

Muscarinic receptors in the bladder: from basic research to therapeutics
- PMID: 16465186
- PMCID: PMC1751492
- DOI: 10.1038/sj.bjp.0706560
Muscarinic receptors in the bladder: from basic research to therapeutics
Abstract
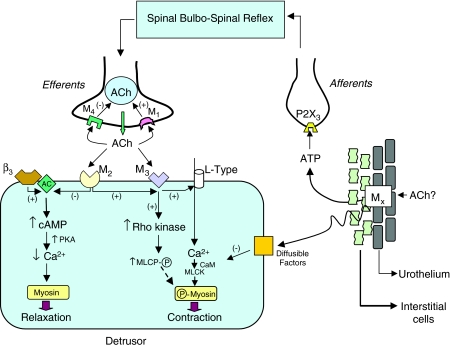
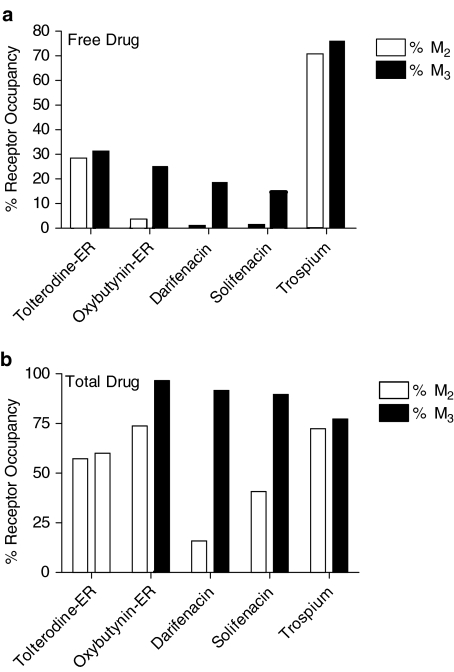
Muscarinic receptor antagonists (antimuscarinics) serve as the cornerstone in the pharmacological management of overactive bladder (OAB) by relieving the symptoms of urgency, frequency and incontinence. These drugs operate primarily by antagonizing post-junctional excitatory muscarinic receptors (M(2)/M(3)) in the detrusor. The combination of pharmacological and gene knockout studies has greatly advanced our understanding of the functional role of muscarinic receptors in the bladder. M(3) receptors produce direct smooth muscle contraction by a mechanism that relies on entry of extracellular calcium through L-type channels and activation of a rho kinase. M(2) receptors, which predominate in number, appear to facilitate M(3)-mediated contractions. M(2) receptors can also produce bladder contractions indirectly by reversing cAMP-dependent beta-adrenoceptor-mediated relaxation, although the physiological role of beta-adrenoceptors in detrusor relaxation is controversial. Emerging evidence suggests that muscarinic receptors in the urothelium/suburothelium can modulate the release of certain factors, which in turn may affect bladder function at the efferent or afferent axis. Currently, oxybutynin, tolterodine, darifenacin, solifenacin and trospium are the five major antimuscarinics approved for the treatment of OAB. Comparative clinical studies have shown that oxybutynin and solifenacin may be marginally more effective than tolterodine, although the latter seems to be better tolerated. Pharmacokinetic-pharmacodynamic analyses using plasma concentrations of 'total drug' indicate that, at therapeutic doses, the clinical efficacy of darifenacin and solifenacin may be driven primarily by selective M(3) receptor occupation, whereas the pharmacodynamic effects of pan-selective molecules (such as tolterodine, trospium) may potentially involve multiple receptors, including M(2) and M(3). Furthermore, high M(3) receptor occupation is the likely explanation for the greater propensity of darifenacin and oxybutynin to cause dry mouth and/or constipation. Although the recently introduced drugs represent a significant improvement over older drugs, especially with respect to the convenience of dosing schedule, their overall efficacy and tolerability profile is still less than optimal and patient persistence with therapy is low. Recent advances in basic research have not yet offered a clear discovery path for improving the therapeutic index of antimuscarinic molecules. There is still an unmet need for an antimuscarinic medicine with superior clinical effectiveness that can translate into better persistence on therapy.
Figures
Similar articles
-
Muscarinic receptor antagonists for overactive bladder.BJU Int. 2007 Nov;100(5):987-1006. doi: 10.1111/j.1464-410X.2007.07205.x. BJU Int. 2007. PMID: 17922784 Review.
-
Pharmacological properties of TD-6301, a novel bladder selective muscarinic receptor antagonist.Eur J Pharmacol. 2009 Mar 1;605(1-3):145-52. doi: 10.1016/j.ejphar.2008.12.043. Epub 2009 Jan 10. Eur J Pharmacol. 2009. PMID: 19168050
-
Antimuscarinics for the treatment of overactive bladder: current options and emerging therapies.Curr Opin Investig Drugs. 2004 Jan;5(1):40-9. Curr Opin Investig Drugs. 2004. PMID: 14983972 Review.
-
The cost-effectiveness of solifenacin vs fesoterodine, oxybutynin immediate-release, propiverine, tolterodine extended-release and tolterodine immediate-release in the treatment of patients with overactive bladder in the UK National Health Service.BJU Int. 2010 Aug;106(4):506-14. doi: 10.1111/j.1464-410X.2009.09160.x. Epub 2010 Feb 3. BJU Int. 2010. PMID: 20132203
-
Effects of imidafenacin (KRP-197/ONO-8025), a new anti-cholinergic agent, on muscarinic acetylcholine receptors. High affinities for M3 and M1 receptor subtypes and selectivity for urinary bladder over salivary gland.Arzneimittelforschung. 2007;57(2):92-100. doi: 10.1055/s-0031-1296589. Arzneimittelforschung. 2007. PMID: 17396619
Cited by
-
Comparative functional selectivity of imidafenacin and propiverine, antimuscarinic agents, for the urinary bladder over colon in conscious rats.Naunyn Schmiedebergs Arch Pharmacol. 2015 Nov;388(11):1171-8. doi: 10.1007/s00210-015-1155-9. Epub 2015 Jul 28. Naunyn Schmiedebergs Arch Pharmacol. 2015. PMID: 26216447
-
Blood-brain barrier permeation and efflux exclusion of anticholinergics used in the treatment of overactive bladder.Drugs Aging. 2012 Apr 1;29(4):259-73. doi: 10.2165/11597530-000000000-00000. Drugs Aging. 2012. PMID: 22390261 Review.
-
In vivo characterization of muscarinic receptors in peripheral tissues: evaluation of bladder selectivity of anticholinergic agents to treat overactive bladder.Naunyn Schmiedebergs Arch Pharmacol. 2008 Jun;377(4-6):463-71. doi: 10.1007/s00210-007-0207-1. Epub 2007 Dec 12. Naunyn Schmiedebergs Arch Pharmacol. 2008. PMID: 18074121
-
Safety and tolerability profiles of anticholinergic agents used for the treatment of overactive bladder.Drug Saf. 2011 Sep 1;34(9):733-54. doi: 10.2165/11592790-000000000-00000. Drug Saf. 2011. PMID: 21830836 Review.
-
Overactive bladder - 18 years - Part II.Int Braz J Urol. 2016 Mar-Apr;42(2):199-214. doi: 10.1590/S1677-5538.IBJU.2015.0367. Int Braz J Urol. 2016. PMID: 27176185 Free PMC article. Review.
References
-
- ABRAMS P., CARDOZO L., FALL M., GRIFFITHS D., ROSIER P., ULMSTEN U., VAN KERREBROECK P., VICTOR A., WEIN A. Standardisation Sub-Committee of the International Continence Society. Related Articles. The standardisation of terminology in lower urinary tract function: report from the standardisation sub-committee of the International Continence Society. Urology. 2003;61:37–49. - PubMed
-
- ANDERSSON K.E. Changes in bladder tone during filling: pharmacological aspects. Scand. J. Urol. Nephrol. Suppl. 1999;201:67–72. - PubMed
-
- ANDERSSON K.E., YOSHAIDA M. Antimuscarinics and the overactive detrusor – which is the main mechanism of action. Eur. Urol. 2003;43:1–5. - PubMed
-
- ANDRADE S.E., WALKER A.M., GOTTLIEB L.K., HOLLENBERG N.K., TESTA M.A., SAPERIA G.M., PLATT R. Discontinuation of antihyperlipidemic drugs: Do rates reported in clinical trials reflect rates in primary care settings. New Engl. J. Med. 1995;332:1125–1131. - PubMed
-
- CARDOZO L., LISEC M., MILLARD R., VAN VIERSSEN TRIP O., KUZMIN I., DROGENDIJK T.E., HUANG M., RIDDER A.M.2004Randomized, double-blind placebo controlled trial of the once daily antimuscarinic agent solifenacin succinate in patients with overactive bladder J. Urol. 172Part 1), 1919–1924. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Molecular Biology Databases
