

Whole-exome sequencing-based discovery of STIM1 deficiency in a child with fatal classic Kaposi sarcoma
- PMID: 20876309
- PMCID: PMC2964585
- DOI: 10.1084/jem.20101597
Whole-exome sequencing-based discovery of STIM1 deficiency in a child with fatal classic Kaposi sarcoma
Abstract
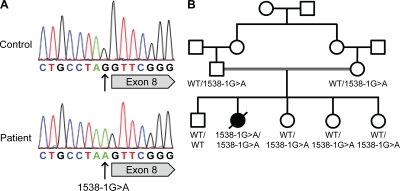
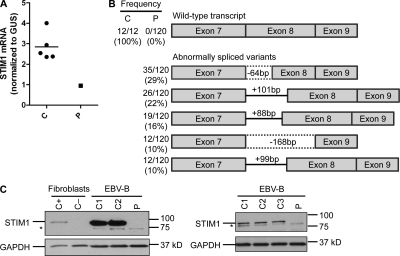
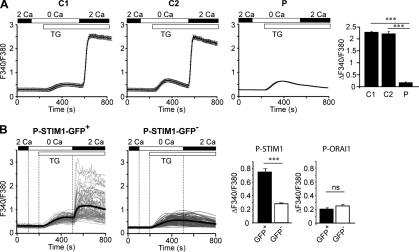
Classic Kaposi sarcoma (KS) is exceedingly rare in children from the Mediterranean Basin, despite the high prevalence of human herpesvirus-8 (HHV-8) infection in this region. We hypothesized that rare single-gene inborn errors of immunity to HHV-8 may underlie classic KS in childhood. We investigated a child with no other unusually severe infectious or tumoral phenotype who died from disseminated KS at two years of age. Whole-exome sequencing in the patient revealed a homozygous splice-site mutation in STIM1, the gene encoding stromal interaction molecule 1, which regulates store-operated Ca(2+) entry. STIM1 mRNA splicing, protein production, and Ca(2+) influx were completely abolished in EBV-transformed B cell lines from the patient, but were rescued by the expression of wild-type STIM1. Based on the previous discovery of STIM1 deficiency in a single family with a severe T cell immunodeficiency and the much higher risk of KS in individuals with acquired T cell deficiencies, we conclude that STIM1 T cell deficiency precipitated the development of lethal KS in this child upon infection with HHV-8. Our report provides the first evidence that isolated classic KS in childhood may result from single-gene defects and provides proof-of-principle that whole-exome sequencing in single patients can decipher the genetic basis of rare inborn errors.
Figures
Similar articles
-
Kaposi Sarcoma of Childhood: Inborn or Acquired Immunodeficiency to Oncogenic HHV-8.Pediatr Blood Cancer. 2016 Mar;63(3):392-7. doi: 10.1002/pbc.25779. Epub 2015 Oct 15. Pediatr Blood Cancer. 2016. PMID: 26469702 Free PMC article. Review.
-
Classic Kaposi sarcoma in 3 unrelated Turkish children born to consanguineous kindreds.Pediatrics. 2010 Mar;125(3):e704-8. doi: 10.1542/peds.2009-2224. Epub 2010 Feb 15. Pediatrics. 2010. PMID: 20156905 Free PMC article.
-
Inherited human OX40 deficiency underlying classic Kaposi sarcoma of childhood.J Exp Med. 2013 Aug 26;210(9):1743-59. doi: 10.1084/jem.20130592. Epub 2013 Jul 29. J Exp Med. 2013. PMID: 23897980 Free PMC article.
-
HHV-8-associated Kaposi sarcoma in a child with IFNgammaR1 deficiency.J Pediatr. 2004 Apr;144(4):519-23. doi: 10.1016/j.jpeds.2003.11.012. J Pediatr. 2004. PMID: 15069403
-
Rapidly progressive Kaposi's Sarcoma in an Iraqi boy received Valproic acid: a case report and review of literature.BMC Pediatr. 2016 Jul 26;16:111. doi: 10.1186/s12887-016-0653-3. BMC Pediatr. 2016. PMID: 27459853 Free PMC article. Review.
Cited by
-
Mycobacterial disease and impaired IFN-γ immunity in humans with inherited ISG15 deficiency.Science. 2012 Sep 28;337(6102):1684-8. doi: 10.1126/science.1224026. Epub 2012 Aug 2. Science. 2012. PMID: 22859821 Free PMC article.
-
Immunodeficiency, autoinflammation and amylopectinosis in humans with inherited HOIL-1 and LUBAC deficiency.Nat Immunol. 2012 Dec;13(12):1178-86. doi: 10.1038/ni.2457. Epub 2012 Oct 28. Nat Immunol. 2012. PMID: 23104095 Free PMC article.
-
Nationwide registry-based analysis of cancer clustering detects strong familial occurrence of Kaposi sarcoma.PLoS One. 2013;8(1):e55209. doi: 10.1371/journal.pone.0055209. Epub 2013 Jan 24. PLoS One. 2013. PMID: 23365693 Free PMC article.
-
Statistical guidance for experimental design and data analysis of mutation detection in rare monogenic mendelian diseases by exome sequencing.PLoS One. 2012;7(2):e31358. doi: 10.1371/journal.pone.0031358. Epub 2012 Feb 10. PLoS One. 2012. PMID: 22348076 Free PMC article.
-
A Report of Novel STIM1 Deficiency and 6-Year Follow-Up of Two Previous Cases Associated with Mild Immunological Phenotype.J Clin Immunol. 2019 Apr;39(3):249-256. doi: 10.1007/s10875-019-00618-3. Epub 2019 Apr 4. J Clin Immunol. 2019. PMID: 30949876 No abstract available.
References
-
- Akman E.S., Ertem U., Tankal V., Pamir A., Tuncer A.M., Uluogu O. 1989. Aggressive Kaposi’s sarcoma in children: a case report. Turk. J. Pediatr. 31:297–303 - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Molecular Biology Databases
Miscellaneous
