

Different microcirculatory and interstitial matrix patterns in idiopathic dilated cardiomyopathy and Chagas' disease: a three dimensional confocal microscopy study
- PMID: 10455076
- PMCID: PMC1729160
- DOI: 10.1136/hrt.82.3.279
Different microcirculatory and interstitial matrix patterns in idiopathic dilated cardiomyopathy and Chagas' disease: a three dimensional confocal microscopy study
Abstract
Objective: To analyse the morphological aspects of the extracellular matrix and microcirculation to clarify whether chronic Chagas' cardiopathy (CCC) is an accurate model to study the pathogenesis of idiopathic dilated cardiomyopathy (IDCM).
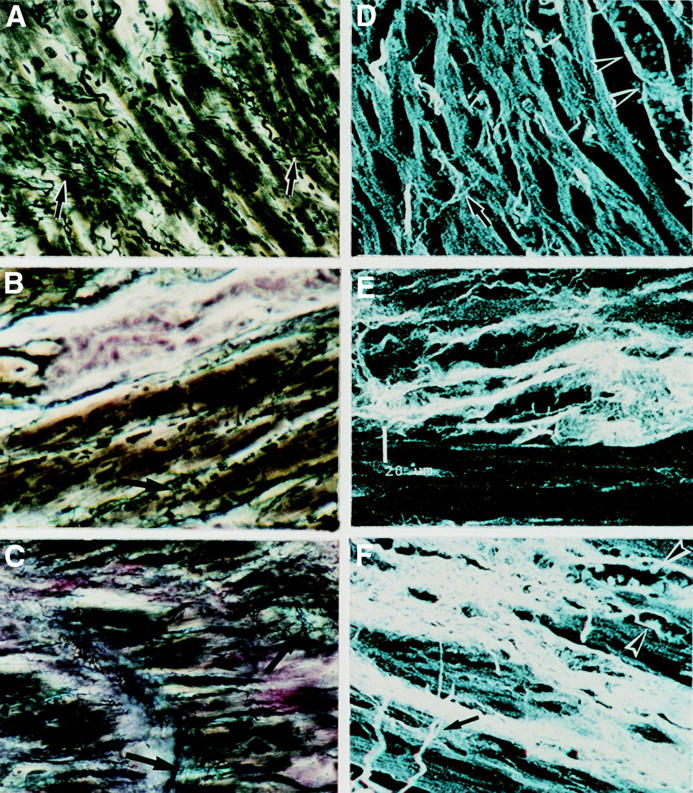
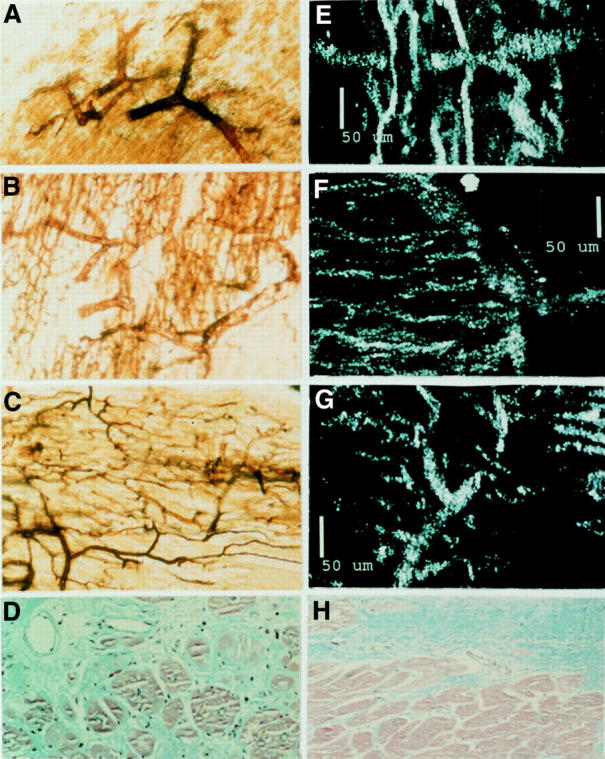
Design: Thick histological myocardial sections were prepared to analyse collagen, and microcirculation was examined during confocal laser and light microscopy.
Setting: The specimens were prepared at the pathology service of the Heart Institute of São Paulo, Brazil.
Patients: Nine control hearts, eight IDCM hearts, and 10 CCC hearts were studied after necropsy.
Main outcome measures: The number of collagen struts per 100x field, the area of fibrosis (%), and the diameters of arterioles and capillaries were measured in each heart to establish outcome.
Results: A smaller number (mean (SD)) of collagen struts was seen in the hearts in the IDCM group (9.1 (4.1)) than in the control (22.4 (3.2)) (p < 0.05) or CCC (15.7 (7.4)) (p > 0.05) groups. Fibrosis was greater in the CCC hearts (13.8 (10.5)%) than in the IDCM hearts (5.9 (6.6)%) (p > 0.05). Major increases in arteriole (65.4 (9.9) microm) and capillary (9.9 (1.7) microm) diameters were seen in the CCC hearts but not in the IDCM hearts (arteriole diameter 40.3 (7.9) microm; capillary diameter 7.9 (1.3) microm).
Conclusions: Hearts demonstrating CCC and IDCM present different extracellular and microvessel alterations. This suggests that distinct pathogenic mechanisms are responsible for each condition and that CCC is not an effective model to study IDCM.
Figures
Similar articles
-
Coronary microcirculation remodeling in patients with idiopathic dilated cardiomyopathy.Cardiology. 2011;119(4):191-6. doi: 10.1159/000331440. Epub 2011 Oct 4. Cardiology. 2011. PMID: 21986631
-
The role of storage of interstitial myocardial collagen on the overlife rate of patients with idiopathic and Chagasic dilated cardiomyopathy.Arq Bras Cardiol. 2006 Dec;87(6):757-62. doi: 10.1590/s0066-782x2006001900012. Arq Bras Cardiol. 2006. PMID: 17262114 English, Portuguese.
-
Patterns of myocardial fibrosis in idiopathic cardiomyopathies and chronic Chagasic cardiopathy.Can J Cardiol. 1991 Sep;7(7):287-94. Can J Cardiol. 1991. PMID: 1933634
-
Coronary microvascular abnormalities in Chagas' disease.Am Heart J. 1996 Jul;132(1 Pt 1):207-10. doi: 10.1016/s0002-8703(96)90417-2. Am Heart J. 1996. PMID: 8701871 Review. No abstract available.
-
[Specific dilated myocardiopathy. Chronic chagasic cardiopathy at the National Institute of Cardiology Ignacio Chávez].Arch Cardiol Mex. 2002 Jan-Mar;72 Suppl 1:S148-52. Arch Cardiol Mex. 2002. PMID: 12001835 Review. Spanish.
Cited by
-
T-Cell Subpopulations Exhibit Distinct Recruitment Potential, Immunoregulatory Profile and Functional Characteristics in Chagas versus Idiopathic Dilated Cardiomyopathies.Front Cardiovasc Med. 2022 Feb 2;9:787423. doi: 10.3389/fcvm.2022.787423. eCollection 2022. Front Cardiovasc Med. 2022. PMID: 35187122 Free PMC article.
-
Absence of Atherosclerosis in Chagas' Disease: The Role of Trypanosoma Cruzi Transialidase.Arq Bras Cardiol. 2020 Dec;115(6):1061-1062. doi: 10.36660/abc.20201229. Arq Bras Cardiol. 2020. PMID: 33470301 Free PMC article. English, Portuguese. No abstract available.
-
Epicardial and Endocardial Ablation Based on Channel Mapping in Patients With Ventricular Tachycardia and Chronic Chagasic Cardiomyopathy: Importance of Late Potential Mapping During Sinus Rhythm to Recognize the Critical Substrate.J Am Heart Assoc. 2022 Jan 4;11(1):e021889. doi: 10.1161/JAHA.121.021889. Epub 2021 Dec 20. J Am Heart Assoc. 2022. PMID: 34927451 Free PMC article.
-
Advanced management of ventricular arrhythmias in chronic Chagas cardiomyopathy.Heart Rhythm O2. 2021 Dec 17;2(6Part B):807-818. doi: 10.1016/j.hroo.2021.10.010. eCollection 2021 Dec. Heart Rhythm O2. 2021. PMID: 34988532 Free PMC article.
-
Infectious myocarditis: the role of the cardiac vasculature.Heart Fail Rev. 2018 Jul;23(4):583-595. doi: 10.1007/s10741-018-9688-x. Heart Fail Rev. 2018. PMID: 29536322 Free PMC article. Review.
References
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources