
Key Points
-
In the past three decades, the approach to cancer prevention has moved from population and epidemiological studies to molecular targeting and immunological approaches and to identifying high-risk pre-cancerous lesions in individuals using emerging early detection technologies.
-
Global implementation of these scientifically-sound lifestyle- and medical-based cancer prevention strategies has the potential to reduce worldwide cancer incidence, prevalence and mortality rates in the decades ahead.
-
As more is learned about the mechanisms and pathways that are influenced by genetic and molecular changes that initiate cancer or encourage its progression, targeted therapies are being developed to interrupt these processes. Additional strategies are specifically focused on interrupting the late-stage, but still pre-malignant, processes that lead to in situ cancers, with the goal of averting progression to actual invasive cancer.
-
The success of vaccines for human papilloma virus (HPV)- and hepatitis B virus (HBV)-related cancers has led to an increased focus on immunologically based research for many other cancers. Efforts are ongoing to develop immune response modulation strategies to augment the innate immunity and to develop vaccines against oncogenic infectious agents, as well as tumour-associated and tumour-specific antigens.
-
The groundwork for the future of cancer prevention is currently being developed through multidisciplinary initiatives that involve researchers from tradition biology-based laboratories, as well as collaborators from the fields of information technology, imaging technologies, '-omics' (such as genomics, proteomics and metabolomics) and communication. Expertise in communication is essential to disseminate research findings to the communities that are likely to benefit from these findings. Inherent to this future progress is a focus on precision (individualized) medicine that will include identifying those who are at a high risk of developing cancer.
Abstract
Prevention of cancer remains the most promising strategy for reducing both its incidence and the mortality due to this disease. For more than four decades, findings from epidemiology, basic research and clinical trials have informed the development of lifestyle and medical approaches to cancer prevention. These include selective oestrogen receptor modulators and aromatase inhibitors for breast cancer, the 5-α-reductase inhibitors finasteride and dutasteride for prostate cancer, and the development of vaccines for viruses that are associated with specific cancers. Future directions include genetic, proteomic and other molecular approaches for identifying pathways that are associated with cancer initiation and development, as well as refining the search for immunologically modifiable causes of cancer.
Similar content being viewed by others

Main
Globally, cancer is the leading cause of death in developed countries and the second leading cause of death in developing countries, where the cancer burden is rising. Estimates for 2008 pointed to 12.7 million cancer cases and 7.6 million cancer deaths worldwide1,2. Despite improvements in the treatment of various common cancers, a large cancer burden remains, providing a growing incentive to address this problem by a preventive approach. Although eliminating exposure to carcinogens, such as tobacco, is a well-established approach to prevention, active intervention with agents that are expected to reduce the risk of cancer is becoming increasingly accepted3,4.
Carcinogenesis: opportunities for prevention
Common, adult, epithelial cancers represent the final step in a multi-year progression from normal tissue, through increasingly abnormal-looking stages of pre-malignancy to invasion of the basement membrane, which constitutes overt cancer. Once a histological boundary has been penetrated, invasive cancer has the potential to metastasize, and metastases generally lead to cancer-related mortality.
The evolution of these adult malignancies involves the gradual accumulation of genetic and epigenetic cancer-promoting changes (Fig. 1). The affected genes, oncogenes, as well as tumour suppressor genes, are mutated in a manner that subverts their normal function, thereby contributing to the multiple processes that are considered to be the hallmarks of cancer5,6. Additional modifications, such as epigenetic silencing of tumour suppressor genes also contribute to the relentless progression to invasive cancer, as can aspects of the immune response, such as immunoediting7.

The progression from normal tissue to invasive cancer is characterized by genetic and epigenetic changes that occur at different points along the carcinogenic continuum. This continuum is organ- and tissue-specific, with the time between initiation and invasive cancer dependent on the accumulation of these changes. Because of the lengthy time between initiation and overt (that is, invasive) cancer in most cancer types, early intervention and prevention strategies can potentially interrupt the cancer progression process. Crucial gene mutations that contribute to this progression from normal tissue to invasive cancer vary between cancer types. These genes, their mutations and their epigenetic modifications are the subject of intensive research in the hope that they will serve as targets of anticancer or prevention agents (drugs and nutrients). Appropriately targeted interventions should interrupt the cancer-promoting consequences of genetic mutations and/or epigenetic modifications, thereby halting progression through the cancer continuum. Orange cells represent changes to the tumour microenvironment, including the recruitment of immune cells, the induction of angiogenesis and the alterations in the surrounding cells such as fibroblasts. CIN, adenocarcinoma in situ; CIS, carcinoma in situ; DCIS, ductal carcinoma in situ; TIS, transitional cell carcinoma in situ.
The physiological goal of cancer prevention is to intercept these processes in order to inhibit progression to the invasive stage (Fig. 2). An understanding of the accumulating genetic and other molecular alterations that characterize progressively advanced, pre-malignant lesions will offer targets for putative, preventive interventions. Protracted carcinogenic progression also lends itself to the screening of high-risk individuals without clinically evident cancer (Box 1). Screening identifies not only early stage invasive cancers that are expected to be more amenable to cure, but also pre-malignancies that can be removed and thus prevented from progressing to invasive lesions. Finally, precancerous lesions often spontaneously regress, presumably in response to innate immune mechanisms. This endogenous behaviour suggests that exogenously administered immunological interventions should be effective in eliminating pre-cancers. In fact, prophylactic vaccines against cancer-causing infectious agents are highly effective in eliminating the causative agent for cancer initiation. Other immune response modulators might also have a role in cancer prevention.

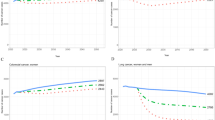
There are crucial benchmarks in the progression of cancer that afford the maximum opportunity to interrupt the cancer process. The 'gold standard' for cancer prevention is to interrupt the cancer-initiating process before pre-cancers form. However, genetic and epigenetic changes accumulate throughout the lifespan, with some changes routinely eliminated by normal innate or adaptive immune responses. The changes that do escape the immune system then provide a second opportunity for prevention efforts. Because of the number of years it may take to produce carcinoma in situ from early pre-cancers, many opportunities exist for interrupting this progression, often through aggressive screening programmes in people at a high risk for specific cancers. Another opportunity for preventing overt cancer is late in the progression, after the formation of carcinoma in situ, but still before invasion. This phase of prevention may include interventions (drugs, nutrients and surgery or radiation) for prevention and/or treatment. The presumption is that the earlier that prevention is initiated during carcinogenesis, the greater the degree to which the progression to cancer is impaired (indicated by a less steep slope in the figure). Cancer treatment slows carcinogenesis and delays death due to cancer but it is cancer prevention at earlier time points that has the biggest effect on cancer-free survival. The challenge is to detect pre-cancer early in its development for intervention. In the ultimate form of slowing of carcinogenesis, the stage of invasive cancer is never reached during the individual's lifetime; hence, cancer has truly been prevented.
The precancerous lesion itself is not the only manifestation of the process of carcinogenesis. The microenvironment encasing and interspersed with a lesion often undergoes changes that actively contribute to carcinogenesis. Precancerous changes in the microenvironment can be included in the larger category of field effects8,9: those generalized tissue changes that provide a crucial backdrop against which a given lesion will develop. Therefore, relevant changes in the microenvironment can be used as biomarkers for early detection and treatment, as well as serving as targets for chemopreventive and immunopreventive interventions8,10. Examples of microenvironment modifications that contribute to carcinogenesis include increased angiogenesis10, as well as inflammatory and immunological changes. Notably, increased mammographic density, a frequently cited risk factor for breast cancer, is actually an imaging manifestation of microenvironment changes in stromal and epithelial tissue11.
Lifestyle modifications in cancer prevention
Lifestyle modifications offer an important strategy for cancer prevention. Evidence that has accumulated since the 1980s strongly suggests that better dietary choices, increasing physical activity, maintaining a healthy weight, stopping (or not starting) the use of tobacco, moderating alcohol intake and other lifestyle factors can reduce cancer risk12,13. However, a change in only one lifestyle factor is unlikely to reduce the risk of cancer or other diseases. The exception is stopping tobacco use, which decreases the risk of several diseases, including cardiovascular, lung and kidney diseases, as well as cancer.
Tobacco. Taking into account all smoking-related diseases, tobacco use is responsible for more than 400,000 deaths in the United States each year. Although tobacco use has decreased in the United States, use is increasing in many countries in the developing world, and the focus of tobacco control measures needs to be concentrated in those countries. Tobacco control programmes in such countries have been successful in raising awareness of the dangers of tobacco use; however, initiatives will need to be adapted for implementation in developing countries owing to differences in cultural and societal norms between different countries14.
Nutrition and diet. Considerable progress has been made in the past four decades regarding our understanding of the association between diet and cancer13,15,16. The study of diet and cancer has been separated into studies investigating dietary patterns, specific foods and biologically active food components (BFCs). Large population studies have revealed associations between certain dietary patterns and cancer risk, thus setting the stage for nutritional intervention programmes that encourage healthier diets and clinical trials that include cancer risk reduction as an end point17,18.
Going beyond studies of overall diets, laboratory-based investigations are progressively identifying specific cancer-preventive nutrients and the molecular mechanisms by which they exert this property19. Among the BFCs that seem to be somewhat promising for cancer prevention are soy isoflavones for breast cancer, lycopene (found in tomatoes) for prostate cancer, as well as resveratrol (from grapes and red wine), omega-3-fatty acids (found in fish oil), pomegranate, curcumin and antioxidants such as selenium and vitamin E, for other cancers20 (Table 1). Several large Phase III trials that randomize participants to specific nutrients that have been hypothesized to lower the risk of specific cancers have been carried out. One such trial, the Selenium and Vitamin E Cancer Prevention Trial (SELECT), indicated that neither selenium nor vitamin E supplementation, alone or in combination, reduced the risk of prostate cancer compared with a placebo21. Indeed, dietary supplementation with vitamin E alone increased the risk of prostate cancer22. The reasons why the outcomes of SELECT failed to confirm cancer-preventive activity for both micronutrients, the hypothesis on which this trial was based, continue to elude us. With regard to selenium, the 200 μg per day dose and, more importantly, the l-selenomethionine formulation (different from the selenized yeast used in the hypothesis-generating Nutritional Prevention of Cancer (NPC) trial23) that were used in SELECT have been cited as potential reasons for the ineffectiveness of selenium21,24,25. Furthermore, the study populations may have differed with respect to baseline selenium levels. Baseline levels were probably low in the NPC trial as the study participants primarily lived in regions of low environmental selenium, in contrast to SELECT, which had participants throughout the United States and who were therefore subject to variations in environmental selenium. These explanations are conjectures, but they point to a need for attention to the accurate measurement of baseline and treatment levels of nutrients being tested in future cancer prevention trials. One lesson from past large, nutritionally based clinical trials is that they should ideally be designed with multiple disease end points, as well as biomarker-based end points. This will provide opportunities for better understanding the role of nutrients and BFCs across a range of diseases and conditions.
Obesity and physical activity. Obesity and physical activity are independently associated with cancer risk, but they are inherently intertwined as lifestyle factors. Estimates indicate that obesity accounts for approximately 20% of all cancer cases, and obesity has been identified as a cause of cancer in about 14% of cancer deaths in men and 20% of cancer deaths in women26. Obesity is associated with an increased risk of cancers of the oesophagus, breast (in postmenopausal women), endometrium, colon and rectum, kidney, pancreas, thyroid, gallbladder and possibly others18. Inflammation has a substantial role in the association between obesity and many cancers. A parallel increase in the levels of aromatase expression or activity with obesity (in adipose and breast tissue) has suggested a possible mechanism for the increased incidence of hormone receptor-positive breast cancer in obese, postmenopausal women27. The obesity–inflammation–aromatase axis was investigated in a small trial using breast tissue samples from obese women who had undergone breast surgery28. Of these patient samples, 50% contained crown-like structures, a marker of inflammation, and the severity of breast inflammation significantly correlated with body mass index (BMI) and adipocyte size, increased nuclear factor-κB (NF-κB)-binding activity and increased aromatase expression. This suggests that the crown-like structures, with BMI and adipocyte size, may serve as a potential biomarker for increased breast cancer risk or poor prognosis, especially in obese and overweight women28.
The relationship between obesity and cancer can also be viewed through the lens of metabolism, the reprogramming of which has increasingly been addressed as a feature of carcinogenesis and as a potential target of therapeutic intervention6. Cancer cells generally use aerobic glycolysis to generate the energy needed for cell proliferation29. This phenomenon, known since its description in the 1920s as the Warburg effect30, distinguishes malignant cells from normal differentiated cells, which rely on mitochondrial oxidative phosphorylation to generate energy. Metabolic syndrome, which encompasses abdominal obesity, hypertension, dyslipidemia and hyperglycaemia31, offers another look at the connection between the deregulation of metabolism and cancer32. This syndrome is linked to insulin resistance and the development of diabetes mellitus, which are characterized by elevated circulating levels of insulin and components of the biologically active insulin-like growth factor 1 (IGF1) axis33. Epidemiological evidence supports an association between this constellation of related diseases and conditions and the development of various cancers31,33,34. In cancer treatment, efforts to target components of this insulin–IGF system, including IGF receptor-specific antibodies and small-molecule receptor kinase inhibitors, have not yet proved to be effective therapies35. However, the promise of targeting the insulin–IGF axis may well be fulfilled in cancer prevention. In a meta-analysis of eleven epidemiological studies of cancer incidence in patients with diabetes, a 31% reduction in overall relative risk of cancer (0.69; 95% confidence interval (CI) = 0.61–0.79) was observed in individuals taking metformin compared with other anti-diabetic drugs36. The risk-reducing effect of metformin suggested by these observational data is reinforced by preclinical evidence of anticancer activity by this drug in a number of different cancers, including breast, pancreas and lung cancer37,38,39. Clinical trials of metformin as a supplement to standard-of-care therapy are already underway in the cancer treatment setting (see the ClinicalTrials.gov website; see Further information). Prevention trials using metformin are now beginning. A short-term intervention with metformin in a Phase II trial assessing the prevention of second primary cancers in women with treated localized oestrogen receptor-negative breast cancer will soon be open for accrual (clinical trial number: NCT01471106 (see Further information)). In an effort to lay the groundwork for future metformin prevention trials, the US National Cancer Institute (NCI) Division of Cancer Prevention (DCP) has recently set up a collaboration with the US National Institute of Diabetes and Digestive Diseases (NIDDK) as an extension of its Diabetes Prevention Program (DPP). The DPP is a 3,234-person randomized clinical trial that reported the efficacy of metformin in reducing the incidence of diabetes in high-risk obese or overweight individuals by 31% relative to a placebo40. Of the participants, 88% (n = 2,776) enrolled in a follow-up study, the DPP Observational Study (DPPOS), which showed a 10-year risk reduction for type 2 diabetes of 18% in the patients treated with metformin41. Through its collaborative study with the DPPOS, the NCI DCP will collect well-annotated cancer data in a structured manner that should enable analyses of cancer incidence and mortality that address the underlying question of the possible role of metformin in preventing cancer in this population, which is at an increased risk of both cancer and diabetes. Attention to the chemopreventive potential of metformin has been bolstered by mechanistic studies of this drug, which modulates adenosine monophosphate-activated protein kinase (AMPK) and inhibits the mTOR pathway38, an important cell signalling pathway in many cancers. Future mechanistic and clinical studies will answer several questions, including the exact mechanism of action of metformin for cancer prevention, why it is effective in certain organs but not in others and whether it is possible to further optimize its therapeutic index for cancer prevention in a generalized population.
In a counterintuitive and somewhat ironic twist, 15 obese individuals carrying PTEN mutations have recently been shown to exhibit increased sensitivity to insulin42. Given the predisposition to breast and other cancers linked to inherited mutations in this tumour suppressor gene43, together with the increased cancer risk associated with obesity and increased circulating insulin and IGF1 levels, this demonstration of profound constitutive insulin sensitivity in the context of obesity combined with PTEN haploinsufficiency reminds us that the interaction between the genetic and metabolic signalling pathways is complex and requires further investigation.
Cancer prevention approaches that address the obesity and metabolism axis also include insights gained from studies of calorific and dietary restriction. Calorific restriction in a variety of animal models has yielded decreases in carcinogen-induced tumours in the mammary gland, brain and intestine44,45. In humans, retrospective and historic observations concur with these animal data. For example, women in Okinawa, Japan, who adhere to a traditional lower calorie diet, exhibit lower rates of breast cancer than women in other parts of Japan46. Similarly, the Netherlands Cohort Study on Diet and Cancer, involving 62,573 women and 58,279 men who experienced puberty during the economic depression, the Second World War and the hunger winter of 1944–1945, showed a weak inverse relation between energy restriction early in life and subsequent development of colon carcinoma45,47. Unfortunately, although dietary restriction offers a promising route to cancer risk reduction, prospective randomized clinical trials of extensively restricted diet regimens are unlikely to be feasible in terms of accruing interested participants willing to adhere to strict calorific guidelines45,47,48.
Physical activity, at levels recommended by relevant organizations using evidence-based results when available49,50, may reduce the risk of developing some cancers, increase survival after a cancer diagnosis and possibly reduce the risk of cancer recurrence51. Breast cancer risk, in particular, has been shown in both observational studies and clinical trials to be inversely associated with level of physical activity52. Understanding the negative impact of sedentary behaviour on obesity and the positive impact of moderate and vigorous activity on obesity has led to new perspectives on this topic based on the lifestyles pursued by most people in post-agricultural and post-industrial societies53.
Chemoprevention using pharmaceutical agents
The term chemoprevention, first coined in 1976 to describe a pharmacological approach to cancer prevention, focuses on the pre-malignant period before the transition to invasive cancer54 (Fig. 2). An important feature of chemopreventive agents is that they confer cancer-preventive effects on high-risk tissue, blocking or reversing the development of cancer in normal or pre-malignant tissue55 (Table 1). In addition to drug-based interventions, chemoprevention is used to refer to BFCs that are administered much like a drug and may share mechanistic features with synthetic chemical medicines. An active programme of drug development for the purposes of cancer prevention has been ongoing since the 1980s4,56,57. The use of drugs that are approved and in widespread use for diseases other than cancer is another tested and reliable practice (sometimes referred to as repurposing). As discussed above in the context of the obesity–insulin–IGF axis, metformin, which is widely used for first-line management of type 2 diabetes mellitus58, reduces cancer rates compared with other insulin-lowering agents. Various epidemiological studies, including meta-analyses, point to several cancers as exhibiting inverse associations with metformin use: pancreatic cancer36, hepatocellular carcinoma (HCC)36,59, colorectal cancer59, lung cancer59 and breast cancer60,61.
Breast cancer. Two successes in breast cancer prevention agents involve the selective oestrogen receptor modulators (SERMs) tamoxifen and raloxifene. Each SERM has been approved by the US Food and Drug Administration (FDA) for risk reduction of breast cancer in high-risk women based on results from large Phase III randomized control trials (RCTs)62,63,64,65. Raloxifene offers a classic example of re-purposing a drug that was developed for the prevention and treatment of another disease — osteoporosis — to cancer prevention. In 2006, the first analysis of the Study of Tamoxifen and Raloxifene (STAR) indicated equivalent efficacy of raloxifene compared with tamoxifen for breast cancer risk reduction, ultimately leading to the approval of raloxifene for this purpose64. Although a follow-up analysis has revealed a trend towards a reduced efficacy of raloxifene versus tamoxifen65, raloxifene is less toxic, it does not increase the risk of endometrial cancer and its adverse effect on thromboembolic disease is lower than that of tamoxifen.
Concerns about the SERMs have inspired continued research into identifying agents that resemble the SERMs for decreasing breast cancer risk (48% decrease in oestrogen receptor-positive breast cancer) but that do so with lower toxicities than the SERMs. A promising class of drugs, the aromatase inhibitors, which inhibit oestrogen production, was known from adjuvant trials to decrease the incidence of oestrogen receptor-positive contralateral breast cancers by 40% to 50%66. This led to the testing of the third-generation aromatase inhibitors exemestane and anastrozole in Phase III primary prevention RCTs that compared the aromatase inhibitor with a placebo in high-risk postmenopausal women. In the National Cancer Institute of Canada (NCIC) Mammary Prevention 3 (MAP.3) trial, exemestane led to a 65% reduction in the annual incidence of invasive breast cancer and a 73% reduction in oestrogen receptor-positive breast cancers relative to a placebo in high-risk women67. Expected toxicities, which relate to reduced bone density, fractures and other musculoskeletal side effects, were limited according to the initial publication. However, not only was the 35-month follow-up time too short to allow the adverse event data to mature, but key anticipated bone-related events, as well as other toxicities were not prospectively included as study end points68.
Colon and other gastrointestinal cancers. Multiple trials that have tested aspirin for its cancer-preventive effect using colorectal adenomas as a surrogate primary end point for cancer have shown benefits for the use of this non-steroidal anti-inflammatory drug (NSAID) in reducing the risk of colorectal cancer (CRC). For example, in patients with a history of a previous CRC69 or a history of colorectal adenomas70,71, the incidence of new adenomas was reduced in those taking aspirin versus those taking no aspirin. In the Colorectal Adenoma/Carcinoma Prevention Programme (CAPP2) trial in patients with hereditary CRC (Lynch syndrome), the long-term effects of aspirin use, determined using an intent-to-treat analysis to first CRC, indicated a hazard ratio (HR) of 0.63 (95% CI = 0.35−1.13; p = 0.12)72.
Recent post-hoc analyses and meta-analyses from multiple randomized clinical trials that were originally designed with non-cancer end points found that, after a minimum of 5 years of follow-up, trial participants who took aspirin daily — regardless of dose — for a mean of 4 years, had a 44% reduction in cancer mortality compared with participants who took a placebo. The largest decrease in risk was for gastrointestinal cancers (oesophageal and colorectal adenocarcinoma)73,74,75. Data for individual participants in three of the eight trials showed a lower risk of cancer-associated mortality after 20 years of follow-up73.
In addition to aspirin, other NSAIDs have shown efficacy in CRC prevention trials. Celecoxib, a selective inhibitor of cyclooxygenase 2 (COX2), proved promising for inhibiting adenoma occurrence in patients with familial adenomatous polyposis (FAP)76 and in patients following polypectomy77,78. However, COX2 inhibitors are no longer considered for prevention owing to their cardiovascular toxicities79,80,81. Despite this, other NSAIDs show promise, including sulindac, for which 375 individuals with a history of resected adenomas were randomized to take either sulindac plus difluoromethylornithine (DFMO) or matched placebos. The risk ratio for recurrent adenomas in the intervention relative to the placebo group was 0.30 (95% CI = 0.18−0.49; p <0.001) and 0.085 (95% CI = 0.011–0.65; p <0.001) for advanced adenomas82. These remarkable results have led to an ongoing Phase III trial (NCT01349881; see Further information). Together, these studies strongly suggest a role for aspirin and other NSAIDs in colon cancer risk reduction.
Prostate cancer. Prostate cancer, the most common cancer and the second leading cause of cancer-related death in men, has been the subject of a number of large prevention trials over the past three decades. Although they fostered a better understanding of the disease and strategies for reducing incidence, unexpected results from past trials, including SELECT, have raised troubling questions regarding preventive interventions for prostate cancer.
Prostate cancer prevention efforts with the 5-α-reductase inhibitors finasteride and dutasteride, two agents used for benign prostatic hyperplasia, have encountered other obstacles. The Prostate Cancer Prevention Trial (PCPT) showed that finasteride compared with a placebo reduced the risk of prostate cancer in healthy men by 25%. However, a 27% increase in high-grade tumours (Gleason grades 7−10) was observed in the treated group relative to the placebo group when the comparison was made in terms of the percentage of high-grade tumours among all men in the study83. The Reduction by Dutasteride of Prostate Cancer Events (REDUCE) trial in men at a high risk of prostate cancer based on increased levels of prostate-specific antigen (PSA) showed a similar reduction in prostate cancer risk (relative risk reduction of 22.8% (95% CI = 15.2–29.8; p <0.001). Again, a slight increase in high-grade tumours was noted in individuals taking dutasteride compared with a placebo84.
Attempts to explain the unexpected increase in high-grade tumours in the otherwise promising results from the PCPT and REDUCE trials, as well as other trials, have engendered considerable commentary, influencing future directions for prostate cancer prevention research85,86. The observed reductions in prostate cancer prevalence (PCPT) and incidence (REDUCE) suggest that the identification of the men that are most likely to benefit from cancer prevention would optimize the use of 5-α-reductase inhibitors. Research has indicated variability in the CYP3A4 genotypes and haplotypes that correlate with CYP3A4 enzyme activity, which affects testosterone metabolism and ultimately has implications for prostate cancer risk. For example, ethnic differences in CYP3A4*1B allele frequencies correlate with the risk of prostate cancer: Asian men (0%*1B), have the lowest risk, followed by Caucasian men (7%*1B), Hispanic men (20%*1B) and finally African American men (81%*1B), who have the highest risk. As with risk, responses to a drug may be predicted by the pharmacogenetics of finasteride-metabolizing and target enzymes, and this offers a fertile area for investigation87. A key approach would be based on biomarkers such as genetic variants in genes encoding enzymes, such as CYP3A4, which are involved in the biotransformation of 5-α-reductase inhibitors, as well as SRD5A2, which is the target of drugs in this class87. In addition, lifestyle interventions for reducing the risk of prostate cancer are focused on the role of obesity and physical activity88.
Application of effective chemopreventive agents in general clinical use. Despite promising outcomes from clinical trials of chemopreventive agents, potential agents still face challenges in terms of being brought to generalized clinical use. The first challenge is to engage the interest of pharmaceutical companies for the purpose of chemoprevention. With a few exceptions (tamoxifen, raloxifene, dutasteride, finasteride, celecoxib and others), these companies have not viewed the necessary drug development process in a favourable light owing to a lack of anticipated financial benefits in the preventive setting. Necessary Phase III trials are resource intensive (large, long and expensive) and are unlikely to pay off in terms of widespread uptake into general clinical use even if they are approved for preventive indications by the FDA. The FDA itself poses obstacles because of intense scrutiny for toxicity, a huge hurdle for drugs to be administered in a non-cancer population. A telling example of the objection of the FDA to a preventive application is finasteride. The PCPT demonstrated that eligible healthy men taking finasteride for 5 years exhibited nearly a 25% reduction in the prevalence of prostate cancer compared with men taking a placebo83. This promising outcome was far out-shadowed from the viewpoint of the FDA by the 27% increase in high-grade cancers (Gleason grades 7–10) in men in the finasteride (6.4%) group compared with men in the placebo (5.1%) group. An additional impediment to bringing chemoprevention agents into clinical use is the perception of the public regarding the toxicities associated with these agents. This is particularly well illustrated by tamoxifen, which successfully survived FDA approval for the purpose of risk reduction in high-risk women based on the outcomes from the Breast Cancer Prevention Trial (BCPT)89. Despite FDA approval, uptake by high-risk women and their physicians of preventive tamoxifen has been very limited90,91. Finally, in the case of commonly used drugs that are approved for other indications, completing large definitive clinical trials is not feasible. For example, although extensive epidemiological74,75 and clinical69,70,72,82,92 evidence supports cancer-preventive effects for aspirin, its important role in cardiovascular preventive measures93 precludes placebo-controlled clinical testing of this agent for chemoprevention.
Immunotherapy for cancer prevention
Vaccines are prominent among the approaches that aim to harness an individual's immune system against cancer, showing greater success in cancer prevention than treatment (Tables 2,3). The preferential success of preventive vaccination is generally attributable to a minimal or non-existent tumour burden. In addition, candidates for preventive vaccination still have fully competent immune systems that are capable of developing robust antitumour responses, leading to the eradication of abnormal cells and/or the prevention of disease onset and recurrence.
Endogenous immune responses can be recruited to prevent cancer via three basic approaches: using vaccines to prevent infection with cancer-associated agents; using vaccines to target tumour-associated antigens (TAAs) or tumour-specific antigens; and using nonspecific immunomodulators that recruit components of the innate immune system to exert their anticancer effect.
Vaccines against oncogenic infectious agents. The most obvious successes involve the development of vaccines that prevent cancer by inhibiting the onset of factors that are known to initiate carcinogenesis. Preventing infection with cancer-causing viruses offers a case in point. The identification of hepatitis B virus (HBV) as a major cause of HCC94 instigated an effort to develop an HBV vaccine. The use of a prophylactic vaccine based on purified S particles from the virus in high-risk individuals has led to an estimated 69% reduction in the incidence of HBV-specific HCC worldwide. The next step will be to develop HBV and HCV therapeutic vaccines for cancer prevention in individuals that are already infected (Table 2).
A similar trajectory has transpired in recent years for cervical cancer, which is induced through infection with specific strains of the human papillomavirus (HPV). Two highly effective vaccines that target the L1 protein, a component of the outer shell of the virus, have been developed and licensed94,95. In the United States and the European Union, Gardisil (Merck), which targets HPV strains 6 and 11, and the oncogenic strains 16 and 18, was approved in 2006 for young females aged 9–26. In 2009 the FDA approved Cervarix (GlaxoSmithKline), which targets HPV-16 and HPV-18, for females aged 10–25. However, several issues remain unresolved, such as the actual duration of vaccine efficacy in preventing infection and the need to develop vaccines that target a broader range of both oncogenic and non-oncogenic HPV strains. Although less than 25% of HPV-associated cancers occur in men overall, some subgroups are particularly susceptible to such cancers96. Specifically, 90% of anal cancers are HPV-related, and according to recent data a steady increase has been occurring in HPV-positive orophayrngeal cancer in men97. Together, these observations suggest that addressing a broader reach of HPV vaccines, beyond that of cervical cancer, would be valuable. Thus, current interest in the HPV vaccines now centres on extending coverage to boys96,98. Additional efforts are underway to develop an HPV vaccine that can cure previously infected individuals, including those with existing pre-malignant lesions99. This cohort represents a majority of men and women above the age of 11 (Refs 100,101). Although HPV vaccines seem to exhibit reduced efficacy in individuals with prior exposure to HPV96, modelling analysis of their cost effectiveness suggests that vaccination is a beneficial intervention in high-risk men for the prevention of genital warts, and oropharyngeal and anal cancer98. Importantly, not all oncogenic strains of HPV are covered by current prophylactic vaccines; hence, a need still exists for Papanicolaou tests (Pap smears), as the remaining uncovered strains will continue to pose an oncogenic challenge to the cervix until newer multivalent vaccines are developed that cover all strains.
Vaccines directed against tumour antigens. Tumour antigens are endogenous (or self) proteins that are aberrantly expressed102. Tumour-specific antigens are expressed only in cancer cells and germ cells. By contrast, tumour-associated antigens (TAAs) occur normally in adult somatic cells but are modified in cancer cells. The mechanisms responsible for the transition of these normal cell regulatory proteins to aberrant (abnormal self), and thus immunogenic proteins in malignant cells, are not fully understood. Several possible explanations have been proposed, including the acquisition of stable mutations (as is evident in the melanoma antigen MAGE1); overexpression of the tumour-associated protein (such as ERBB2 (also known as HER2 and neu)), revealing additional epitopes that are not routinely exposed; and through the post-translational modification of a normal self-antigen, as is seen with abnormal glycosylation of MUC1 in colon cancer103 (Table 3).
The intactness of the immune system in healthy, high-risk individuals who are in need of preventive interventions makes them ideal candidates for prevention vaccines. In addition, pre-cancers are smaller lesions, which are more likely to be controlled by an effective immune response. Both of these facts argue that immunological approaches may be better suited to cancer prevention or for early stage treatment, than for the treatment of late-stage cancers. Impressive preclinical evidence that supports the immunological effects of preventive vaccines comes from a mouse model of colitis-associated colon cancer (CACC). MUC1 is abnormally expressed in inflammatory bowel disease (IBD), as it is in colon cancers104. Vaccination against MUC1 not only delayed IBD but also prevented progression to CACC in this mouse model, at least in part by eliciting MUC1-specific adaptive immunity, which eliminated abnormal MUC1-expressing cells in IBD colons. Following vaccination in patients with breast cancer, T cell (both CD4+ and CD8+ T cells) immunity to three TAAs that are typically found in tumour tissue (ERBB2, carcinoembryonic antigen (CEA) and melanoma-associated protein 3(MAGE3)) was increased relative to controls103. Such antigen-specific cancer vaccines targeting these TAAs have been shown to elicit tumour-suppressive responses in the clinical setting. Admittedly, the responses were incomplete, but they offer proof-of-principle for this approach in preventing invasive disease. A large number of clinical trials have been carried out using different TAAs and most have shown minimal toxicities and side effects that are common with any vaccinations105,106,107.
Non-targeted immunological preventive interventions. In addition to interventions that are targeted to specific antigens, agents that elicit nonspecific immunological responses have proved useful in preventing the initiation and/or progression of carcinogenesis. Some of these non-targeted immunomodulators have already been approved by the FDA for use in cancer prevention. One success with a non-targeted intervention is imiquimod (Aldara; Graceway Pharmaceuticals). Imiquimod, and a sister compound, resiquimod (R-848; Biovision), both activate the innate immune system through the toll-like receptors TLR7 and TLR8. Imiquimod applied topically was originally approved by the FDA to treat actinic keratosis, superficial basal cell carcinoma and external genital warts. Imiquimod has yielded an 80% cure rate for lentigo maligna and has shown efficacy in vulvar intraepithelial neoplasia108. A recent, small clinical trial of imiquimod showed benefit as an adjunct to surgery for high-risk, primary melanoma109. Like other TLR agonists, imiquimod has been shown to enhance antitumour activity in an adjuvant manner when combined with a viral vector vaccine, specifically an adeno-associated virus carcinoembryonic antigen (CEA) vaccine110.
Carrageenans, a family of linear sulphated polysaccharides from red algae that are related to heparan sulphate, possess nonspecific immunomodulatory properties, activating macrophages and inducing pro-inflammatory cytokines through the BCL-10–NF-κB–interleukin-8 (IL-8) pathway111,112. Carrageenans bind TLR4, conferring their immunological effect via an innate immune response. In vitro and animal studies have suggested that carrageenans may be potent inhibitors of HPV infection113. A clinical trial of Carraguard (FMC Biopolymer), a carrageenan-based lubricant, in 1,723 high-risk, sexually active women, showed a reduction in HPV infection among women using the lubricant compared with those who did not114. This ability to protect against vaginal transmission of HPV suggests a role for this nonspecific immunomodulator in the prevention of HPV-associated cancers.
Immunostimulatory drugs have long been used for the treatment of cancer and other diseases. Instillation of the Bacillus Calmette–Guérin (BCG) into the bladder is an established treatment for preventing the recurrence of superficial bladder cancer115. Long-term follow-up of patients with high-grade T1 bladder cancer indicated a benefit from this nonspecific immunomodulation after transurethral resection116, although long-term follow-up (>3 years) demonstrated progression in 30% of patients. The ability to predict which patients will develop recurrent disease should improve the use of this approach. A study of BCG response biomarkers identified urinary IL-2 as a promising predictive biomarker of BCG response117.
Several drugs, such as ipilimumab, have been developed that target distinct regulatory elements of the immune system. Cytotoxic T lymphocyte antigen 4 (CTLA4), which belongs to the immunoglobulin superfamily, is expressed on the surface of T helper cells and transmits inhibitory signals to T cells, preventing the over-activation and prolongation of an immune response. Although early clinical studies show promise for this approach in patients with advanced cancer, there is considerable concern that such agents will have unacceptable side effects, including autoimmune reactions in healthy individuals with an intact, fully functional immune system. Further research is undoubtedly needed in this area, although initial findings have indicated that targeting another T cell inhibitory molecule, PD1, might have reduced side effects118.
Cancer immunoprevention
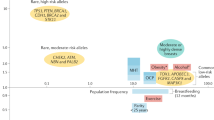
In general, biomarkers are physical entities or images of these entities or other indirect manifestations of a physiological state that indicate the presence of a biological process, disease process or drug response119. Biomarkers can serve several purposes in clinical trial testing of potential cancer-preventive interventions (Fig. 3). Biomarkers can be used to assess the risk of developing cancer, as seen with genetic mutations (such as BRCA1, BRCA2 and APC in specific cancer-associated syndromes) and genetic polymorphisms and variants, which are revealed via epidemiological and genome-wide association studies. Imaging modalities are also currently being used to assess risk. For example, breast density on mammograms120 is being used in some clinical trials to assess the risk of breast cancer for the purposes of trial eligibility66.

In cancer medicine biomarkers have been used for several purposes. Risk biomarkersreflect the increased risk of developing a cancer type or subtype. In genetic syndromes, a gene mutation in the germline DNA correlates with an increased risk of disease; the same mutation is observed in all tissues of the affected individual. Pre-malignant lesions serve as tissue indicators of increased risk of progression to cancer. Such risk biomarkers can be used for risk classification or risk stratification, which quantifies the level of risk and/or separates at-risk individuals into categories on the basis of predicted response to a given treatment. Risk stratification is useful in designing clinical trials that involve individualized treatment interventions. Predictive biomarkerspredict the likelihood of drug response, specifically the likelihood that a precancer will respond to a mechanism-based therapy that is targeted to that lesion. Surrogate end point biomarkers (SEBs) are used as substitutes for key clinical outcomes; modulation of SEBs in response to drug or other interventions should be in a direction that parallels the desired response of the clinical end point.
Few biomarkers have been validated for the early detection of cancer. Among those most widely used are PSA for prostate cancer, cancer antigen (CA)-125 for ovarian and cervical cancer, CA 19–9 for pancreatic cancer, carcinoembryonic antigen (CEA) for colon cancer and α-fetoprotein (AFP) for liver cancer121. However, these biomarkers are far from optimal with respect to two key elements that are required of a validated screening marker: sensitivity and specificity. Considerable controversy exists regarding their application in the early detection of cancer.
As a result of recent advances in our understanding of molecular carcinogenesis, several molecular biomarkers have been developed for prognostic use, as well as for risk stratification and decision-making as to whether to incorporate chemotherapy into the therapeutic regimen. Biomarkers used in this manner include the Oncotype DX (Genomic Health Inc) and ColoPrint (Agendia) for colorectal cancer122, and the Oncotype DX and MammaPrint (Agendia) tests for early stage breast cancer123,124. Future cancer prevention trials will use some variations of these multi-gene arrays to assist in deciding whether specific interventions should be used based on both risk stratification and minimizing overall toxicity in high-risk individuals. The process of developing and validating biomarkers is long and rigorous, and few biomarkers have so far been validated for their intended application, whether for early detection, prognosis or prediction of drug response.
Future directions in cancer prevention
Continued interest in established classes of chemopreventive agents. Given the well-documented chemopreventive properties of both SERMs and aromatase inhibitors, interest continues in testing newer hormone-modulating agents for cancer prevention62. Two doses of the non-steroidal SERM lasofoxifene were compared with a placebo in osteoporotic women in the Postmenopausal Evaluation and Risk-Reduction with Lasofoxifene (PEARL) trial125,126. Not only did both lasofoxifene doses reduce fracture risk but they also reduced the risk of oestrogen receptor-positive breast cancer (0.5 mg per day (81% reduction; p <0.001); 0.25 mg per day (48% reduction; p = 0.07))125, making this a promising agent for breast cancer prevention. Similarly, the SERM arzoxifene was shown in the Generations Trial involving osteopenic and osteoporotic postmenopausal women to reduce invasive breast cancer incidence by 1.3% (cumulative rate = 1.0% with arzoxifene versus 2.3% with a placebo), giving a 56% relative decrease in risk (HR = 0.44 (95% CI = 0.26−0.76; p >0.001))127. Even as the MAP.3 trial documented the benefits of exemestane in prevention, aromatase inhibitors continue to be under investigation for breast cancer risk reduction. Results from the International Breast Cancer Intervention Study II (IBIS-II) are eagerly awaited. This two-group trial is comparing the aromatase inhibitor anastrozole to a placebo in women at an increased risk of breast cancer (first group) and anastrozole to tamoxifen in women with ductal carcinoma in situ (second group). An interesting feature of the high-risk group is the inclusion among the eligibility criteria of high mammographic density, a well-documented risk factor for breast cancer11,66,128. In addition to serving as a documented biomarker of cancer risk, data are accumulating to support mammographic density both as a surrogate end point biomarker of drug effect and as a predictive biomarker of clinical drug efficacy when evaluated with tamoxifen and aromatase inhibitors in women with high breast density at baseline129,130. Although a study of raloxifene in high-risk premenopausal women did not reveal a change in mammographic density with this agent131, the design and small size of this study precluded the evaluation of clinical response correlates of mammographic density. Clearly, the potential application of baseline mammographic density as a predictive biomarker should be investigated in the future in relation to the efficacy of other breast cancer risk-reducing agents.
Individualized cancer prevention. Just as genomic analyses of various cancers have been undertaken as part of The Cancer Genome Atlas (TCGA) project, attention is now being directed towards analogous genomic probing of pre-malignant lesions. Evaluation of the genetic abnormalities is expected to promote a gene-based functional understanding of carcinogenesis and lead to the identification of molecular targets for interventions. In addition to genomics, cancer prevention strategies in the future will incorporate a variety of new modalities, including imaging, proteomic, metabolomic, glycomic and epigenetic, to identify, and validate, surrogate biomarkers for use in Phase I and II prevention trials.
Overdiagnosis, underdiagnosis and risk stratification.Overdiagnosis of cancerous lesions the clinical significance of which is undetermined provides a great challenge for the screening and cancer prevention community132. In addition, screening can identify pre-cancers the clinical relevance of which is also unknown. The problem is further complicated by the fact that not only are pre-cancers of undetermined significance being identified at an alarmingly high rate, partly due to improvement in detection technologies, but the lesions that are ultimately destined to progress to cancer are also either not diagnosed or are hidden in these myriad pre-cancers; this situation is a form of underdiagnosis. This is exemplified in the case of Barrett's oesophagus and oesophageal adenocarcinoma. Although individuals with Barrett's oesophagus are at a high risk of developing oesophageal adenocarcinoma, 95% of patients with Barrett's oesophagus never develop cancer. Conversely, most oesophageal adenocarcinoma cases were missed as they were diagnosed as Barrett's oesophagus133. Genomic analysis resembling TCGA-like projects offers a crucial approach for discerning which of the screen-diagnosed pre-cancerous and small invasive lesions pose actual threats to the health of individuals. Distinguishing these from lesions that are benign and innocuous, or that are overdiagnosed, would avoid morbid and costly follow-up medical intervention in individuals whose newly revealed lesions are predicted never to progress based on genomic classification.
Immunoprevention modalities. Cancer prevention is ideal for interventions involving the modulation of the immune response. The small size of pre-invasive lesions that confer high cancer risk combined with the robust nature of the immune system, promise better success with immune modalities in preventive as opposed to treatment settings. Vaccines, already well-established tools for preventing a variety of infectious diseases, have been applied to the prevention of some of the 20% of cancers that are known to have infectious aetiologies. Building on past successes with prophylactic HBV and HPV vaccines, research is beginning to address the cancer-preventive effects of therapeutic vaccines in individuals who are already infected with oncogenic viruses. In the near future, an important application of successful vaccines, such as those for HPV and HBV, will be to direct their use in developing countries, which lack resources for standard-of-care treatment of infection-associated (and other) cancers. The immune evasiveness of highly mutable cancer-causing viruses poses a special challenge to vaccine development, but improved understanding of the immune system should allow this obstacle to be overcome.
Similarly, the identification of tumour antigens in pre-cancers and a better understanding of innate immune surveillance during carcinogenesis is needed so that future research can be better defined for immunomodulatory approaches, including combinations of small molecules that modulate the immune response.
Adaptive and creative clinical trials for cancer prevention. Whereas past definitive Phase III prevention trials have served us well in documenting or rejecting the efficacy of promising preventive interventions for high-risk individuals21,22,64,65,83,89,134, the necessarily large size of such trials requires substantial investment of both monetary and human resources. For these reasons, alternative designs for definitive clinical prevention trials, aiming for shorter intervention durations and smaller participant cohorts, are beginning to be investigated. Future large prevention trials should be prospectively designed to cut across multiple disease entities in a manner resembling the Women's Health Initiative135. In addition, more efficient approaches to the development of cancer-preventive agents from in vitro testing, through in vivo animal model evaluation to clinical trials are currently being explored136.
Public health education and community outreach. Finally, a major challenge for prevention is improving the methods of communicating research results to the public. Despite strong evidence from well-designed Phase III trials that the SERMs tamoxifen and raloxifene are effective risk-reducing agents for breast cancer, as well as FDA approval and endorsement by respected professional organizations for this indication137,138, the acceptability of preventive tamoxifen and raloxifene to high-risk women and their physicians has been limited, primarily owing to concerns over perceived unacceptable toxicity36,90,139,140. This misunderstanding by the public is due to a number of factors: an inadequate communication of the risks and benefits by clinical researchers; a lack of integration of cancer prevention into the education of primary care providers, who comprise the clinical frontline in disease prevention; and an exaggeration of the adverse effects by the mass media. In addition, underserved populations suffer from a lack of access to cutting edge health information in general. Methods to improve the communication of the actual risk to benefit balance of preventive drugs for individual patients must be developed91. If physicians and other health professionals are to increase the use of cancer-preventive agents, whether drugs, nutrients or vaccines, a clear message must be given that the benefits far outweigh the identified side effects, especially if medical professionals are to be successful in recommending these interventions to otherwise healthy individuals.
References
Bray, F., Ren, J. S., Masuyer, E. & Ferlay, J. Global estimates of cancer prevalence for 27 sites in the adult population in 2008. Int. J. Cancer 26 Jul 2012 (doi:10.1002/ijc.27711).
Jemal, A. et al. Global cancer statistics. CA Cancer J. Clin. 61, 69–90 (2011).
Lippman, S. M. & Hawk, E. T. Cancer prevention: from 1727 to milestones of the past 100 years. Cancer Res. 69, 5269–5284 (2009).
Greenwald, P. & Dunn, B. K. Landmarks in the history of cancer epidemiology. Cancer Res. 69, 2151–2162 (2009). A comprehensive history of the landmarks in cancer epidemiology from 1900 to 2008.
Hanahan, D. & Weinberg, R. A. The hallmarks of cancer. Cell 100, 57–70 (2000).
Hanahan, D. & Weinberg, R. A. Hallmarks of cancer: the next generation. Cell 144, 646–674 (2011). Presents the hallmarks of cancer that constitute an organizing principle for understanding the complexities of neoplastic disease.
Schreiber, R. D., Old, L. J. & Smyth, M. J. Cancer immunoediting: integrating immunity's roles in cancer suppression and promotion. Science 331, 1565–1570 (2011). An overview of the dual role that immunoediting has in promoting and suppressing tumour growth.
William, W. N. Jr, Heymach, J. V., Kim, E. S. & Lippman, S. M. Molecular targets for cancer chemoprevention. Nature Rev. Drug Discov. 8, 213–225 (2009).
Chai, H. & Brown, R. E. Field effect in cancer-an update. Ann. Clin. Lab Sci. 39, 331–337 (2009).
Albini, A., Tosetti, F., Li, V. W., Noonan, D. M. & Li, W. W. Cancer prevention by targeting angiogenesis. Nature Rev. Clin. Oncol. 9, 498–509 (2012).
Assi, V., Warwick, J., Cuzick, J. & Duffy, S. W. Clinical and epidemiological issues in mammographic density. Nature Rev. Clin. Oncol. 9, 33–40 (2012).
Doll, R. & Peto, R. The causes of cancer: quantitative estimates of avoidable risks of cancer in the United States today. J. Natl Cancer Inst. 66, 1191–1308 (1981).
Willett, W. C. Diet and cancer: one view at the start of the millennium. Cancer Epidemiol. Biomarkers Prev. 10, 3–8 (2001).
World Bank & World Health Organization. Tobacco Control in Developing Countries (Oxford Univ. Press, 2000).
Gibson, T. M., Ferrucci, L. M., Tangrea, J. A. & Schatzkin, A. Epidemiological and clinical studies of nutrition. Semin. Oncol. 37, 282–296 (2010).
Umar, A. & Greenwald, P. Alarming colorectal cancer incidence trends: a case for early detection and prevention. Cancer Epidemiol. Biomarkers Prev. 18, 1672–1673 (2009).
Prentice, R. L. et al. Low-fat dietary pattern and cancer incidence in the Women's Health Initiative Dietary Modification Randomized Controlled Trial. J. Natl Cancer Inst. 99, 1534–1543 (2007).
World Cancer Research Fund/American Institute for Cancer Research. Food, Nutrition, Physical Activity, and the Prevention of Cancer: a Global Perspective. (American Institute for Cancer Research, 2007).
Davis, C. D., Emenaker, N. J. & Milner, J. A. Cellular proliferation, apoptosis and angiogenesis: molecular targets for nutritional preemption of cancer. Semin. Oncol. 37, 243–257 (2010).
Gullett, N. P. et al. Cancer prevention with natural compounds. Semin. Oncol. 37, 258–281 (2010). A comprehensive review of natural compounds that exhibit cancer-preventive properties.
Lippman, S. M. et al. Effect of selenium and vitamin E on risk of prostate cancer and other cancers: the Selenium and Vitamin E Cancer Prevention Trial (SELECT). JAMA 301, 39–51 (2009).
Klein, E. A. et al. Vitamin E and the risk of prostate cancer: the Selenium and Vitamin E Cancer Prevention Trial (SELECT). JAMA 306, 1549–1556 (2011).
Clark, L. C. et al. Effects of selenium supplementation for cancer prevention in patients with carcinoma of the skin. A randomized controlled trial. Nutritional Prevention of Cancer Study Group. JAMA 276, 1957–1963 (1996).
Dunn, B. K., Richmond, E. S., Minasian, L. M., Ryan, A. M. & Ford, L. G. A nutrient approach to prostate cancer prevention: the Selenium and Vitamin E Cancer Prevention Trial (SELECT). Nutr. Cancer 62, 896–918 (2010). A comprehensive discussion of the negative results of the SELECT prostate cancer prevention trial, and what that means for the future of selenium and vitamin E for cancer prevention.
Dunn, B. K., Ryan, A. & Ford, L. G. Selenium and Vitamin E Cancer Prevention Trial: a nutrient approach to prostate cancer prevention. Recent Results Cancer Res. 181, 183–193 (2009).
Calle, E. E., Rodriguez, C., Walker-Thurmond, K. & Thun, M. J. Overweight, obesity, and mortality from cancer in a prospectively studied cohort of U.S. adults. N. Engl. J. Med. 348, 1625–1638 (2003).
Subbaramaiah, K. et al. Obesity is associated with inflammation and elevated aromatase expression in the mouse mammary gland. Cancer Prev. Res. 4, 329–346 (2011).
Morris, P. G. et al. Inflammation and increased aromatase expression occur in the breast tissue of obese women with breast cancer. Cancer Prev. Res. 4, 1021–1029 (2011).
Vander Heiden, M. G., Cantley, L. C. & Thompson, C. B. Understanding the Warburg effect: the metabolic requirements of cell proliferation. Science 324, 1029–1033 (2009).
Hamanaka, R. B. & Chandel, N. S. Cell biology. Warburg effect and redox balance. Science 334, 1219–1220 (2011).
Braun, S., Bitton-Worms, K. & LeRoith, D. The link between the metabolic syndrome and cancer. Int. J. Biol. Sci. 7, 1003–1015 (2011).
Lazar, M. A. & Birnbaum, M. J. Physiology. De-meaning of metabolism. Science 336, 1651–1652 (2012).
Giovannucci, E. Nutrition, insulin, insulin-like growth factors and cancer. Horm. Metab. Res. 35, 694–704 (2003).
Hankinson, S. E. et al. Circulating concentrations of insulin-like growth factor-I and risk of breast cancer. Lancet 351, 1393–1396 (1998).
Pollak, M. The insulin and insulin-like growth factor receptor family in neoplasia: an update. Nature Rev. Cancer 12, 159–169 (2012). In-depth discussion of the relationship between diabetes, metabolic syndrome, insulin–IGF axis and cancer risk.
Decensi, A. et al. Metformin and cancer risk in diabetic patients: a systematic review and meta-analysis. Cancer Prev. Res. 3, 1451–1461 (2010). A meta-analysis that indicated the most commonly used medication for diabetes may have cancer-prevention properties.
Engelman, J. A. & Cantley, L. C. Chemoprevention meets glucose control. Cancer Prev. Res. 3, 1049–1052 (2010).
Gonzalez-Angulo, A. M. & Meric-Bernstam, F. Metformin: a therapeutic opportunity in breast cancer. Clin. Cancer Res. 16, 1695–1700 (2010).
Kisfalvi, K., Eibl, G., Sinnett-Smith, J. & Rozengurt, E. Metformin disrupts crosstalk between G protein-coupled receptor and insulin receptor signaling systems and inhibits pancreatic cancer growth. Cancer Res. 69, 6539–6545 (2009).
Knowler, W. C. et al. Reduction in the incidence of type 2 diabetes with lifestyle intervention or metformin. N. Engl. J. Med. 346, 393–403 (2002).
Fradkin, J. E., Roberts, B. T. & Rodgers, G. P. What's preventing us from preventing type 2 diabetes? N. Engl. J. Med. 367, 1177–1179 (2012).
Pal, A. et al. PTEN mutations as a cause of constitutive insulin sensitivity and obesity. N. Engl. J. Med. 367, 1002–1011 (2012).
Pilarski, R. Cowden syndrome: a critical review of the clinical literature. J. Genet. Couns. 18, 13–27 (2009).
Dirx, M. J., Zeegers, M. P., Dagnelie, P. C., van den Bogaard, T. & van den Brandt, P. A. Energy restriction and the risk of spontaneous mammary tumors in mice: a meta-analysis. Int. J. Cancer 106, 766–770 (2003).
Pallavi, R., Giorgio, M. & Pelicci, P. G. Insights into the beneficial effect of caloric/ dietary restriction for a healthy and prolonged life. Front. Physiol. 3, 318 (2012).
Willcox, D. C., Willcox, B. J., Todoriki, H. & Suzuki, M. The Okinawan diet: health implications of a low-calorie, nutrient-dense, antioxidant-rich dietary pattern low in glycemic load. J. Am. Coll. Nutr. 28, 500S–516S (2009).
Dirx, M. J., van den Brandt, P. A., Goldbohm, R. A. & Lumey, L. H. Energy restriction early in life and colon carcinoma risk: results of The Netherlands Cohort Study after 7.3 years of follow-up. Cancer 97, 46–55 (2003).
Marteau, T. M., Hollands, G. J. & Fletcher, P. C. Changing human behavior to prevent disease: the importance of targeting automatic processes. Science 337, 1492–1495 (2012).
Courneya, K. S. & Friedenreich, C. M. Physical activity and cancer: an introduction. Recent Results Cancer Res. 186, 1–10 (2011).
Physical Activity Guidelines Advisory Committee. Physical Activity Guidelines Advisory Committee Report, 2008. (U.S. Department of Health and Human Services, 2008).
Siegel, R. et al. Cancer treatment and survivorship statistics, 2012. CA Cancer J. Clin. 62, 220–241 (2012).
Friedenreich, C. M. The role of physical activity in breast cancer etiology. Semin. Oncol. 37, 297–302 (2010).
Ballard-Barbash, R. et al. Physical activity, biomarkers, and disease outcomes in cancer survivors: a systematic review. J. Natl Cancer Inst. 104, 815–840 (2012).
Sporn, M. B., Dunlop, N. M., Newton, D. L. & Smith, J. M. Prevention of chemical carcinogenesis by vitamin A and its synthetic analogs (retinoids). Fed. Proc. 35, 1332–1338 (1976).
Lippman, S. M. & Heymach, J. V. The convergent development of molecular-targeted drugs for cancer treatment and prevention. Clin. Cancer Res. 13, 4035–4041 (2007).
Greenwald, P., Kelloff, G., Burch-Whitman, C. & Kramer, B. S. Chemoprevention. CA Cancer J. Clin. 45, 31–49 (1995).
Kelloff, G. J. et al. Progress in chemoprevention drug development: the promise of molecular biomarkers for prevention of intraepithelial neoplasia and cancer-a plan to move forward. Clin. Cancer Res. 12, 3661–3697 (2006).
Nathan, D. M. et al. Medical management of hyperglycaemia in type 2 diabetes mellitus: a consensus algorithm for the initiation and adjustment of therapy: a consensus statement from the American Diabetes Association and the European Association for the Study of Diabetes. Diabetologia 52, 17–30 (2009).
Noto, H., Goto, A., Tsujimoto, T. & Noda, M. Cancer risk in diabetic patients treated with metformin: a systematic review and meta-analysis. PLoS ONE 7, e33411 (2012).
Bodmer, M., Meier, C., Krahenbuhl, S., Jick, S. S. & Meier, C. R. Long-term metformin use is associated with decreased risk of breast cancer. Diabetes Care 33, 1304–1308 (2010).
Goodwin, P. J. et al. Evaluation of metformin in early breast cancer: a modification of the traditional paradigm for clinical testing of anti-cancer agents. Breast Cancer Res. Treat. 126, 215–220 (2011).
Arun, B., Dunn, B. K., Ford, L. G. & Ryan, A. Breast cancer prevention trials: large and small trials. Semin. Oncol. 37, 367–383 (2010). A review of past prevention trials in breast cancer with an emphasis on uses of this knowledge in designing future trials.
Cuzick, J. et al. Overview of the main outcomes in breast-cancer prevention trials. Lancet 361, 296–300 (2003).
Vogel, V. G. et al. Effects of tamoxifen versus raloxifene on the risk of developing invasive breast cancer and other disease outcomes: the NSABP Study of Tamoxifen and Raloxifene (STAR) P-2 trial. JAMA 295, 2727–2741 (2006).
Vogel, V. G. et al. Update of the National Surgical Adjuvant Breast and Bowel Project Study of Tamoxifen and Raloxifene (STAR) P-2 Trial: preventing breast cancer. Cancer Prev. Res. 3, 696–706 (2010).
Cuzick, J. Aromatase inhibitors for breast cancer prevention. J. Clin. Oncol. 23, 1636–1643 (2005).
Goss, P. E. et al. Exemestane for breast-cancer prevention in postmenopausal women. N. Engl. J. Med. 364, 2381–2391 (2011).
Decensi, A., Dunn, B. K., Puntoni, M., Gennari, A. & Ford, L. G. Exemestane for breast cancer prevention: a critical shift? Cancer Discov. 2, 25–40 (2012).
Sandler, R. S. et al. A randomized trial of aspirin to prevent colorectal adenomas in patients with previous colorectal cancer. N. Engl. J. Med. 348, 883–890 (2003).
Baron, J. A. et al. A randomized trial of aspirin to prevent colorectal adenomas. N. Engl. J. Med. 348, 891–899 (2003).
Benamouzig, R. et al. Daily soluble aspirin and prevention of colorectal adenoma recurrence: one-year results of the APACC trial. Gastroenterology 125, 328–336 (2003).
Burn, J. et al. Long-term effect of aspirin on cancer risk in carriers of hereditary colorectal cancer: an analysis from the CAPP2 randomised controlled trial. Lancet 378, 2081–2087 (2011).
Rothwell, P. M. et al. Effect of daily aspirin on long-term risk of death due to cancer: analysis of individual patient data from randomised trials. Lancet 377, 31–41 (2011).
Rothwell, P. M. et al. Long-term effect of aspirin on colorectal cancer incidence and mortality: 20-year follow-up of five randomised trials. Lancet 376, 1741–1750 (2010).
Rothwell, P. M. et al. Short-term effects of daily aspirin on cancer incidence, mortality, and non-vascular death: analysis of the time course of risks and benefits in 51 randomised controlled trials. Lancet 379, 1602–1612 (2012). The most comprehensive meta-analysis of RCTs of the impact of daily aspirin use on cancer incidence, mortality and non-vascular death.
Steinbach, G. et al. The effect of celecoxib, a cyclooxygenase-2 inhibitor, in familial adenomatous polyposis. N. Engl. J. Med. 342, 1946–1952 (2000).
Arber, N. et al. Celecoxib for the prevention of colorectal adenomatous polyps. N. Engl. J. Med. 355, 885–895 (2006).
Bertagnolli, M. M. et al. Celecoxib for the prevention of sporadic colorectal adenomas. N. Engl. J. Med. 355, 873–884 (2006). One of the first studies to show that the celecoxib had both cancer preventive and adverse cardiovascular effects.
Bresalier, R. S. et al. Cardiovascular events associated with rofecoxib in a colorectal adenoma chemoprevention trial. N. Engl. J. Med. 352, 1092–1102 (2005).
Kerr, D. J. et al. Rofecoxib and cardiovascular adverse events in adjuvant treatment of colorectal cancer. N. Engl. J. Med. 357, 360–369 (2007).
Solomon, D. H. et al. Cardiovascular outcomes in new users of coxibs and nonsteroidal antiinflammatory drugs: high-risk subgroups and time course of risk. Arthritis Rheum. 54, 1378–1389 (2006).
Meyskens, F. L. Jr et al. Difluoromethylornithine plus sulindac for the prevention of sporadic colorectal adenomas: a randomized placebo-controlled, double-blind trial. Cancer Prev. Res. (Phila) 1, 32–38 (2008).
Thompson, I. M. et al. The influence of finasteride on the development of prostate cancer. N. Engl. J. Med. 349, 215–224 (2003).
Andriole, G. L. et al. Effect of dutasteride on the risk of prostate cancer. N. Engl. J. Med. 362, 1192–1202 (2010). This paper presented the results of an RCT of dutasteride showing that it reduced the risk of prostate cancer.
Scardino, P. T. The prevention of prostate cancer--the dilemma continues. N. Engl. J. Med. 349, 297–299 (2003).
Walsh, P. C. Chemoprevention of prostate cancer. N. Engl. J. Med. 362, 1237–1238 (2010).
Hulin-Curtis, S. L., Petit, D., Figg, W. D., Hsing, A. W. & Reichardt, J. K. Finasteride metabolism and pharmacogenetics: new approaches to personalized prevention of prostate cancer. Future Oncol. 6, 1897–1913 (2010).
Parsons, T. J., Power, C. & Manor, O. Physical activity, television viewing and body mass index: a cross-sectional analysis from childhood to adulthood in the 1958 British cohort. Int. J. Obes (Lond.) 29, 1212–1221 (2005).
Fisher, B. et al. Tamoxifen for prevention of breast cancer: report of the National Surgical Adjuvant Breast and Bowel Project P-1 Study. J. Natl Cancer Inst. 90, 1371–1388 (1998).
Waters, E. A., Cronin, K. A., Graubard, B. I., Han, P. K. & Freedman, A. N. Prevalence of tamoxifen use for breast cancer chemoprevention among U.S. women. Cancer Epidemiol. Biomarkers Prev. 19, 443–446 (2010).
Dreyfuss, J. H. Tamoxifen infrequently used by women at risk for breast cancer. CA Cancer J. Clin. 60, 204–206 (2010).
Sample, D. et al. A dose-finding study of aspirin for chemoprevention utilizing rectal mucosal prostaglandin E(2) levels as a biomarker. Cancer Epidemiol. Biomarkers Prev. 11, 275–279 (2002).
U. S. Preventive Services Task Force. Aspirin for the prevention of cardiovascular disease: U.S. Preventive Services Task Force recommendation statement. Ann. Intern. Med. 150, 396–404 (2009).
Schiller, J. T. & Lowy, D. R. Vaccines to prevent infections by oncoviruses. Annu. Rev. Microbiol. 64, 23–41 (2010). One of the most comprehensive reviews of the state of vaccine research against oncoviruses, with examples from the past, and a look at the future.
Lowy, D. R., Solomon, D., Hildesheim, A., Schiller, J. T. & Schiffman, M. Human papillomavirus infection and the primary and secondary prevention of cervical cancer. Cancer 113, 1980–1993 (2008).
Kim, J. J. Focus on research: weighing the benefits and costs of HPV vaccination of young men. N. Engl. J. Med. 364, 393–395 (2011).
Gillison, M. L. et al. Prevalence of oral HPV infection in the United States, 2009–2010. JAMA 307, 693–703 (2012).
Kim, J. J. Targeted human papillomavirus vaccination of men who have sex with men in the USA: a cost-effectiveness modelling analysis. Lancet Infect. Dis. 10, 845–852 (2010).
Marquez, J. P., Rivera, R., Kang, K. H., Gardner, M. B. & Torres, J. V. Human papillomavirus immunogen that provides protective tumor immunity and induces tumor regression. Viral Immunol. 25, 141–152 (2012).
Centers for Disease Control and Prevention. Genital HPV Infection−Fact Sheet. (Centers for Disease Control and Prevention, 2012).
Dunne, E. F. et al. Prevalence of HPV infection among females in the United States. JAMA 297, 813–819 (2007).
Weiner, L. M., Surana, R. & Murray, J. Vaccine prevention of cancer: can endogenous antigens be targeted? Cancer Prev. Res. 3, 410–415 (2010).
Disis, M. L., Bernhard, H. & Jaffee, E. M. Use of tumour-responsive T cells as cancer treatment. Lancet 373, 673–683 (2009).
Beatty, P. L., Narayanan, S., Gariepy, J., Ranganathan, S. & Finn, O. J. Vaccine against MUC1 antigen expressed in inflammatory bowel disease and cancer lessens colonic inflammation and prevents progression to colitis-associated colon cancer. Cancer Prev. Res. 3, 438–446 (2010).
Gulley, J. L. et al. Pilot study of vaccination with recombinant CEA-MUC-1-TRICOM poxviral-based vaccines in patients with metastatic carcinoma. Clin. Cancer Res. 14, 3060–3069 (2008).
Moingeon, P. Recombinant cancer vaccines based on viral vectors. Dev. Biol. 116, 117–122; discussion 133–143 (2004).
Schlom, J. & Hodge, J. W. The diversity of T-cell co-stimulation in the induction of antitumor immunity. Immunol. Rev. 170, 73–84 (1999).
van Seters, M. et al. Treatment of vulvar intraepithelial neoplasia with topical imiquimod. N. Engl. J. Med. 358, 1465–1473 (2008).
Narayan, R. et al. Immunomodulation by imiquimod in patients with high-risk primary melanoma. J. Invest. Dermatol. 132, 163–169 (2012).
Triozzi, P. L., Aldrich, W. & Ponnazhagan, S. Inhibition and promotion of tumor growth with adeno-associated virus carcinoembryonic antigen vaccine and Toll-like receptor agonists. Cancer Gene Ther. 18, 850–858 (2011).
Bhattacharyya, S. et al. Toll-like receptor 4 mediates induction of the Bcl10-NFκB-interleukin-8 inflammatory pathway by carrageenan in human intestinal epithelial cells. J. Biol. Chem. 283, 10550–10558 (2008).
Tsuji, R. F. et al. Suppression of allergic reaction by lambda-carrageenan: toll-like receptor 4/MyD88-dependent and -independent modulation of immunity. Clin. Exp. Allergy 33, 249–258 (2003).
Buck, C. B. et al. Carrageenan is a potent inhibitor of papillomavirus infection. PLoS Pathog. 2, e69 (2006).
Marais, D. et al. in 26th International Papillomavirus Conference & Clinical and Public Health Workshops - Sharing Knowledge for Global Health Paper P-604 (Palais des Congres de Montreal, Canada, 2010).
Brausi, M. et al. A review of current guidelines and best practice recommendations for the management of nonmuscle invasive bladder cancer by the International Bladder Cancer Group. J. Urol. 186, 2158–2167 (2011).
Kakiashvili, D. M. et al. Long-term follow-up of T1 high-grade bladder cancer after intravesical bacille Calmette-Guerin treatment. BJU Int. 107, 540–546 (2011).
Zuiverloon, T. C. et al. Markers predicting response to bacillus Calmette-Guerin immunotherapy in high-risk bladder cancer patients: a systematic review. Eur. Urol. 61, 128–145 (2012).
Ribas, A. Tumor immunotherapy directed at PD-1. N. Engl. J. Med. 366, 2517–2519 (2012).
Dunn, B. K., Jegalian, K. & Greenwald, P. Biomarkers for early detection and as surrogate endpoints in cancer prevention trials: issues and opportunities. Recent Results Cancer Res. 188, 21–47 (2011). A comprehensive review of the types of biomarkers used in cancer prevention trials, and possible avenues of research for the future.
Boyd, N. F., Martin, L. J., Yaffe, M. J. & Minkin, S. Mammographic density and breast cancer risk: current understanding and future prospects. Breast Cancer Res. 13, 223 (2011).
Dunn, B. K., Wagner, P. D., Anderson, D. & Greenwald, P. Molecular markers for early detection. Semin. Oncol. 37, 224–242 (2010).
Kelley, R. K. & Venook, A. P. Prognostic and predictive markers in stage II colon cancer: is there a role for gene expression profiling? Clin. Colorectal Cancer 10, 73–80 (2011).
Agendia. MammaPrint Provides Individualized Metastasis Risk Assessment for Your Breast Cancer Patients. (Agendia, 2011).
Buyse, M. et al. Validation and clinical utility of a 70-gene prognostic signature for women with node-negative breast cancer. J. Natl Cancer Inst. 98, 1183–1192 (2006).
Cummings, S. R. et al. Lasofoxifene in postmenopausal women with osteoporosis. N. Engl. J. Med. 362, 686–696 (2010).
LaCroix, A. Z. et al. Breast cancer incidence in the randomized PEARL trial of lasofoxifene in postmenopausal osteoporotic women. J. Natl Cancer Inst. 102, 1706–1715 (2010).
Cummings, S. R. et al. Arzoxifene for prevention of fractures and invasive breast cancer in postmenopausal women. J. Bone Miner. Res. 26, 397–404 (2011).
Cuzick, J. I.B.I. S. II: a breast cancer prevention trial in postmenopausal women using the aromatase inhibitor anastrozole. Expert Rev. Anticancer Ther. 8, 1377–1385 (2008).
Cuzick, J. et al. Tamoxifen-induced reduction in mammographic density and breast cancer risk reduction: a nested case-control study. J. Natl Cancer Inst. 103, 744–752 (2011).
Kim, J. et al. Breast density change as a predictive surrogate for response to adjuvant endocrine therapy in hormone receptor positive breast cancer. Breast Cancer Res. 14, R102 (2012).
Eng-Wong, J. et al. Effect of raloxifene on mammographic density and breast magnetic resonance imaging in premenopausal women at increased risk for breast cancer. Cancer Epidemiol. Biomarkers Prev. 17, 1696–1701 (2008).
Welch, H. G. & Black, W. C. Overdiagnosis in cancer. J. Natl Cancer Inst. 102, 605–613 (2010).
Reid, B. J., Li, X., Galipeau, P. C. & Vaughan, T. L. Barrett's oesophagus and oesophageal adenocarcinoma: time for a new synthesis. Nature Rev. Cancer 10, 87–101 (2010).
Fisher, B. et al. Tamoxifen for the prevention of breast cancer: current status of the National Surgical Adjuvant Breast and Bowel Project P-1 study. J. Natl Cancer Inst. 97, 1652–1662 (2005).
The Women's Health Initiative Study Group. Design of the Women's Health Initiative clinical trial and observational study. Control. Clin. Trials 19, 61–109 (1998).
Steele, V. E. & Lubet, R. A. The use of animal models for cancer chemoprevention drug development. Semin. Oncol. 37, 327–338 (2010).
Nelson, H. D. et al. Systematic review: comparative effectiveness of medications to reduce risk for primary breast cancer. Ann. Intern. Med. 151, 703–715 (2009).
Visvanathan, K. et al. American society of clinical oncology clinical practice guideline update on the use of pharmacologic interventions including tamoxifen, raloxifene, and aromatase inhibition for breast cancer risk reduction. J. Clin. Oncol. 27, 3235–3258 (2009).
Ravdin, P. M. The lack, need, and opportunities for decision-making and informational tools to educate primary-care physicians and women about breast cancer chemoprevention. Cancer Prev. Res. 3, 686–688 (2010).
Ropka, M. E., Keim, J. & Philbrick, J. T. Patient decisions about breast cancer chemoprevention: a systematic review and meta-analysis. J. Clin. Oncol. 28, 3090–3095 (2010).
Moyer, V.A. & U.S. Preventive Services Task Force. Screening for Prostate Cancer: U.S. Preventive Services Task Force Recommendation Statement. Ann. Intern. Med. 157, 120–134 (2012).
Marshall, E. Public health. Brawling over mammography. Science 327, 936–938 (2010).
U. S. Preventive Services Task Force. Screening for breast cancer: U.S. Preventive Services Task Force recommendation statement. Ann. Intern. Med. 151, 716–726 (2009).
National Lung Screening Trial Research Team et al. Reduced lung-cancer mortality with low-dose computed tomographic screening. N. Engl. J. Med. 365, 395–409 (2011). Results of one of the largest lung cancer screening trials that showed that screening with low dose CT reduces mortality from lung cancer.
U.S. Preventive Services Task Force. Guide to Clinical Preventive Services, 2010–2011. Section 2: Recommendations for Adults. (Agency for Healthcare Research and Quality, 2010).
Patel, V. B., Misra, S., Patel, B. B. & Majumdar, A. P. Colorectal cancer: chemopreventive role of curcumin and resveratrol. Nutr. Cancer 62, 958–967 (2010).
Dahirel, V. et al. Coordinate linkage of HIV evolution reveals regions of immunological vulnerability. Proc. Natl Acad. Sci. USA 108, 11530–11535 (2011).
Lok, A. S. et al. Preliminary study of two antiviral agents for hepatitis C genotype 1. N. Engl. J. Med. 366, 216–224 (2012).
Ward, J. W., Valdiserri, R. O. & Koh, H. K. Hepatitis C virus prevention, care, and treatment: from policy to practice. Clin. Infect. Dis. 55, S58–S63 (2012).
Zeng, Q. et al. Development of a DNA vaccine targeting Merkel cell polyomavirus. Vaccine 30, 1322–1329 (2012).
Baxevanis, C. N., Voutsas, I. F., Gritzapis, A. D., Perez, S. A. & Papamichail, M. HER-2/neu as a target for cancer vaccines. Immunotherapy 2, 213–226 (2010).
Benavides, L. C. et al. Comparison of different HER2/neu vaccines in adjuvant breast cancer trials: implications for dosing of peptide vaccines. Expert Rev. Vaccines 10, 201–210 (2011).
Park, K. H. et al. Insulin-like growth factor-binding protein-2 is a target for the immunomodulation of breast cancer. Cancer Res. 68, 8400–8409 (2008).
Lu, J. & Celis, E. Use of two predictive algorithms of the world wide web for the identification of tumor-reactive T-cell epitopes. Cancer Res. 60, 5223–5227 (2000).
Gnjatic, S. et al. NY-ESO-1: review of an immunogenic tumor antigen. Adv. Cancer Res. 95, 1–30 (2006).
Cany, J. et al. AFP-specific immunotherapy impairs growth of autochthonous hepatocellular carcinoma in mice. J. Hepatol. 54, 115–121 (2011).
Yuan, W., Xia, G., Zhao, C., Sui, C. & Ma, J. Anti-idiotypic single chain mimicking CA125 linked with tuftsin provides protective immunity against ovarian cancer in mice. Mol. Med. Rep. 5, 388–394 (2012).
Beatty, P., Ranganathan, S. & Finn, O. J. Prevention of colitis-associated colon cancer using a vaccine to target abnormal expression of the MUC1 tumor antigen. Oncoimmunology 1, 263–270 (2012).
Meek, D. W. & Marcar, L. MAGE-A antigens as targets in tumour therapy. Cancer Lett. 324, 126–132 (2012).
Carbone, D. P. et al. Immunization with mutant p53- and K-ras-derived peptides in cancer patients: immune response and clinical outcome. J. Clin. Oncol. 23, 5099–5107 (2005).
Wolfel, T. et al. A p16INK4a-insensitive CDK4 mutant targeted by cytolytic T lymphocytes in a human melanoma. Science 269, 1281–1284 (1995).
Robbins, P. F. et al. A mutated β-catenin gene encodes a melanoma-specific antigen recognized by tumor infiltrating lymphocytes. J. Exp. Med. 183, 1185–1192 (1996).
Coulie, P. G. et al. A mutated intron sequence codes for an antigenic peptide recognized by cytolytic T lymphocytes on a human melanoma. Proc. Natl Acad. Sci. USA 92, 7976–7980 (1995).
Bosch, G. J., Joosten, A. M., Kessler, J. H., Melief, C. J. & Leeksma, O. C. Recognition of BCR-ABL positive leukemic blasts by human CD4+ T cells elicited by primary in vitro immunization with a BCR-ABL breakpoint peptide. Blood 88, 3522–3527 (1996).
Mandruzzato, S., Brasseur, F., Andry, G., Boon, T. & van der Bruggen, P. A. CASP-8 mutation recognized by cytolytic T lymphocytes on a human head and neck carcinoma. J. Exp. Med. 186, 785–793 (1997).
Acknowledgements
The authors are indebted to E. Richmond, A. Ryan and D. Anderson for contributions to the writing and content of this manuscript.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Competing interests
The authors declare no competing financial interests.
Related links
Glossary
- Biologically active food components
-
(BFCs). Found in foods or nutrients; responsible for increasing or decreasing the risk of cancer.
- The Cancer Genome Atlas
-
(TCGA). Catalogues genetic mutations that are found in cancers.
- Overdiagnosis
-
A diagnosis of cancerous lesions the clinical significance of which is undetermined.
- Underdiagnosis
-
The failure to diagnose cancerous lesions that will ultimately recur, metastasize or lead to death.
Rights and permissions
About this article
Cite this article
Umar, A., Dunn, B. & Greenwald, P. Future directions in cancer prevention. Nat Rev Cancer 12, 835–848 (2012). https://doi.org/10.1038/nrc3397
Published:
Issue Date:
DOI: https://doi.org/10.1038/nrc3397
This article is cited by
-
The potential preventive effect of dietary phytochemicals In Vivo
BDJ Open (2023)
-
Localization, tissue biology and T cell state — implications for cancer immunotherapy
Nature Reviews Immunology (2023)
-
Cholesterol and breast cancer risk: a cohort study using health insurance claims and health checkup databases
Breast Cancer Research and Treatment (2023)
-
In vivo and in vitro inhibition of SCLC by combining dual cancer-specific recombinant adenovirus with Etoposide
Journal of Cancer Research and Clinical Oncology (2022)
-
Functional metabolome profiling may improve individual outcomes in colorectal cancer management implementing concepts of predictive, preventive, and personalized medical approach
EPMA Journal (2022)
