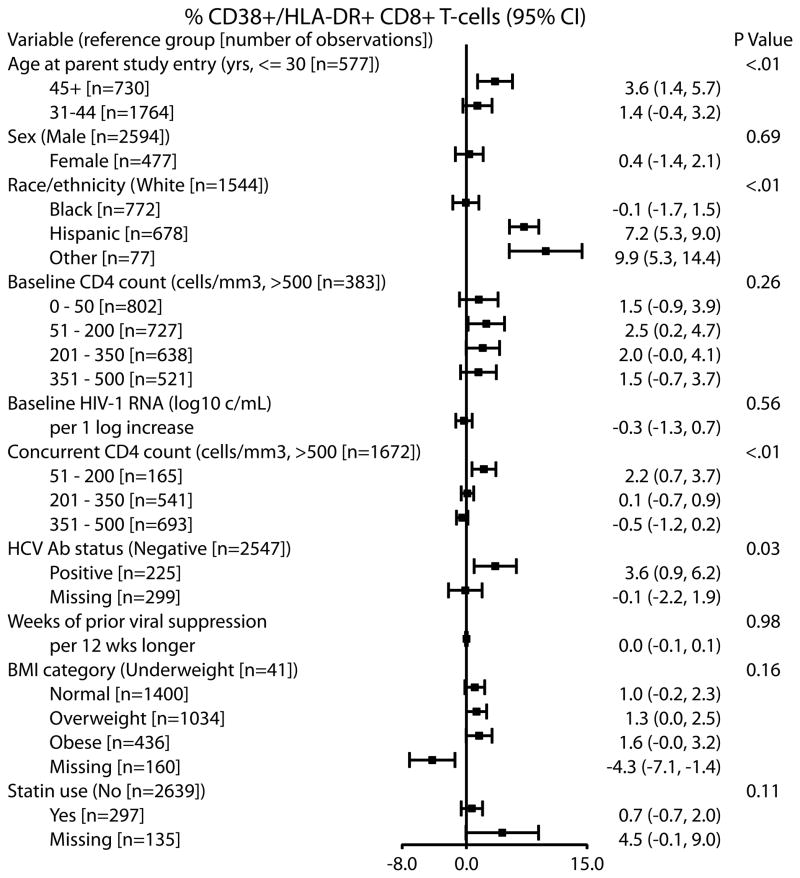
Results: Participants were 84% men, 47% white, 28% black, and 22% Hispanic, with median pre-ART age 38 years and median ART exposure 144 weeks. CD8 T-cell activation was higher at timepoints when vRNA was 51-200 versus ≤50 copies per milliliter [mean CD8 T-cell activation 23.4% vs. 19.7%; adjusted difference: 1.7% (95% confidence interval: 0.1 to 3.4), P = 0.042]. Restricting to vRNA ≤50 copies per milliliter, multivariable models showed the following factors associated with higher CD8 T-cell activation: older age [≥45 vs. ≤30 years: 3.6% (1.4 to 5.7), P = 0.004], hepatitis C virus antibody positivity [3.6% (0.9 to 6.2), P = 0.032], Hispanic vs. white [7.2% (5.3 to 9.0), P < 0.001], lower concurrent CD4 count [≤200 vs. >500 cells/mm: 2.2% (0.7 to 3.7), P < 0.001], lower concurrent CD4/CD8 ratio [-2.6% (-3.7 to -1.5) per 0.5 unit increase, P < 0.001], and higher pre-ART CD8 T-cell activation [2.0% (1.6 to 2.5) per 10% higher, P < 0.001].
Conclusions: In participants included in our analysis, residual low-level viremia between 51 and 200 copies per milliliter during ART was shown to be associated with greater CD8 T-cell activation than full suppression to <50 copies per milliliter. Older age, hepatitis C virus antibody positivity, race/ethnicity, higher pre-ART CD8 T-cell activation, and lower concurrent CD4/CD8 ratio and CD4 T-cell count also contribute to greater CD8 T-cell activation during suppressive ART.
Conflict of interest statement
B.T. has served as an advisor and/or received research support (to Northwestern University) from Janssen, Pfizer, GlaxoSmithKline and ViiV. R.T.G. has received institutional research grant support from Abbott, Viiv and Janssen. A.C.C. receives research support from Merck and past research support from Schering-Plough; previously owned stock in Abbott, Bristol-Myers-Squibb, Johnson and Johnson, and Pfizer; and was a DSMB member for a Merck-sponsored study. C.F. reports receiving research grant support from Boehringer-Ingelheim and GlaxoSmithKline for research unrelated to this study; and serving as a consultant to Bristol-Myers Squibb, Boehringer-Ingelheim, GlaxoSmithKline, Merck, Roche, Schering-Plough, Tobira Therapeutics, Tibotec, Vertex, Virostatics, and ViiV Healthcare. All other authors report no potential conflict.
Figures
Similar articles
-
Impact of CD8+ T-cell activation on CD4+ T-cell recovery and mortality in HIV-infected Ugandans initiating antiretroviral therapy.AIDS. 2011 Nov 13;25(17):2123-31. doi: 10.1097/QAD.0b013e32834c4ac1. AIDS. 2011. PMID: 21881481 Free PMC article.
-
CD8+ T-cell activation in HIV-1-infected patients experiencing transient low-level viremia during antiretroviral therapy.J Acquir Immune Defic Syndr. 2013 May 1;63(1):101-4. doi: 10.1097/QAI.0b013e3182895af4. J Acquir Immune Defic Syndr. 2013. PMID: 23392463 Free PMC article. Clinical Trial.
-
Dominant enrichment of phenotypically activated CD38(+) HLA-DR(+) CD8(+) T cells, rather than CD38(+) HLA-DR(+) CD4(+) T cells, in HIV/HCV coinfected patients on antiretroviral therapy.J Med Virol. 2016 Aug;88(8):1347-56. doi: 10.1002/jmv.24475. Epub 2016 Jan 20. J Med Virol. 2016. PMID: 26765625
-
Activation of CD8 T cells normalizes and correlates with the level of infectious provirus in tonsils during highly active antiretroviral therapy in early HIV-1 infection.AIDS. 1999 Dec 3;13(17):2365-76. doi: 10.1097/00002030-199912030-00008. AIDS. 1999. PMID: 10597778
-
A Systematic Review and Meta-Analysis on the Impact of Statin Treatment in HIV Patients on Antiretroviral Therapy.Int J Environ Res Public Health. 2023 Apr 27;20(9):5668. doi: 10.3390/ijerph20095668. Int J Environ Res Public Health. 2023. PMID: 37174188 Free PMC article. Review.
Cited by
-
Serious Non-AIDS Events: Therapeutic Targets of Immune Activation and Chronic Inflammation in HIV Infection.Drugs. 2016 Apr;76(5):533-49. doi: 10.1007/s40265-016-0546-7. Drugs. 2016. PMID: 26915027 Free PMC article. Review.
-
Host and Viral Factors in HIV-Mediated Bystander Apoptosis.Viruses. 2017 Aug 22;9(8):237. doi: 10.3390/v9080237. Viruses. 2017. PMID: 28829402 Free PMC article. Review.
-
Impact of HIV-ART on the restoration of Th17 and Treg cells in blood and female genital mucosa.Sci Rep. 2019 Feb 13;9(1):1978. doi: 10.1038/s41598-019-38547-1. Sci Rep. 2019. PMID: 30760809 Free PMC article.
-
Treatment intensification with maraviroc (CCR5 antagonist) leads to declines in CD16-expressing monocytes in cART-suppressed chronic HIV-infected subjects and is associated with improvements in neurocognitive test performance: implications for HIV-associated neurocognitive disease (HAND).J Neurovirol. 2014 Dec;20(6):571-82. doi: 10.1007/s13365-014-0279-x. Epub 2014 Sep 17. J Neurovirol. 2014. PMID: 25227930 Free PMC article.
-
HIV post-treatment controllers have distinct immunological and virological features.Proc Natl Acad Sci U S A. 2023 Mar 14;120(11):e2218960120. doi: 10.1073/pnas.2218960120. Epub 2023 Mar 6. Proc Natl Acad Sci U S A. 2023. PMID: 36877848 Free PMC article.
References
-
- Valdez H, Connick E, Smith KY, et al. Limited immune restoration after 3 years’ suppression of HIV-1 replication in patients with moderately advanced disease. AIDS. 2002;16:1859–1866. - PubMed
-
- Gandhi RT, Spritzler J, Chan E, et al. Effect of baseline- and treatment-related factors on immunologic recovery after initiation of antiretroviral therapy in HIV-1-positive subjects: results from ACTG 384. J Acquir Immune Defic Syndr. 2006;42(4):426–434. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
- AI-68634/AI/NIAID NIH HHS/United States
- UM1 AI069434/AI/NIAID NIH HHS/United States
- U01 AI038855/AI/NIAID NIH HHS/United States
- AI-69434/AI/NIAID NIH HHS/United States
- AI-68636/AI/NIAID NIH HHS/United States
- UM1 AI069496/AI/NIAID NIH HHS/United States
- UM1 AI106701/AI/NIAID NIH HHS/United States
- UM1 AI069465/AI/NIAID NIH HHS/United States
- AI-38858/AI/NIAID NIH HHS/United States
- P30 MH062246/MH/NIMH NIH HHS/United States
- U01 AI069434/AI/NIAID NIH HHS/United States
- UM1 AI069412/AI/NIAID NIH HHS/United States
- UM1 AI068634/AI/NIAID NIH HHS/United States
- AI-38855/AI/NIAID NIH HHS/United States
- U01 AI038858/AI/NIAID NIH HHS/United States
- U01 AI068636/AI/NIAID NIH HHS/United States
- U01 AI068634/AI/NIAID NIH HHS/United States
- UM1 AI068636/AI/NIAID NIH HHS/United States
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
